Article Text

Statistics from Altmetric.com
The idea that “we are what we eat” has motivated numerous ever-changing food fads, diet books and dietary guidelines over the past 200 years, often in the absence of firm scientific evidence to support potential health benefits. In addition, some foods, such as chocolate, are often suspected of being bad for us, probably because they taste so good.
In this edition of Heart, Kwok and colleagues (see page 1279) examined the association between chocolate consumption and risk of cardiovascular disease (CVD) based on dietary histories in over 20 thousand men and women in the European Prospective Investigation into Cancer-Norfolk (EPIC-Norfolk) study. At a median followup of 11.9 years, coronary heart disease was present in 9.7% of patients in the highest, compared to 13.8% of patients in the lowest, quintile of chocolate consumption Similarly, the rate for stroke was 3.1% in the highest, compared to 5.4% in the lowest quintile. With multivariate adjustment, the hazard ratio was 0.88 (95% CI 0.77 to 1.01) for those in the top quintile of chocolate consumption (16–99 g/day) versus those who ate no chocolate. This trend was confirmed in a propensity score matched analysis and in a meta-analysis of nine previous publications (figure 1).
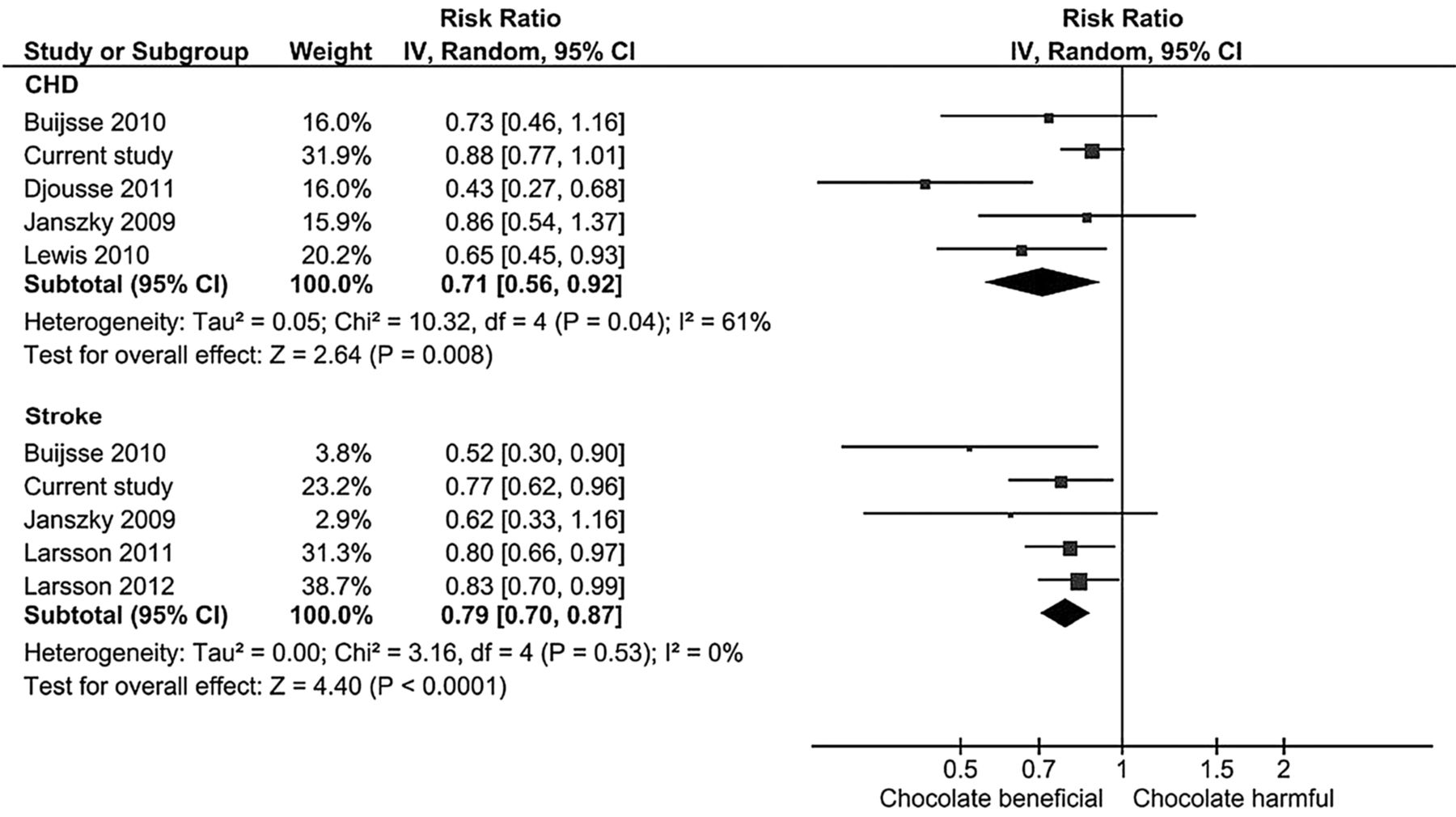
Meta-analysis risk of the association between chocolate consumption and risk of coronary heart disease (CHD) and stroke.
Is it biologically plausible that chocolate might have beneficial (or at least not harmful) effects in terms of cardiovasculare disease? Chocolate contains flavonoid anti-oxidants with proposed mechanisms including improved endothelial function, a more favorable balance between serum high (HDL) and low-density lipoprotein (LDL) cholesterol concentrations, reduced LDL oxidation, and decreased inflammation. However, despite biological plausibility and convincing association studies, we need to be cautious in concluding that higher chocolate intake does not have adverse cardiovascular effects. First, this might be an example of “reverse causation” – people who report higher chocolate intake have fewer cardiovascular risk factors and engage in a healthier life-style, rather than the other way around. Second, we need to be sure that eating more chocolate does not have unanticipated secondary effects, such as increased caloric intake and weight gain. Even so, this study provides reassurance that continued chocolate consumption by our patients (and ourselves) has not been shown to increase the risk of cardiovascular events.
Obstructive sleep apnea (OSA) is associated with increased CVD risk, yet remains underdiagnosed in outpatient cardiology settings. Given the increasing prevalence of obesity, a risk factor of OSA, the prevalence of OSA is increasing as well. Drager and colleagues (see page 1288) found that over 50% of outpatients in five different cardiac specialty clinics in Sao Paulo, Brazil were at high risk for OSA based on a standard questionnaire, but only 3.1% had a previous diagnosis of OSA. Sleep studies in a randomly selected subset of this population documented OSA in 66% of patients (table 1).
Characteristics of the studied population
In an accompanying editorial, Fuchs and Martinez (see page 1261) remind us that “Sleep-related breathing disorders are highly prevalent in patients with cardiovascular disease. Central sleep apnoea (CSA) occurs mostly in patients with heart failure. Obstructive sleep apnoea (OSA) may occur in up to one third of the general population and in 71% of patients with resistant hypertension”. They also remind us that this common condition is a treatable risk factor for hypertension, heart failure, arrhythmias and stroke. Further they suggest that that OSA education be included in cardiology training and at cardiology meetings because “the use of proven therapies for OSA would reduce its cardiovascular consequences”.
Identification of patients at risk of atrial fibrillation might allow earlier detection, treatment, and prevention of complications. Tiwari and colleagues (see page 1302) hypothesized, that evidence of diastolic dysfunction on echocardiography would be predictive of incident atrial fibrillation (AF). In 2406 subjects with a mean age of 62.6 years, AF occurred in 462 (19%) over 16 years of followup for an incidence rate of 12.6 per 1000 person-years. On multivariable analysis, the risk of AF increased with increased left atrial (LA) size with moderate LA enlargement associated with a 60% increased risk for AF. Doppler measures of diastolic function alone were not predictive, but when adjusted for LA size abnormal mitral flow was associated with a 30% increased risk of AF (figure 2). Their video abstract can be viewed online http://heart.bmj.com/content/early/2015/05/13/heartjnl-2015-307438.full

Kaplan–Meier curves for atrial fibrillation (AF) categories of left atrial (LA) size and mitral Doppler indices combined. The Tromsø Study, 1994–2010. Group 1=LA size <2.2 cm/m2 and normal mitral Doppler indices (n=947). Group 2=LA size <2.2 cm/m2 and abnormal mitral Doppler indices (n=294). Group 3=LA size 2.2–2.79 cm/m2 and normal mitral Doppler indices (n=720). Group 4=LA size 2.2–2.79 cm/m2 and abnormal mitral Doppler indices (n=227). Group 5=LA size ≥2.8 cm/m2 and normal/abnormal mitral Doppler indices (n=92).
Although this study supports the concept that long-standing diastolic dysfunction predisposes patients to AF, Delgado and Bax (see page 1263) suggest in their editorial commentary that advanced imaging approaches may provide further insights beyond simple measures of LA size or LV diastolic filling. For example, “Echocardiographic tissue Doppler imaging and speckle tracking permit the assessment of total atrial activation time and active deformation of the atrial myocardium and the reservoir function, respectively”. In addition, “Late gadolinium contrast-enhanced magnetic resonance techniques permit direct quantification of diffuse and focal fibrosis of the atrial wall”. They conclude that further research is needed “to refine the risk stratification of individuals who are at risk of developing AF and to develop effective interventions that reduce the global burden of AF”.
The Education in Heart article in this issue (see page 1332) focuses on myocarditis. Sections include pathogenesis, clinical presentation, imaging and biomarker findings and the current diagnostic criteria for myocarditis, as well as a flow chart for patient evaluation and therapy (figure 3).

{kind=link}
{kind=link}
{kind=link}
Diagnostic work-up and aetiology-based management in myocarditis according to the European Society of Cardiology 2013 Task Force criteria. Aab, cardiac autoantibody, EMB, endomyocardial biopsy.
The Image challenge case (see page 1317) in this issue shows an unusual echocardiographic finding in a young man presenting with dyspnea and a murmur. Be sure to look at the online videos before you try to make the diagnosis.
Linked Articles
- Education in Heart
- Arrhythmias and sudden death
- Editorial
- Editorial
- Cardiac risk factors and prevention
- Image challenge
- Cardiac risk factors and prevention