Article Text

Statistics from Altmetric.com
The increasing prevalence of aortic stenosis (AS) in our ageing population and clinical trials demonstrating the benefits of transcatheter valve implantation for severe symptomatic AS have focused attention on this disease in recent years. Yet, despite clear recommendations from professional societies, it remains unclear whether all patients receive timely and appropriate treatment. To address this concern, Frey and colleagues1 looked at data from the Study to Improve Outcomes in Aortic Stenosis (IMPULSE) registry which included 2171 adults with severe AS at 23 tertiary care hospitals in 9 European countries, including the UK. Patient mean age was 78 years, 48% were women and 27% had a left ventricular ejection fraction less than 50%. Over 80% of these patients were symptomatic, but only 76% of those with severe symptomatic AS were treated appropriately with aortic valve replacement (AVR), most often by the transcatheter approach (figure 1). Of even more concern, among asymptomatic patients with an indication for AVR, 42% (22/52) were not treated, whereas AVR was performed in 36% (123/339) of asymptomatic AS patients with no established indication.

Flowchart of the population and management according to functional status. AS, aortic stenosis; AVR, aortic valve replacement.
In the accompanying editorial, Chambers2 discusses the study design and comments that ‘the IMPULSE registry is a useful ‘snapshot’ of current care and reminds us that the key to improving care for patients with valve disease is to develop a comprehensive valve service at three levels: 1. the detection of valve disease; 2. referral of patients with moderate or severe disease to a specialist valve clinic to plan management and follow-up until intervention is indicated and 3. intervention in a heart valve centre with recognised performance standards’ (figure 2).
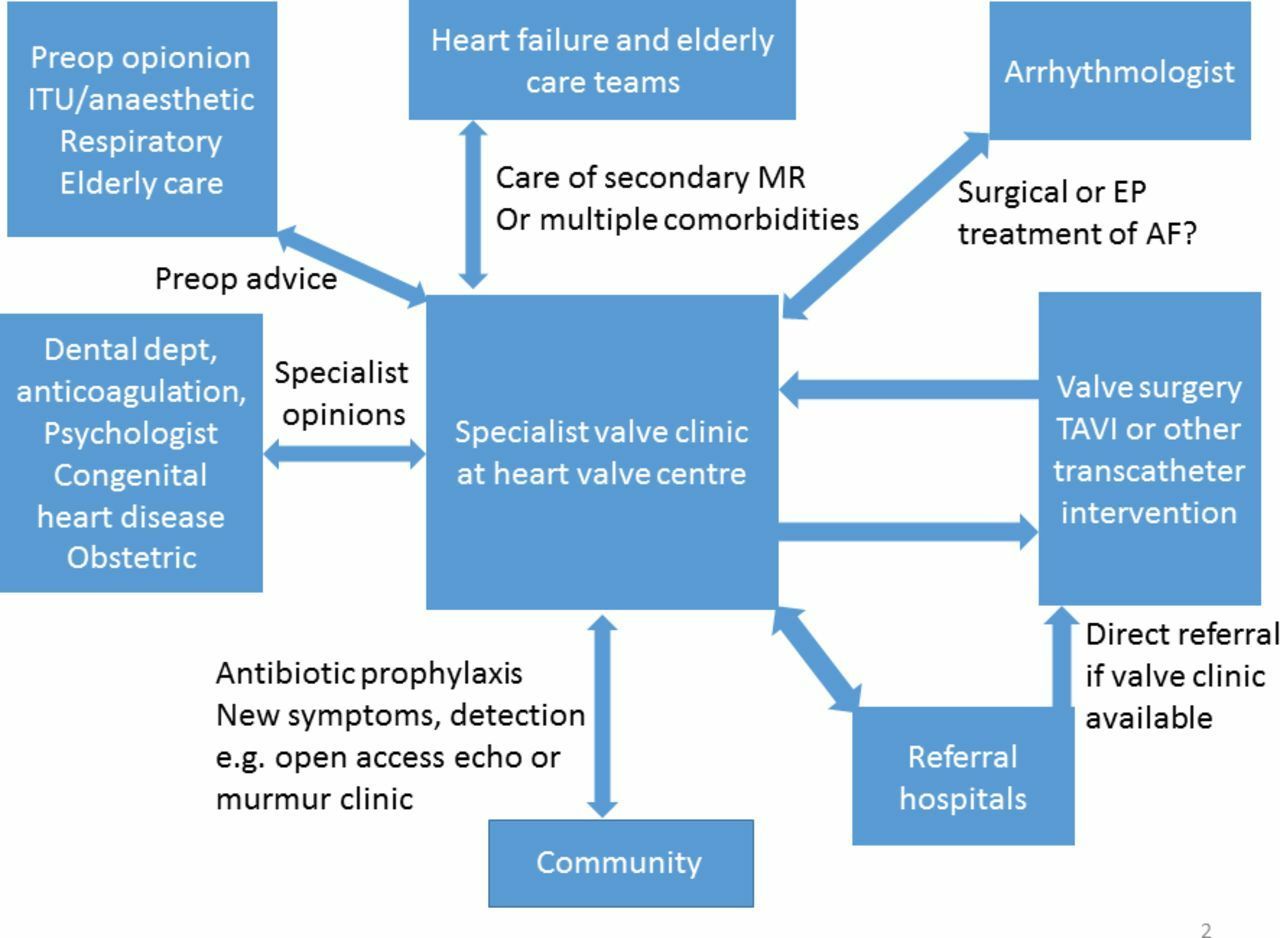
The valve disease network. AF, atrial fibrillation; EP, electrophysiologic; ITU, intensive treatment unit; TAVI, transcatheter aortic valve implantation.
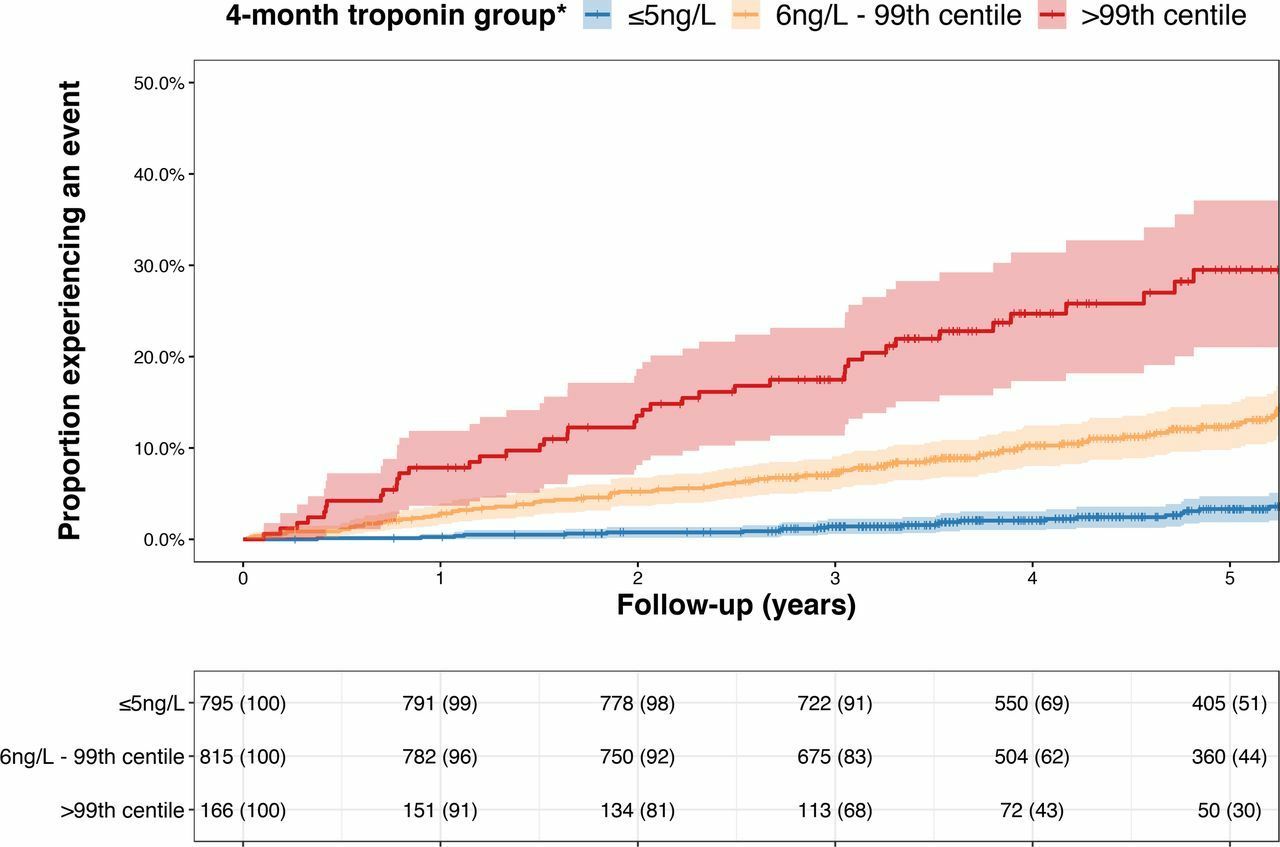
High-sensitivity cardiac troponin testing is integral for diagnosis of acute coronary syndromes (ACSs) but the potential value of troponin measurements months to years after the acute event has not been studied. In this issue of Heart, Adamson and colleagues3 found that troponin concentrations 4 months after an ACS were an independent predictor of cardiovascular death, with an HR of 1.4 (CI 1.3 to 1.5) per doubling of the serum level (figure 3). Risk was highest in patients who had increasing troponin levels at 12 months and in those with a 4-month level > 99th percentile compared those with a troponin ≤5 ng/L (29.5% (49/166) vs 4.3% (34/795); adjusted HR 4.9, 95% CI 3.8 to 23.7).

Cumulative incidence of cardiovascular death according to 4-month troponin concentration cumulative event curves for cardiovascular death according to troponin concentrations determined at the 4-month visit. Each cross-hair indicates when a subject is censored from further follow-up. The number at risk (% in group remaining) for each yearly interval is given for each troponin group. Follow-up begins from date of 4-month visit. *For descriptive purposes, troponin concentrations have been rounded to nearest integer value. Therefore ≤5 ng/L includes all patients <5.5 ng/L.
In a provocative editorial, Kavask and Devereaux4 commend the authors for ‘undertaking and executing this study, laying the foundation for a possible testing protocol with high-sensitivity cardiac troponin following ACS.’ However, in the context of varying definitions, methods and variability in high-sensitivity troponin testing, they point out that ‘a question lingers as to whether current laboratory practices can provide accurate and reproducible results around the thresholds of such a framework.’ Based on a simulation using their own quality control data for troponin measurements, they suggest ‘that the percent change criterion as suggested by Adamson and colleagues3 would be appropriate for concentrations near the 99th percentile but not at the lower concentration limit of 6 ng/L, where absolute changes (rather than percent) in high-sensitivity cardiac troponin at this low concentration range have demonstrated clinical utility.’
The importance of reporting and analysing sex difference in cardiovascular outcomes is discussed in detail in a review article and tutorial5 by Woodward in this issue of Heart. Readers will find that this article provides a clear rationale for the optimal approaches to analysing sex differences with examples shown in figures and tables. Clinical researchers will find this article is a practical guide to study design and data analysis with a table (table 1) of specific recommendations for reporting study results.
Recommendations for reporting sex differences in cardiovascular associations
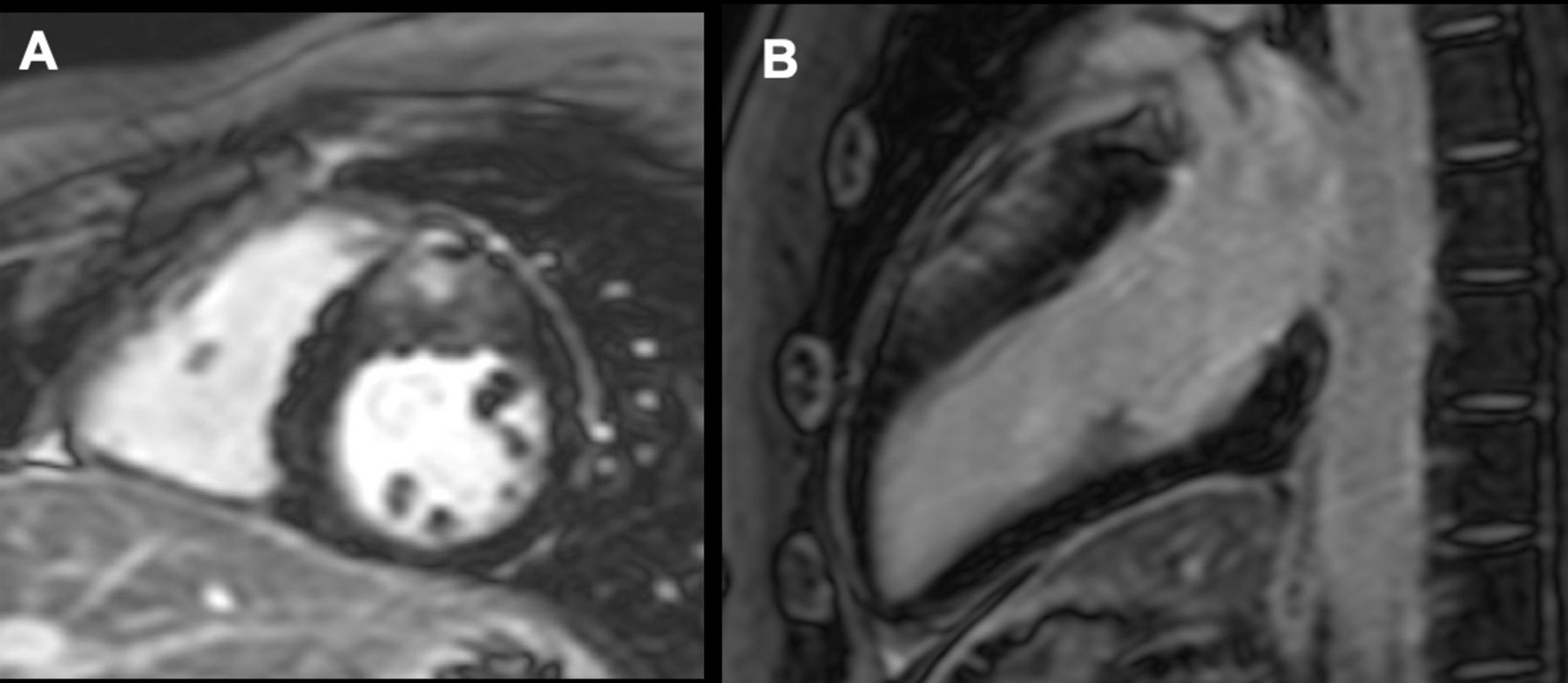
Our Education in Heart article reviews clinical indications for cardiovascular magnetic resonance (CMR) imaging6 with tables highlighting the strengths of different imaging techniques and detailing CMR findings that differentiate restrictive and hypertrophic cardiomyopathies (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient with hypertrophic cardiomyopathy with asymmetric anterior and anteroseptal hypertrophy and an associated non-ischaemic diffuse scar in the area of maximal hypertrophy (A, B).
In our Cochrane Corner series, short summaries of recent Cochrane Reviews relevant to clinical cardiology, Stranges and colleagues7 address the question ‘Does the Mediterranean-style diet help in the prevention of cardiovascular disease?’ They conclude: ‘At the present time, there is no definitive trial evidence regarding the effects of a Mediterranean-style diet on clinical endpoints for both the primary and secondary prevention of major CVD. Overall, the available trial evidence is promising (though not conclusive) and generally supportive of favourable effects of the Mediterranean-style diet on individual cardiometabolic risk factors in primary prevention studies, and potentially also on clinical endpoints such as stroke. Several ongoing trials, particularly those reporting clinical endpoints in secondary prevention, will add to the evidence base.’
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.