Article Text

Abstract
Objective Distinguishing early dilated cardiomyopathy (DCM) from physiological left ventricular (LV) dilatation with LV ejection fraction <55% in athletes (grey zone) is challenging. We evaluated the role of a cascade of investigations to differentiate these two entities.
Methods Thirty-five asymptomatic active males with DCM, 25 male athletes in the ‘grey zone’ and 24 male athletes with normal LV ejection fraction underwent N-terminal pro-brain natriuretic peptide (NT-proBNP) measurement, ECG and exercise echocardiography. Grey-zone athletes and patients with DCM underwent cardiovascular magnetic resonance (CMR) and Holter monitoring.
Results Larger LV cavity dimensions and lower LV ejection fraction were the only differences between grey-zone and control athletes. None of the grey-zone athletes had abnormal NT-proBNP, increased ectopic burden/complex arrhythmias or pathological late gadolinium enhancement on CMR. These features were also absent in 71%, 71% and 50% of patients with DCM, respectively. 95% of grey-zone athletes and 60% of patients with DCM had normal ECG. During exercise echocardiography, 96% grey-zone athletes increased LV ejection fraction by >11% from baseline to peak exercise compared with 23% of patients with DCM (p<0.0001). Peak LV ejection fraction was >63% in 92% grey-zone athletes compared with 17% patients with DCM (p<0.0001). Failure to increase LV ejection fraction >11% from baseline to peak exercise or achieve a peak LV ejection fraction >63% had sensitivity of 77% and 83%, respectively, and specificity of 96% and 92%, respectively, for predicting DCM.
Conclusion Comprehensive assessment using a cascade of routine investigations revealed that exercise stress echocardiography has the greatest discriminatory value in differentiating between grey-zone athletes and asymptomatic patients with DCM. Our findings require validation in larger studies.
- idiopathic dilated cardiomyopathy
Statistics from Altmetric.com
Introduction
Dilated cardiomyopathy (DCM) is a rare but recognised cause of sudden cardiac death in athletes.1 A small proportion of endurance athletes show enlarged left ventricular (LV) cavities with borderline/low left ventricular ejection fraction (LVEF)2 which overlaps with the phenotypic expression of morphologically mild DCM. Differentiation between these entities is an important focus of the sports cardiology and imaging societies. Expert opinion suggests that comprehensive assessments including the ECG, advanced imaging such as exercise stress echocardiography, two-dimensional strain imaging and the presence of late enhancement on cardiovascular magnetic resonance (CMR) imaging are necessary to differentiate these two entities3 4; however, data regarding utility of such investigations in this context is limited. We sought to evaluate the role of conventional investigations to differentiate between physiological adaptation in healthy athletes with LV dilatation and LVEF <55% (grey zone) and active asymptomatic individuals with DCM.
Methods
The data, analytical methods and study materials will not be made available to other researchers for the purpose of reproducing the results or replicating the procedure. Researchers interested in the data, methods or analysis can contact the corresponding author for more information. Patients and public were not involved in the design, conduct, reporting or dissemination plans of our research.
Study subjects
Patients with DCM
Asymptomatic male patients with non-ischaemic DCM were recruited from two tertiary cardiomyopathy centres in London. DCM was defined as systolic impairment in association with LV enlargement (either LV end-diastolic dimension >58 mm or LV end-diastolic volume of >150 mL, equating to 2 SD above the mean, as per the American Society of Echocardiography).5 LV impairment was defined as LVEF <55%. Exclusion criteria included ischaemic heart disease, hypertension, valvular disease, LVEF <35% and poor echocardiographic windows. In individuals who exercised more than 5 hours of exercise per week, DCM was confirmed by the presence of DCM in a first-degree relative, remodelled severe LV systolic dysfunction or late enhancement on CMR. Thirty-five individuals who fulfilled these criteria agreed to participate in the study.
Healthy athletes with LV dilatation and LVEF <55% (grey zone)
In the UK, the charity Cardiac Risk in the Young (CRY) subsidises preparticipation cardiovascular evaluations for elite professional and national sporting organisations. Over the period 2015–2017, 8006 athletes were evaluated by CRY. Additionally, the sports cardiology unit at St George’s Hospital is a quaternary referral centre for athletes from centres throughout the country. Twenty-five asymptomatic athletes with phenotypic features resembling DCM were recruited from these sources. The grey zone was defined as an athlete with LV enlargement and borderline ejection fraction (<55%) who exercised for ≥8 hours per week. Athletes with a family history of DCM were excluded.
Athlete controls
A control cohort of 24 healthy asymptomatic male athletes with normal LV geometry matched to athletes with an increased LV cavity and LVEF <55% for age and sporting discipline were recruited through the CRY screening programme.
Study protocol
Participants underwent health questionnaire, N-terminal pro-brain natriuretic peptide (NT-proBNP), 12-lead ECG, baseline and exercise echocardiogram and cardiopulmonary exercise testing (CPET). Beta-blockade was held for 48 hours prior to exercise testing. Grey-zone athletes and patients with DCM also underwent a CMR and 24-hour Holter monitor.
Health questionnaire
The health questionnaire contained questions regarding cardiovascular symptoms, family history and exercise activity.
NT-proBNP
Blood samples for NT-proBNP were obtained from participants during resting conditions. Analysis was performed within 2 hours of extraction at room temperature using a Cobas 8000 E602 Module Immunochemistry Analyser (Roche Diagnostics, Basel, Switzerland).
Electrocardiography
12-lead ECG was performed in the supine position in a quiet room using a GE Marquette Hellige (Milwaukee, Wisconsin, USA) ECG machine with a paper speed of 25 mm/s as described.6 ECGs were interpreted in accordance with international guidelines.7
Twenty-four-hour Holter
Twenty-four-hour ambulatory ECG monitoring was performed using Life Card CF Holters (Spacelabs Healthcare). A high ventricular ectopic burden >500 beats/24 hours8 or the presence of non-sustained ventricular tachycardia (NSVT) was considered abnormal. The presence of NSVT was defined as three or more consecutive beats of >120 ms.9
Echocardiography
Two-dimensional transthoracic echocardiography was performed by two board accredited sonographers using a commercially available, portable ultrasound system (Vivid E9, GE Healthcare, Milwaukee, Wisconsin, USA) with a 1.5–3.6 MHz phased array transducer. Conventional views were obtained and measurements made as per the American Society of Echocardiography.5 Pulsed-wave Doppler recordings were obtained to assess transmitral Doppler, and tissue Doppler imaging (TDI) was acquired at the lateral and septal mitral annulus.10 M-mode echocardiography was used to assess the tricuspid annular plane systolic excursion.
Speckle tracking imaging
Speckle tracking imaging was performed using a designated speckle tracking package (GE EchoPAC Clinical Workstation Software (Pollards Wood, UK)) to obtain global LV longitudinal strain (GLS) in the two-, three-, four-chamber views and then averaged accordingly. A normal GLS value was <−17%.5
Stress echocardiography
Exercise echocardiography was conducted on a semirecumbent cycle ergometer (Lode Angio with Echo Cardiac Stress Table, Groningen, The Netherlands) according to a ramp protocol of 20 W/min to volitional exhaustion. Standard apical, parasternal short and long-axis images and transmitral Doppler and TDI of the lateral wall were acquired at baseline and peak exercise. LV volumes and ejection fraction were calculated using the Simpson’s biplane method.5 Intravenous contrast was not required as all subjects had good endocardial definition.
Cardiopulmonary exercise testing
CPET was performed in an upright position with a COSMED E100w cycle ergometer (Rome, Italy) using a ramp protocol 20–30 W/min to volitional exhaustion. Breath-by-breath gas exchange analysis was performed using a dedicated COSMED Quark CPEX metabolic cart (Rome, Italy). Peak oxygen consumption (pVO2) was calculated in millilitre per kilogram per minute.
Cardiovascular magnetic resonance
CMR imaging was performed using methods described and analysed using semiautomated software.11 All measurements were recorded as absolute values and indexed to body surface area as per the DuBois-DuBois formula.12 Delayed enhancement images were acquired after the administration of gadolinium diethylenetriamine pentaacetate. Isolated late gadolinium enhancement (LGE) at the right ventricular insertion was not considered pathological as this is a common finding in healthy endurance athletes.8
Statistical analysis
Analyses were performed using SPSS (V.25.0, IBM). Shapiro-Wilk test and analysis of histograms were performed to assess for normality. Continuous variables are presented as mean±SD or median and IQRs. Comparison of two groups was performed by unpaired Student’s t-tests or Mann-Whitney U tests. Comparisons of more than two groups were performed by one-way analysis of variance (with Bonferroni post hoc test) or Krushal-Wallis (with Dunn’s post hoc test) test where appropriate. Categorical variables were presented as percentages and were compared using Fisher’s exact tests or χ2 test. Receiver operating characteristic (ROC) curve analysis was performed to test the sensitivity of the echocardiographic variables in predicting DCM. Athlete was considered a negative test, whereas DCM was considered a positive test. Optimal cut-off values, defined by the best compromise between sensitivity and specificity, were calculated by the Youden’s index using Medcalc 19.0.7. Inter-reader variability was assessed by intraclass correlation coefficients. Statistical significance was defined for p-values <0.05. Forward stepwise logistic regression was used. Stress echocardiographic variables with an area under the curve (AUC) >0.7 as identified by the ROC curve were included in the model.
To determine sample sizes, we estimated using a previous study of exercise radionuclide angiography which showed those with contractile reserve (representing athletes) had an increase in LVEF of 5%±6% and those with poor outcome (representing DCM) had a change of LVEF of 0±5%.13 Using these assumptions, we calculated that we needed at least 21 in each cohort to provide 80% power. To allow for a margin of error, we aimed to recruit at least 30 patients with DCM and match them for age and baseline LVEF with the grey-zone athletes (α=5%, 1-β=80%, n=21).
Results
Demographics
Patients with DCM
Patients with DCM were aged 39.5±13.4 (18–68) years. The majority (88.6%) were Caucasians. All patients were in New York Heart Association Class 1 and exercised for an average of 4 (2–8) hours per week. Twenty-four (68.8%) were on beta-blockers and 23 (65.7%) on ACE inhibitors or angiotensin II receptor blockers. Three patients (8.6%) had an implantable cardioverter-defibrillator in situ. Fifteen patients (42.9%) had familial DCM, 3 (8.6%) had anthracycline-induced DCM, 4 (11.4%) had postviral DCM and 15 (42.9%) had idiopathic DCM.
Athletes
Athletes with an enlarged LV and baseline LVEF <55% (grey-zone athletes) (32.3±10.4; range 18–58 years) and control athletes (36.7±7.7; 22–48 years) were of similar age; however, grey-zone athletes were younger than patients with DCM (p=0.035). The majority (>90%) were Caucasians. Grey-zone athletes and control athletes exercised for a mean of 14.0 (10–20) and 10 (8.5–14.75) hours per week, respectively, and participated primarily in endurance sports. Grey-zone athletes participated in cycling (n=8), endurance running (n=10), triathlon (n=3), rowing (n=3) and rugby (n=1). Control athletes competed in cycling (n=15), triathlon (n=2), endurance running (n=6) and rowing (n=1).
Electrocardiography
All participants were in sinus rhythm. Fourteen (40%) patients with DCM had an abnormal ECG (some with multiple abnormalities) compared with 2 (8.0%) grey-zone athletes and 1 (4.2%) control athlete (p=0.0007). Among the DCM cohort, four had left bundle branch block, two had pathological Q waves, two had ST-segment depression, five had T-wave inversion and four had two or more ventricular extrasystoles. None of these abnormalities were seen in either athletic cohort. Ten (28.6%) patients with DCM had an abnormal Holter of which 5 (14.3%) showed >500 ventricular extrasystoles, 2 (5.7%) revealed isolated NSVT and 3 (8.5%) had both. None of the grey-zone athletes had an abnormal Holter.
NT-proBNP
There was no significant difference in median NT-proBNP between the three groups (50 (26–262) pg/mL in the DCM group, 33.0 (23.5–57.5) pg/mL in the grey zone and 28 (17.5–42) pg/mL in the athlete controls (p=0.131)). Ten (28.6%) patients with DCM had an NT-proBNP >125 pg/mL (upper limit of normal)14 compared with none of the athletes.
Baseline echocardiography
There were no significant differences in the LV end-diastolic dimensions or ejection fraction between grey-zone athletes or patients with DCM. Both groups had a larger LV cavity compared with control athletes, but there were no differences between the groups in left atrial indexed volume or LV mass (Table 1). LA dilatation was observed in 12 (48.0%) grey-zone athletes, 16 (66.7%) control athletes and 12 (34.3%) patients with DCM. Diastolic dysfunction was noted in five patients with DCM (two grade I, two grade II and one grade III). None of the athletes had diastolic dysfunction. Both athletic cohorts showed significantly higher TDI measurements compared with patients with DCM. Lateral S′ wall was higher in both athletic groups compared with patients with DCM. All the grey-zone athletes and 28 (80.0%) patients with DCM had a lateral E′ ≥10 cm/s. Twenty (80%) grey-zone athletes and 15 (42.9%) patients with DCM had an S′ wave ≥10 cm/s.
Baseline echocardiographic characteristics
Speckle tracking imaging
Average GLS was highest in athlete controls (−17.4%±1.9%), followed by grey-zone athletes (−16.0%±2.1%) and patients with DCM (−13.6%±3.0%), p<0.0001. A significant proportion of grey-zone athletes (n=17; 68%), 14 (n=14; 58.3%) control athletes and 27 (n=27; 79.4%) patients with DCM had GLS values outside the normal range (<−17%).5
Exercise echocardiogram
All cohorts demonstrated improvement in indices of diastolic (E′) and longitudinal systolic function (S′) at peak exercise; however, the athletes showed a greater improvement in lateral S′ compared with patients with DCM (table 2). Change in LVEF ≤11% and peak LVEF ≤63% were considered the optimal ‘cut-off’ to distinguish between DCM and grey-zone athletes (table 3). All but one of the grey-zone athletes (96.0%) failed to increase LVEF >11% as did 19 (79.2%) control athletes (figure 1) compared with only 8 (22.9%) patients with DCM. All athlete controls and 23 (92.0%) grey-zone athletes achieved a peak LVEF >63% compared with only 6 (17.1%) patients with DCM (figure 2). Thirty (85.7%) patients with DCM failed to increase LVEF by >11% or achieve a peak ejection fraction >63%. Combining the inability to achieve a peak exercise LVEF >63% and a change in LVEF >11% exercise echocardiography had a sensitivity of 85.7% and specificity of 92.0%.
Stress echocardiographic characteristics

(A) Change in left ventricular ejection fraction (LVEF) from baseline to peak exercise in the healthy athletes with left ventricular (LV) dilatation and LVEF <55% (the grey zone) (left), athlete controls (centre) and individuals with morphologically mild dilated cardiomyopathy (DCM) (right). Each circle represents an individual and the horizontal line represents the mean and the 95% CIs. Almost all the athletes in both cohorts increase the LVEF by >11% compared with the DCM cohort who demonstrate a heterogeneous response. (B) The change in ejection fraction from baseline to peak exercise. The healthy athletes with LV dilatation and LVEF <55% (grey zone) are on the left, the DCM cohort on the right and the control athletes in the centre. All the athletes demonstrate an increase in LVEF compared with the patients with DCM who show a heterogeneous response.

Peak exercise left ventricular ejection fraction (LVEF). This figure shows peak exercise LVEF from baseline to peak exercise in the healthy athletes with left ventricular (LV) dilatation and LVEF <55% (grey zone) (left), control athletes (centre) and dilated cardiomyopathy (DCM) cohort (right). Each circle represents an individual and the horizontal line represents the mean and the 95% CIs. All the athlete controls and almost all the grey-zone athletes increase their LVEF to >63% from baseline to peak exercise, which is in contrast to the DCM cohort.
Receiver operator characteristic curve analysis evaluating biomarkers and structural and functional stress echocardiographic parameters to distinguish between dilated cardiomyopathy and athletic adaptation
Cardiovascular magnetic resonance
All but one patient with DCM and one athlete with a dilated LV and LVEF >55% (grey zone) underwent a CMR. Pathological LGE was observed in 17 (50.0%) patients with DCM (mid wall n=12 and subepicardial n=5) compared with none of the grey-zone athletes (online supplementary table 1).
Supplemental material
Cardiopulmonary exercise testing
There were no significant differences in cardiopulmonary parameters between either athletic group and both achieved superior results compared with patients with DCM (online supplementary table 2). A significant proportion (n=25; 71.4%) of patients with DCM had a normal pVO2 15 with seven (20%) achieving a pVO2 of >120% predicted. Of these seven, all had ventricular arrhythmias on Holter and six had the late enhancement on CMR.
Discriminating ability of echocardiographic parameters
ROC curve analysis showed peak LVEF ≤63% (AUC 0.904; p<0.0001) and change LVEF ≤11% (AUC 0.906; p<0.0001) predicted DCM with good sensitivity and excellent specificity (table 3). Stepwise logistic regression model including a change in LVEF ≤11%, peak LVEF ≤63%, peak stroke volume ≤94 mL and peak S′ ≤21 cm/s as predictors of DCM revealed that a change in LVEF ≤11% independently predicted DCM. The final model had a Nagelkerke R2 of 0.677.
Interobserver variability
Agreement between observers for the echocardiographic variables was assessed on a random sample of 40 stress echocardiograms using intraclass coefficient between the primary observer and an independent observer blinded to the initial readings and other results. The intraclass coefficients for the assessment of baseline LVEF, the difference between baseline and peak LVEF and peak LVEF were 0.734, 0.877 and 0.899, respectively.
Discussion
To our knowledge, this is the first study which has comprehensively assessed the utility of a cascade of investigations to differentiate between the athletes with an enlarged LV and LVEF <55% (grey zone) and morphologically mild DCM. Our results reveal the combination of investigations including NT-proBNP, ECG, Holter and CMR that will fail to diagnose DCM >30% of cases. Whereas NT-proBNP >125 pg/mL was highly specific for DCM, most affected active patients had normal values. The ECG has a sensitivity of 90%16 and 80%17 in hypertrophic and arrhythmogenic cardiomyopathy, respectively; however, only 40% of our active individuals with DCM demonstrated abnormal ECGs.7 Although, beyond the scope of this paper, genetic testing may have a role in resolving this diagnostic conundrum; however, it is limited by the relatively high cost and low yield for results.
Indices of diastolic and longitudinal function
Baseline echocardiographic markers of systolic and diastolic function as assessed by E′ and S′ at the lateral mitral annulus had a sensitivity of 51.4% and 88.6%, respectively, in differentiating between grey-zone athletes and patients with DCM. Although GLS was higher in the grey-zone athletes compared with patients with DCM, over 50% had low values.5 Interpretation of these results is challenging because currently there is no clear consensus on ‘normal’ GLS values in athletes with a borderline or low LVEF. A meta-analysis by Beaumont et al 18 reported that GLS values in athletes ranged from −16.5% to −23.3% and were lower in endurance athletes. Our results suggest that GLS may be of limited value in this context as low values may not be pathological. Further research is required on the spectrum of GLS values in endurance athletes with borderline or mildly depressed LV function at rest.
Exercise stress echocardiography
Our results demonstrate the importance of exercise echocardiography in differentiating between these entities. Failure to increase LVEF by >11% from baseline to peak exercise is a useful marker of impaired contractile reserve. Only six patients with DCM were able to generate an LVEF >63% at peak exercise compared with more than 90% of the grey-zone athletes and all the athletic controls and therefore the inability to achieve a peak LVEF >63% is an additional marker of pathology. The sensitivity of either of these parameters was around 80% and the specificity was around 90%. Combining these parameters to define a ‘normal’ test reduces the false negatives to 5 (14.2%) with only 2 (8%) false positive results.
There are limited data used to define contractile reserve in health and this has predominantly focused on pharmacological and non-echocardiographic methods.13 19 20 We used exercise echocardiography as it is more physiological and exercise echocardiography is readily available to the physician. Our findings are in-keeping recent study using exercise CMR which also found that a failure to increase LVEF by >11% at peak exercise predicted DCM.21
Cardiopulmonary exercise testing
Although all but one of the grey-zone athletes showed normal pVO2, we observed normal pVO2 in three-quarters of the DCM cohort. Additionally, superior pVO2 >120% predicted was seen in a fifth of our cohort which is similar to a published study looking athletes with hypertrophic cardiomyopathy.22 All the individuals with a pVO2>120% predicted had ventricular arrhythmias and most had late enhancement on CMR. Therefore, highly trained individuals may have excellent functional capacity despite significant pathology
Cardiovascular magnetic resonance
In our study, CMR identified pathological LGE in only 50% patients with DCM, suggesting that baseline CMR at rest is not enough on its own to exclude pathology which gives further importance to the role of stress echocardiography in this setting. Although we did not use T1 and T2 mapping techniques, data suggest these techniques may be useful in distinguishing athlete’s heart from DCM.23
Algorithm
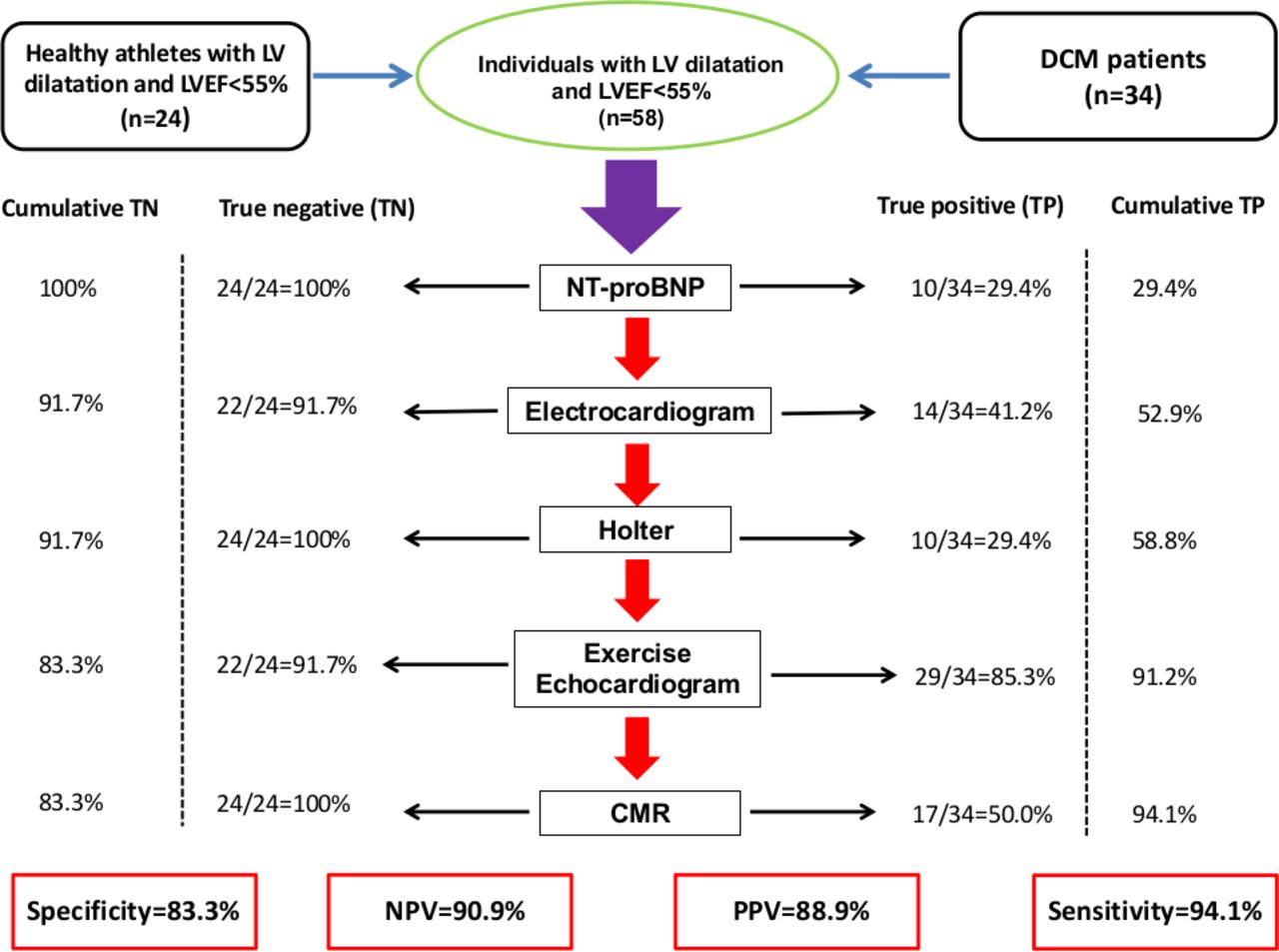
Based on our findings, we have produced a clinical algorithm with diagnostic thresholds to aid physicians when assessing highly active individuals with a dilated LV and an LVEF <55% (figure 3) and demonstrated its utility using our data (figure 4). The two individuals without CMR have been excluded from analysis. The combination of NT-proBNP, ECG and Holter monitoring would confirm DCM in <60% of cases. An additional exercise echocardiogram would result in a diagnosis in 31 (91.2%) cases. A subsequent CMR could exclude pathology in another 3% of cases without impact on false positives. The algorithm has a sensitivity of 94.1%, specificity of 83.3%, positive predictive value of 88.9% and negative predictive value of 90.9%. More than 70% of our patients with DCM had a normal pVO2; therefore, we would not recommend this investigation in isolation.

This figure outlines a simple algorithm to aid physicians when assessing active individuals with LV dilatation and LVEF <55%. On the left are the changes that would support physiological adaptation and on the right those that suggest pathological remodelling. The ECG was interpreted as per the international recommendations in athletes.7 CMR, cardiovascular magnetic resonance; DCM, dilated cardiomyopathy; LV, left ventricular; LVEF, left ventricular ejection fraction; LBBB, left bundle branch block; LGE, late gadolinium enhancement; NSVT, non-sustained ventricular tachycardia; TWI, T-wave inversions; VEs, ventricular extrasystoles.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The figure demonstrates the utility of the stepwise clinical algorithm for differentiating between physiological adaptation and morphologically mild DCM in apparently healthy individuals with LV dilatation and LVEF <55%. The number and percentages of both cohorts with abnormal investigations is shown with the cumulative TN and TP results on the extreme right and left, respectively. The overall sensitivity of the algorithm is 94.1% with a specificity of 83.3%. The PPV is 90.3% with an NPV of 94.7%. CMR, cardiovascular magnetic resonance; DCM, dilated cardiomyopathy; LV, left ventricular; LVEF, left ventricular ejection fraction; NPV, negative predictive value; NT-proBNP, N-terminal pro-brain natriuretic peptide; PPV, positive predictive value; TN, true negative; TP, true positive.
Limitations
Study participants were predominantly Caucasians and exclusively male; therefore, results may not readily be applicable to female athletes or the black athletic population. Given the rarity of patients with DCM who are asymptomatic and athletes in the grey zone, the numbers studied are relatively small. The algorithm was derived and assessed in the same cohort which may result in over-optimistic results; therefore, larger studies are required to validate our findings. Due to the cross-sectional nature of the study, we are unable to confidently exclude the development DCM in the grey-zone athletes in the future.
Conclusion
When attempting to differentiate between physiological LV enlargement with a borderline/low baseline LVEF from mild DCM, a combination of NT-proBNP, ECG, Holter monitoring, baseline echocardiographic and CMR parameters have a modest discriminating value; however, exercise echocardiography has good sensitivity and excellent specificity.
Key messages
What is already known on this subject?
Dilated cardiomyopathy (DCM) is a recognised cause of sudden death in young athletes. It is also known that around 11% of healthy endurance athletes develop physiological left ventricular dilatation with a low/borderline left ventricular (LV) ejection fraction that may simulate DCM. Thus, a distinct grey zone exists between physiological remodelling and DCM where erroneous misinterpretation has potentially serious consequences.
What might this study add?
We have demonstrated that failure to increase LV ejection fraction >11% from baseline to peak exercise and inability to augment the LV ejection fraction >63% at peak exercise during exercise stress echocardiography are suggestive of DCM with high sensitivity of around 80% and specificity >90%. Additionally, we used a composite of routine investigations to derive an algorithm to help clinicians to differentiate between athletes with a physiological increase in LV size and borderline or low baseline LV ejection fraction (grey zone) and DCM. The algorithm has a sensitivity of 94.1%, specificity of 83.3%, positive predictive value of 88.9% and negative predictive value of 90.9% in predicting DCM.
How might this impact on clinical practice?
An erroneous diagnosis of DCM in an athlete with a physiologically increased LV size and borderline or low resting LV ejection fraction may lead to unnecessary disqualification from sport. Conversely, an erroneous diagnosis of athlete’s heart in an individual with morphologically mild DCM deprives the individual of prognostic medications and provides false reassurance which may culminate in progressive deterioration of LV function and an exercise-related sudden death. Our findings and proposed algorithm will aid cardiologists and sports physicians when assessing active individuals with LV dilatation and LV ejection fraction <55% (grey zone). Although our results are promising, the numbers are relatively small and require validation in a larger cohort.
References
Footnotes
Twitter @drlynnemillar, @harshil_dhutia, @MichaelPapadak2, @SSharmacardio
Correction notice Since the online publication of this article, the authors have noticed that the affiliations were incorrect. The affiliation list has now been reduced from 9 to 6 affiliations.
Contributors All authors have been have made substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data and preparation of the manuscript. All authors contributed to manuscript preparation, manuscript revision, quality control and conduct of the study. LMM, ZF, MP, MR, JO’D, DO, MTTE, NB, ERB, GC-W, RS and SS contributed to the study design/planning. LMM, ZF, GF, GS-F, HD, AMa, AMe, AD’S, JW, DO, RS and SS contributed to data acquisition, analysis and interpretation. LMM, GF, RS and SS contributed to statistical analysis. LMM and SS are guarantors for the study.
Funding LMM, HD, AMa and GF were funded by research grants from CRY. AD’S and AMe were funded by research grants from the British Heart Foundation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Full ethical approval was granted by the Chelsea Research Ethics Committee, London, UK, and participants provided informed written consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data, analytical methods and study materials will not be made available to other researchers for the purpose of reproducing the results or replicating the procedure. Researchers interested in the data, methods or analysis can contact the corresponding author for more information.