Article Text

Abstract
Objective We aimed to estimate the current use of secondary prevention drugs and identify its associated individual characteristics among those with established cardiovascular diseases (CVDs) in the communities of China.
Methods We studied 2 613 035 participants aged 35–75 years from 8577 communities in 31 provinces in the China Patient-Centered Evaluative Assessment of Cardiac Events Million Persons Project, a government-funded public health programme conducted from 2014 to 2018. Participants self-reported their history of ischaemic heart disease (IHD) or ischaemic stroke (IS) and medication use in an interview. Multivariable mixed models with a logit link function and community-specific random intercepts were fitted to assess the associations of individual characteristics with the reported use of secondary prevention therapies.
Results Among 2 613 035 participants, 2.9% (74 830) reported a history of IHD and/or IS, among whom the reported use rate either antiplatelet drugs or statins was 34.2% (31.5% antiplatelet drugs, 11.0% statins and 8.3% both). Among the 1 530 408 population subgroups, which were defined by all possible permutations of 16 individual characteristics, reported use of secondary prevention drugs varied substantially (8.4%–60.6%). In the multivariable analysis, younger people, women, current smokers, current drinkers, people without hypertension or diabetes and those with established CVD for more than 2 years were less likely to report taking antiplatelet drugs or statins.
Conclusions The current use of secondary prevention drugs in China is suboptimal and varies substantially across population subgroups. Our study identifies target populations for scalable, tailored interventions to improve secondary prevention of CVD.
- heart disease
- stroke
Statistics from Altmetric.com
Introduction
Cardiovascular diseases (CVDs), especially ischaemic heart disease (IHD) and ischaemic stroke (IS), are the leading causes of death in China.1 Therapies for the secondary prevention of CVD such as aspirin, β blockers, angiotensin converting enzyme inhibitors (ACEIs) and statins could reduce cardiovascular mortality.2 3 Therefore, ensuring widespread use of secondary prevention therapies is crucial for decreasing the burden of CVD in China.
Prior community-based studies in China report that the use of secondary prevention drugs was low (less than 20% taking antiplatelet drugs and less than 2% taking statins) before 2009.4 5 After the health reform of 2009, health insurance coverage expanded, and out-of-pocket payments declined in China.6 In parallel with insurance reform, evidence-based guidelines for secondary prevention of IHD and stroke were published.7–9 Hospital-based studies suggest these developments have been accompanied by improvements in the treatment for secondary CVD prevention.10 However, community physicians lack awareness of the secondary prevention recommendations.11 Individual factors including age, income and severity of diseases also impact on the persistence of secondary prevention medications.12 We have previously shown there is an extremely low use of aspirin and statins for primary prevention in patients with high CVD risk in community settings in China.13 Yet, little is known about the current use of these agents for those with diagnosed CVD. Furthermore, variations in secondary preventive treatment for CVD among population subgroups, which would support targeted preventive health policies in China, have not been characterised.
Accordingly, we report findings from a national community-based project in mainland China. Our aim was to report the use of secondary prevention drugs among those with IHD and/or IS in the community, assess variations among population subgroups and identify the demographic, socioeconomic and health-related factors associated with secondary preventive treatment for CVD in China.
Methods
Study design and participants
The China Patient-Centered Evaluative Assessment of Cardiac Events Million Persons Project is a government-funded public health programme designed to focus on high CVD risk throughout China. Details of the project design have been described previously.14 Briefly, from September 2014 to November 2018, 189 county-level regions (114 rural counties, 75 urban districts) in all 31 provinces in mainland of China were selected to provide diversity in geographic distribution, population structure (ethnicity distribution) and exposure to risk factors and disease patterns (figure 1). Study site selection considered population size, population stability and local capacity to support the project (details were shown in online supplementary eAppendix 1). Local residents aged 35–75 years, who were currently registered in the community’s Hukou (a record officially identifying area residents) or had lived in the community for at least 6 months of the prior 12 months, were invited and recruited in this project. All enrolled participants provided written informed consent.
Supplemental material

Study sites in China Patient-Centered Evaluative Assessment of Cardiac Events Million Persons Project.
Patient and public involvement
This study was done without patient involvement. Patients were not invited to participate in study design, data interpretation and writing or editing of the manuscript.
Data collection and variables
For each participant, blood pressure, blood lipids, blood glucose, height and weight were measured. Blood pressure was measured twice in the right upper arm after 5 min of rest in a seated position using a standardised electronic blood pressure monitor (Omron HEM-7430, Omron Corporation, Kyoto, Japan). If the difference between the two systolic blood pressure measurements was larger than 10 mm Hg, a third measurement was obtained, and the average of the last two readings was used. Hypertension was defined as systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg or the use of antihypertensive medications according to the US and Chinese definitions.15–17 Participants were required to wear light clothes, no shoes and no cap for measurements of height and weight. Body mass index (BMI) was defined as weight in kilograms divided by the square of height in metres. Normal weight was defined as 18.5≤BMI≤23.9, low weight was defined as BMI <18.5, overweight was defined as 24.0≤BMI≤27.9 and obesity was defined as BMI ≥28.0 kg/m2, based on recommendations of the Working Group on Obesity in China.18
Standardised in-person interviews were conducted by trained personnel to collect information on sociodemographic status, lifestyle, medical history and medication usage. All participants were asked if they had the medical histories or received the treatments, including myocardial infarction, coronary artery bypass graft surgery (CABG) or percutaneous coronary -intervention (PCI) and stroke. If participants had a previous history of stroke, they were asked about the type of stroke (IS, haemorrhagic stroke or unclear). Previous history of IHD was derived based on self-reported of myocardial infarction, CABG or PCI. If participants had history of IHD or stroke, they were asked the year of diagnosis. History of hypertension or diabetes was defined as self-reported previously diagnosed hypertension or diabetes. Medication use was determined by self-report of taking drugs for antiplatelet therapy or lipid-lowering in the past 2 weeks. If participants were taking these two kinds of drugs, they were asked to report the name, dose and frequency of each drug (online supplementary eAppendix 2).
Statistical analyses
Among participants with IHD and/or IS, we described the rates of antiplatelet drugs or statins overall and by population subgroups, such as age, sex and urbanity and so on. The use of antihypertensive drugs was also reported. The 95% CIs for prevalence rates were calculated using the Clopper-Pearson method.19
Then, we conducted a subgroup analysis to describe the use of antiplatelet drugs or statins among patients with established CVD. Population subgroups were defined a priori by all possible permutations of 16 characteristics including age group (35–44, 45–54, 55–64 and 65–75), sex (men and women), urbanity (urban and rural), geographic region (Western, Central and Eastern), ethnicity (Han and non-Han), occupation (farmer and non-farmer), annual household income (<10 000 yuan, 10 000–50 000 yuan and >50 000 yuan), education (primary school and below, middle school, high school, college and above), marital status (married and not married), medical insurance (insured and uninsured), current smoker (yes or no), current drinker (yes or no), history of hypertension (yes or no), history of diabetes (yes or no), BMI groups (low weight, normal weight, overweight and obesity) and years since diagnosis (<2, 2–7 and >7 years). We retained 1 530 408 subgroups that included at least 500 participants and assessed the distributions of rates of secondary prevention treatment in these subgroups (online supplementary eAppendix 3). These subgroups were not mutually exclusive. The histogram plots and density plots were used to visualise the estimates in the population subgroups.
Finally, we developed multivariable mixed models with community as a random effect and individual-level variables as fixed effects. Using a logit-link function, we calculated the associations between individual-level variables with the dependent variable accounting for clustering of individuals within communities. The individual characteristics included in the model were age, sex, urbanity, geographic region, ethnicity, education level, occupation, annual household income, marital status, medical insurance, smoking, drinking, history of hypertension, history of diabetes, BMI groups and years since diagnosis. The dependent variable was whether patients with IHD and/or IS reported taking either antiplatelet drugs or statins. Additionally, we fitted mixed models to identified individual characteristics associated with the use of multiple secondary prevention drugs among those with IHD or IS.
We excluded participants with missing value for age, household income, education or BMI. P<0.05 was considered statistically significant. All analyses were conducted with SAS V.9.4 and R 3.4.1 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of study population
Among 2 613 035 participants, 74 830 (2.9%) participants reported a history of IHD and/or IS (online supplementary eFigure 1). Among them, 39.1% (29 231) had IHD, 57.9% (43 359) had IS and 3.0% (2240) had both IHD and IS. The median years since diagnosis was 4 (IQR: 2–7). Among the participants with established CVD, 37 528 (50.2%) were men, the mean age was 61.6±8.1 years, 22.0% were current smoker, 52.9% had previously diagnosed hypertension and 17.6% had previously diagnosed diabetes (table 1).
Baseline characteristics of participants with IHD and/or IS
Use of secondary prevention drugs among participants with established CVD
Overall, the rate of reported antiplatelet drug or statin use was 34.2% among the 74 830 studied population (table 2). The use of secondary prevention drugs among those with IHD were more common than that among those with IS (40.4% vs 29.0% for any of two drugs, 37.4% vs 26.6% for antiplatelet drugs, 14.6% vs 8.2% for statins and 11.6% vs 5.8% for both). Among those with IHD, 10.2% and 10.9% were taking ACEI/angiotensin receptor blocker (ARB) and β blocker for cardiovascular event prevention. About 10% were taking ACEI/ARB for cardiovascular event prevention among those with IS (online supplementary eTable 1).
Use of secondary prevention drugs among participants with IHD and/or IS
Among 11 682 patients with established CVD and taking lipid-lowering drugs, 33% did not remember the exact drug name, which would result in the underestimation of statin use in this study. We conducted a sensitivity analysis to estimate the statin use rate by assuming that patients did not remember the exact drug name were taking statins. The estimated statin use rate is 16.2% among patients with established CVD. Among those with IHD and IS, 21.0% and 12.2% was taking statins, respectively.
The usage rates of secondary prevention drugs increased with age (from 19.2% for 35–39 years to 37.3% for 70–75 years, p<0.001) (table 3 and figure 2). Men was more commonly taking secondary prevention drugs than women (37.9% vs 30.4%, p<0.001). The rates of antiplatelet drug or statin use was higher in urban than in rural areas (35.9% vs 32.9%, p<0.001). Use of antiplatelet drugs or statins was slightly more common among those with higher level of education and household income (p<0.001). Those with medical insurance had higher rates than those without medical insurance, but the difference was not statistically significant (34.3% vs 29.1%, p=0.07). People with hypertension (39.1% vs 28.7%, p<0.001) or diabetes (41.1% vs 32.7%, p<0.001) had significantly higher usage rates. Patients with established CVD diagnosed within 2 years (34.9%) had slightly higher usage rates than those diagnosed 2 or more years before (33.7% for 2–7 years; 33.8% for >7 years, p=0.07). There are few differences in the usage rates of secondary prevention drugs across individual characteristics between those with IHD and IS.

The usage rates of antiplatelet drugs or statins by individual characteristics.
Use of antiplatelet drugs or statins among participants with IHD and/or IS by individual characteristics
Across the 1 530 408 population subgroups, the rates of secondary prevention drugs use varied substantially from 8.4% to 60.6%. Ninety-eight per centof all subgroups had less than 50% usage rates. Groups including people who were elderly, men, having higher education level, having higher household income, with previous diagnosed hypertension or with previous diagnosed diabetes had higher rates of reported use of antiplatelet drugs or statins (figure 3).

Density plots of reported use of antiplatelet drugs or statins in 1 530 408 subgroups defined by 16 patient characteristics subgroups were defined by 16 characteristics including age, sex, urbanity, geographic region, ethnicity, occupation, annual household income, education, marital status, medical insurance, current smoker, current drinker, history of hypertension, history of diabetes, body mass index and years since diagnosis. In the above density plots, we have shown the reported use of antiplatelet drugs or statins of all population subgroups grouped by the variables in the legend. For example, we separated all subgroups by sex, and ‘women’ means all subgroups including women, ‘men’ means all subgroups including men. The vertical axis indicates the probability density of the corresponding reported medication usage rate. The horizontal axis means the reported usage rate of antiplatelet drugs or statins.
Individual factors associated with the secondary prevention drugs use
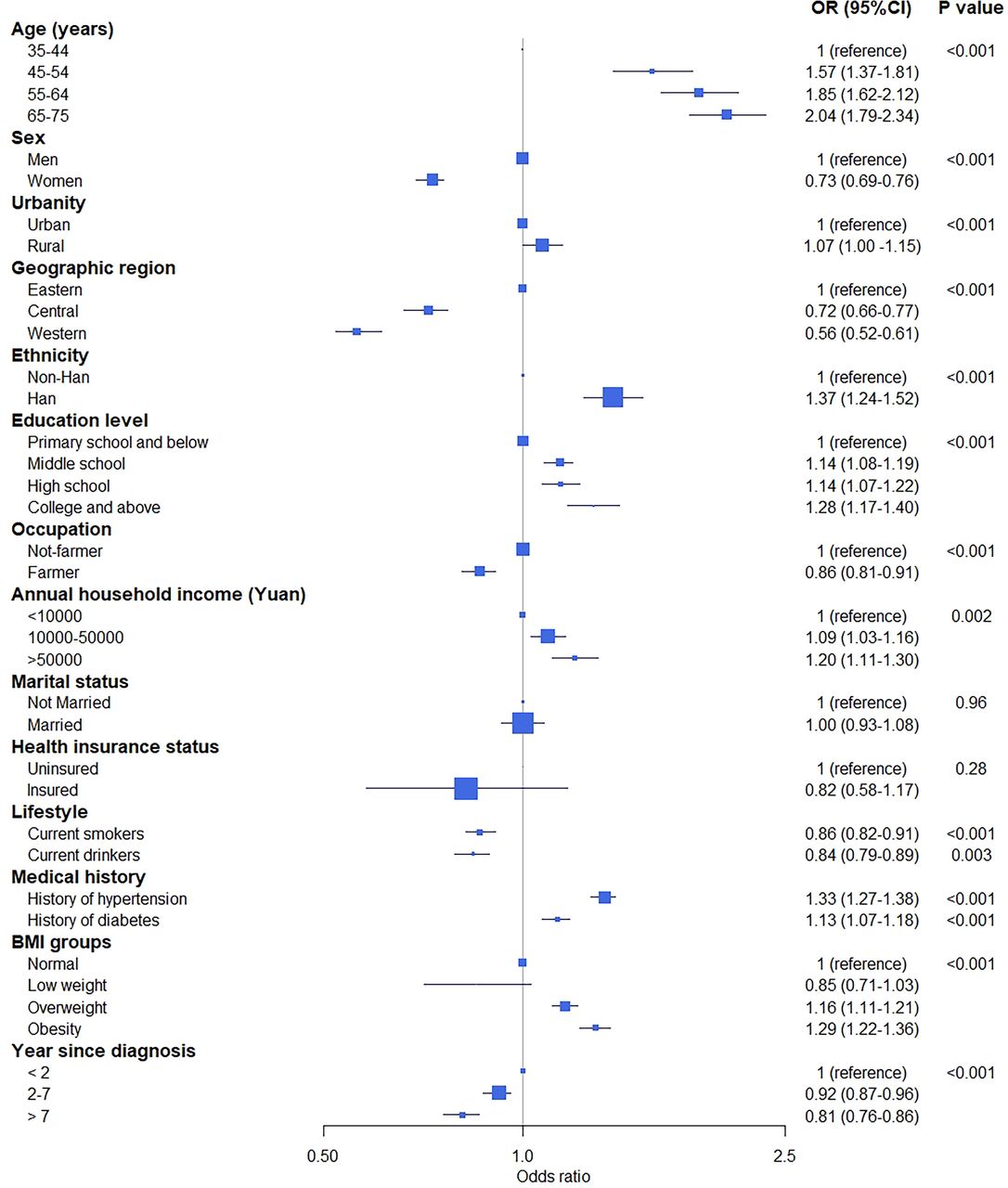
In the mixed model, we found that younger people, women, those with lower education level or those having less household income was less likely to report taking antiplatelet drugs or statins (figure 4). The reported use of antiplatelet drugs or statins was moderately less common in current smokers (OR=0.86, 95% CI 0.82 to 0.91) and current drinkers (OR=0.84, 95% CI 0.79 to 0.89). Patients with self-reported hypertension (OR=1.33, 95% CI 1.27 to 1.38) or diabetes (OR=1.13, 95% CI 1.07 to 1.18) had significantly higher usage rates of antiplatelet drugs or statins. In addition, patients were more likely to take antiplatelet drugs or statins within the first 2 years since diagnosis (2–7 years vs <2 years: OR=0.92, 95% CI 0.87 to 0.96; >7 years vs <2 years: OR=0.81, 95% CI 0.76 to 0.86).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Multivariable regression model for association between individual characteristics and the reported use of secondary prevention drugs or >1 means ‘secondary prevention drug more likely to be used’, whereas or <1 means ‘secondary prevention drug less likely to be used’. The marker size reflects sample size in each subgroup.
Among the patient with IHD who taking secondary prevention drugs, women, those living in rural areas, those with lower education level, those having less household income, current smokers or current drinkers were less likely to report taking at least three kind of drugs (online supplementary eTable 2). Similar findings were identified among the patient with IS who taking secondary prevention drugs (online supplementary eTable 3).
Discussion
About one in three middle-aged adults with IHD and/or IS in this national study reported taking antiplatelet drugs or statins for cardiovascular event prevention, and only 1 in 12 reported taking both antiplatelet drugs and statins. The usage rates of antiplatelet drugs or statins varied substantially across 1.5 million population subgroups defined by 16 individual characteristics. We identified target population subgroups for interventions to improve secondary prevention of CVD, such as younger people, women and people who had lower level of education or household income. Nevertheless, these findings reveal the need to promote secondary prevention therapies in all groups to reduce CVD mortality in primary care settings in China, as the opportunity for improvement is pervasive.
Currently reported usage of secondary prevention drugs is still far from optimal in the communities of China, even though rates in this study represent an improvement from observations before health reform instituted in 2009. A large-scale community-based study, which recruited over 0.5 million residents aged 30–79 years during 2004–2008 from 10 regions in China, reported that only 10.6% and 1.4% of participants with IHD and/or stroke reported taking antiplatelet drugs and statins, respectively.4 Compared with their findings, the current usage rate of anti-platelet drugs are nearly three times higher (31.5% vs 10.6%), and the usage rate of statins is eight times higher (11.0% vs 1.4%) in our study. However, there is still much room for improvement. Furthermore, the usage rates of antiplatelet drugs or statins are much lower than that in other countries. Among US adults aged ≥40 years with previous IHD and/or stroke, the antiplatelet drug use for secondary prevention was 76%.20 Findings from a multicountry study observed that use of antiplatelet drugs and statins for secondary prevention in China was much lower than in North America and Europe (52.2% and 52.1%), South America (29.0% and 15.0%) and Middle East (49.7% and 35.7%).5 This study indicated that therapeutic interventions for patients with established CVD should be widely spread in China. In the meantime, the extremely low use of aspirin (2.4%) and statins (0.6%) in people with high CVD risk founded in our previous study calls for improvement in primary prevention of CVD to effectively reduce the CVD burden.13
Several factors could influence the use of secondary prevention drugs in China. From the healthcare system perspective, recent hospital-based data have indicated that the use of secondary prevention treatment during hospitalisation after acute myocardial infarction dramatically increase during the past decade in China (aspirin: from 78.4% in 2001 to 90.0% in 2011; statins: from 27.9% in 2001 to 88.8% in 2011).10 21 However, huge gaps in the capacity for secondary prevention management among primary care physicians persist. A Chinese study found that less than 50% of community physicians were aware of the secondary prevention recommendations included in the current clinical guidelines.11 Practical guidelines for primary care physicians, physician training and pragmatic implementation strategies are likely to enhance guideline adherence for secondary prevention management. Bidirectional referral mechanisms instituted in China in 2015 could facilitate the provision of preventive therapy by primary care institutions22; this programme however is in the early stages of implementation.
From the patient’s perspective, adherence to secondary preventive treatment is still of great concern and strongly influenced by patients’ awareness and self-management capability. Prior evidence suggested that half of patients hospitalised with an acute cardiovascular event reported discontinuing one or more secondary prevention drugs within few months after discharge.12 23 In a meta-analysis of 376 162 patients, adherence to cardiovascular medications was estimated to be about 57% after a median of 2 years.24 Similar with previous studies,10 21 we have identified that people with lower degrees of health awareness, such as younger people, or people with lower education level, are less likely to take secondary prevention drugs. Moreover, cost-effective approaches to enhancing patients’ self-management in secondary prevention of CVD is lacking, although the number of relevant studies has markedly increased.25 26 Furthermore, financial barriers may have a negative effect on patients’ adherence. Although medical insurance status had no relationship with secondary prevention drug use in our study, we found that lower household income was related. A previous study has also found that about 20% patients in the highest wealth groups, one-third in the middle wealth groups and nearly half in the lowest wealth groups could not afford aspirin, ACEIs, β blockers and statins recommended for the secondary prevention of CVD in lower middle-income countries (including China and other three countries).27 In addition, higher rates of adverse outcomes to statin or aspirin therapy has been reported in Asian population,28 29 which might also influence patient’s adherence.
This study has several limitations. First, a random probability sample was not taken to ensure representativeness in this study; however, our sampling from all 31 provinces in mainland China makes it likely that the findings are generalisable to the mainland China. Second, the use of secondary prevention drugs was self-reported, which could be subject to recall bias and lead to an underestimation of the medication use. Among patients with established CVD and taking lipid-lowering drugs, 33% did not remember the exact drug name. Even if we assume that all these patients were taking statins, the statin use rate is still very low (16%), and the diagnosis of CVD was based on self-reported data. Previous studies have found that self-reported CVD are highly sensitive and specific.30 Although there might be some misclassification, but regardless the rates are quite low and the main findings would be unexpected to change. Third, we did not collect information about the contraindications of antiplatelet therapy and statins. This may underestimate the use of secondary prevention medications. However, the proportion of CVD patients having contraindications is small.10 21 Finally, we did not collect information, such as people’s attitudes and knowledge about secondary prevention treatment for CVD. Therefore, we were unable to assess potential reasons for the low use rates.
In conclusion, among participants with IHD and/or IS, about one in three reported taking antiplatelet drugs or statins and 1 in 12 reported taking both kinds of drugs in this study. The uses of antiplatelet drugs and stains are low in all subgroups, and particularly in younger people, women and people who had lower level of education or household income. The scalable, tailored and effective interventions are needed to improve the secondary prevention for cardiovascular diseases in China.
Key messages
What is already known on this subject?
Hospital-based studies suggest that the use of therapies for secondary cardiovascular disease (CVD) prevention has been improved with the development in medical insurance reform and implementation of evidence-based guidelines in China.
What might this study add?
This study assesses the use of secondary prevention drugs of CVDs that varies across population subgroups in the communities of China. We find that only 34.2% of middle-aged adults with ischaemic heart diseases and/or ischaemic stroke reported taking antiplatelet drugs or statins for secondary prevention. The reported use rates of secondary prevention medications varied substantially among the 1 530 408 population subgroups (from 8.4% to 60.6%).
How might this impact on clinical practice?
By exploring the gaps in secondary prevention of CVD in the communities of China, we highlight the needs of effective interventions that can be tailored to populations at highest risk for undertreatment and are scalable to large populations to improve the secondary prevention for CVDs in China.
Acknowledgments
We would like to thank all the subjects for their participation. We appreciate the contributions made by project teams at the National Center for Cardiovascular Diseases and the Yale-New Haven Hospital Center for Outcomes Research and Evaluation in the realms of project design and operations, particularly data collection by Yang Yang, Jingwei Yang, Jianlan Cui, Wei Xu, Bo Gu, Liping Zhang, Shuang Hu, Chaoqun Wu, Hui Zhong and Binbin Jin. We appreciate the Ministry of Finance of China and National Health Commission of China for funding support. We would like to thank all provincial and regional officers and research staff in all 31 provinces for their collection of data and biosamples.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JL and LZ are joint first authors.
Correction notice Since this article was first published online, middle initials have been added to Professors Krumholz and Masoudi.
Contributors HK and JiapL designed the study. XZ, JingL, HK, JiapL and LZ conceived of this article. JiapL and LZ wrote the manuscript with further contributions from XZ, JingL, YL, MS, XL, JiamL, HZ, KN, FM and HK. JiapL completed all the statistical analysis. All authors interpreted data, contributed to critical revisions and approved the final version of the article.
Funding This project was supported by the National Key Research and Development Program (2017YFC1310801 and 2017YFC1310803) from the Ministry of Science and Technology of China; the CAMS Innovation Fund for Medical Science (2017-I2M-2-002, 2017-I2M-B&R-02, 2016-12M-1-006 and 2016-12M-2-004); the Ministry of Finance of China and National Health Commission of China.
Disclaimer The funder of the study had no role in study design, data collection, data analysis, data interpretation, or the decision to submit the manuscript for publication.
Competing interests HK discloses that he is a recipient of research agreements from Medtronic and from Johnson & Johnson (Janssen), through Yale, to develop methods of clinical trial data sharing; is the recipient of a grant from the Food and Drug Administration and Medtronic, through Yale, to develop methods for postmarket surveillance of medical devices; works under contract with the Centers for Medicare & Medicaid Services to develop and maintain performance measures; chairs a cardiac scientific advisory board for UnitedHealth; is a participant/participant representative of the IBM Watson Health Life Sciences Board; is a member of the Advisory Board for Element Science and the Physician Advisory Board for Aetna; and is the founder of Hugo, a personal health information platform. FAM has a contract with the American College of Cardiology for his role as the Chief Scientific Advisor of the NCDR. All other authors declare no competing interests.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.