Article Text

Statistics from Altmetric.com
The use of implantable cardiac defibrillators (ICDs) has dramatically improved outcomes for patients with many types of heart disease. Yet, the patient with an ICD faces a difficult decision near the end of life—should the ICD be deactivated and, if so, when? Evidence to support a specific approach to this clinical dilemma is not amenable to standard research approaches because the outcomes are qualitative, not quantitative. Thus, carefully designed and implemented qualitative research studies are needed to inform clinical practice. In this issue of Heart, Stoevelaar and colleagues1 performed a focus group study using a constant comparative method for analysis of transcriptions from group sessions with 41 participants. Patients reported that few physicians discussed deactivation of ICDs. Patients also expressed a desire for more information about deactivation and advance care planning, depending on disease stage and patient preferences. The online version of this article also features a helpful video abstract.
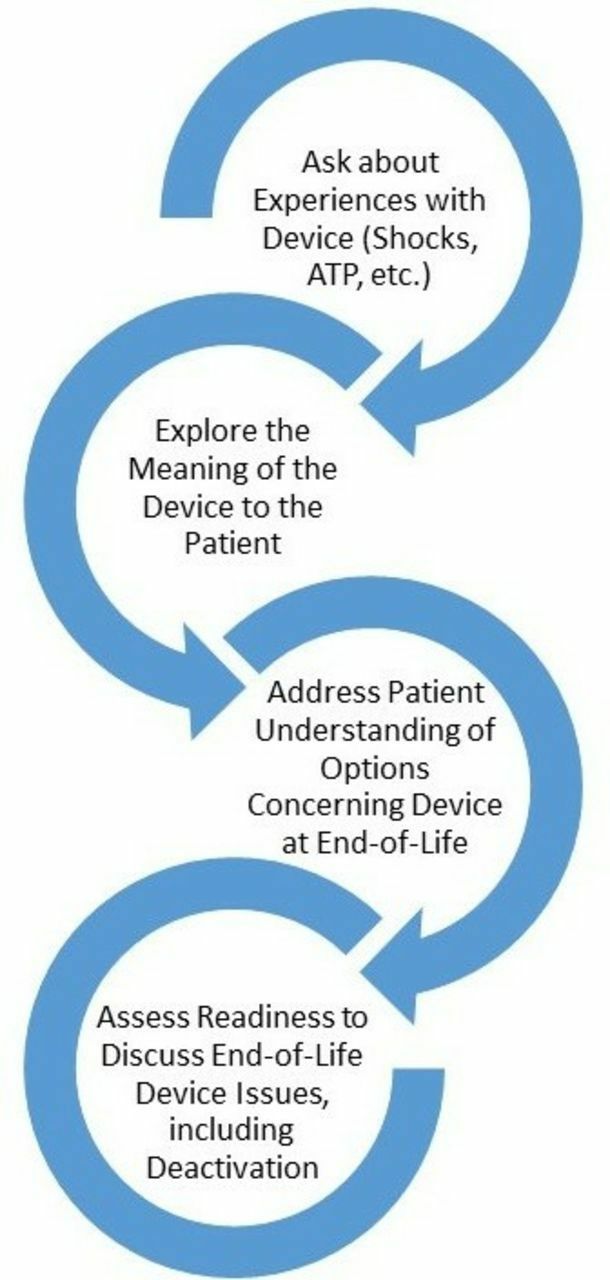
In the accompanying editorial, Steiner2, Bernacki and Kirkpatrick suggest a tiered approach to discussing the patient’s experience with their ICD, their understanding of the options for advance care planning and the possibility of ICD deactivation (figure 1). They conclude: ‘The heterogeneity of patients’ views on ICD therapy at the end of life presented in this manuscript supports the need for more open communication and ongoing education on this topic for both patients and providers. Patients look to their clinicians for guidance with end-of-life decision-making, and it is the clinician’s responsibility to explore the patient’s perspectives on therapies in order to inform this guidance.’

Series of issues to discuss with patients prior to entering into an advance care planning or goals of care discussion concerning management of implantable cardioverter-defibrillators at the end of life. ATP, antitachycardia pacing.
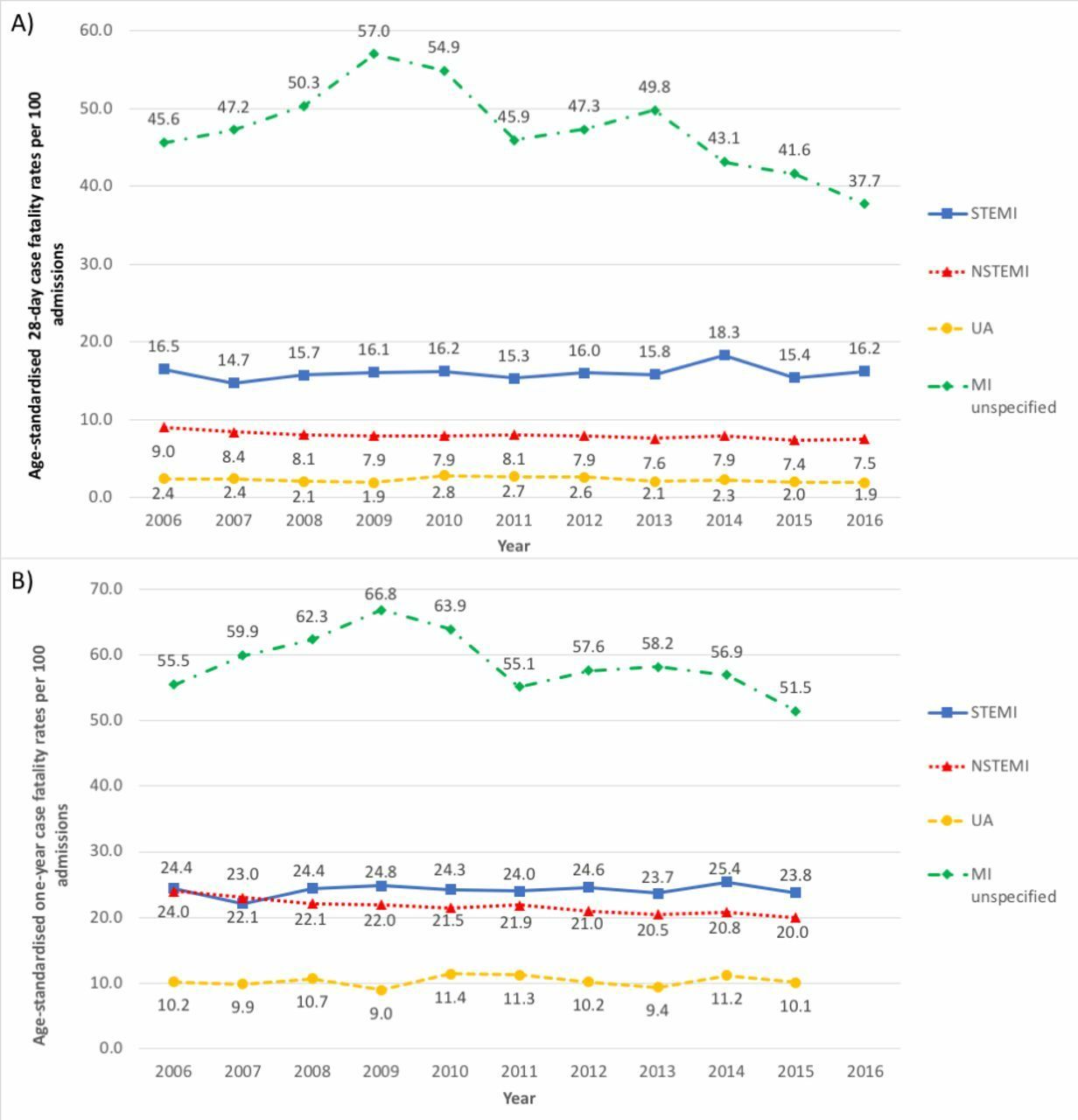
The incidence and mortality of coronary artery disease continues to decline worldwide but there have been inconsistent findings for the relative contribution of different acute coronary syndrome (ACS) subtypes. Wang and colleagues3 report on ACS hospitalisation in the All New Zealand Acute Coronary Syndrome Quality Improvement (ANZACS-QI) 31 study which included 188 264 ACS admissions over the decade from 2006 to 2016. Event rates for all types of ACS declined over this time period while the proportion of patients treated with revascularisation increased. Overall, 1-year mortality in patients with non-ST elevation myocardial infarction showed a relative decline of 1.6% per year but there was no change in mortality for ST-elevation myocardial infarction or unstable angina (figure 2).

Age-standardised mortality outcomes after ACS admissions by subtype 2006–2016 at (A) 28 days and (B) 1 year. ACS, acute coronary syndrome; MI, myocardial infarction; NSTEMI, non-ST-elevation myocardial infarction; STEMI, ST-elevation myocardial infarction; UA, unstable angina.
The apparent paradox that higher rates of re-vascularisation were not associated with a change in mortality for ST-elevation myocardial infarction or unstable angina highlights the fact that medical therapy, not revascularisation, has had the most impact on declining coronary artery disease mortality rates over the last 40 years, as illustrated in an elegant figure by Shaw4 (figure 3). He also points out that the higher mortality rates reported using registry data, such as the study by Wang and colleagues,3 compared with randomised clinical trials, reflect the selection criteria of clinical trials versus the inclusion of all-comers in registries, including those with cardiogenic shock, comorbidities and advanced age. He also suggests: ‘The less than optimal use of guideline-directed therapy, namely invasive angiography, needs to be addressed, and there may have been lower than expected use of secondary prevention therapies, including antiplatelet and lipid-lowering therapy, which if addressed could result in improved patient outcomes.’

The figure demonstrates the reduction in age-standardised mortality rates for coronary artery disease in the UK between 1979 and 2013.8 The corresponding major advancements in cardiovascular preventative and therapeutic strategies and the year at which they were instituted into practice are shown on the x-axis. AICD, automatic implantable cardioverter defibrillator; PCI, percutaneous coronary intervention; PCSK-9 Proprotein Convertase Subtilisin Kexin Type 9; STEMI, ST segment elevation myocardial infarction.
The cardiovascular risk associated with being born during a famine period are not trivial. In a study by Meng and colleagues5 of over 92 000 participants currently aged 39–51 years, urban (but not rural) participants born during a famine period had a higher risk of cerebrovascular disease (HR 1.18; 95% CI 1.09 to 1.28). In participants with lower levels of physical activity, prenatal famine exposure was associated with a higher risk of ischaemic heart disease (HR 1.15; 95% CI 1.05 to 1.26) and cerebrovascular disease (HR 1.13; 95% CI 1.05 to 1.21). The clinical implication of this study, as discussed by Li and Liu6 is that the risk associated with prenatal famine exposure might be attenuated by adult lifestyle behaviours, such as increased physical activity. They also point out that: ‘we should keep in mind that cardiovascular disease (CVD) risk factors exist in all stages of the life span including fetal life, infancy and childhood, adolescence, and adult life. Substantial evidence indicates that CVD processes begin early in life and are influenced by lifestyle and environmental exposures over the life course.
An excellent review article in this issue7 focuses on imaging in patients with a suspected acute aortic syndrome. The primary modality at most medical centres is computed tomographic imaging but additional advanced imaging approaches may be helpful in selected patients. Imaging is essential not only for diagnosis, but also for procedural planning and optimisation of outcomes after intervention (figure 4).

Diagnostic imaging algorithm, for suspected acute aortic syndrome. In patients with suspicion of acute aortic syndrome, CTA is the imaging modality of choice. *In those patients who are at high risk for contrast-induced nephropathy or too unstable for a CTA, echocardiographic evaluation is appropriate. †When TTE is rapidly available at the bedside, it can be used to evaluate for the presence of a dissection while awaiting mobilisation of TOE. Though a positive TTE can prompt appropriate treatment, it is insufficient to exclude the diagnosis. Thus, a TOE should be performed if the TTE is negative or inconclusive. ‡In those patients with very high suspicion and a negative TOE, MRA can be performed in those who are stable; if the patient is too unstable for MRA, then CTA should be performed to confirm a negative TOE in discussion with the patient even when a possible contraindication CTA is present. CTA, CT angiography; ICU, intensive care unit; MRA, magnetic resonance angiography; OR, operating room; TOE, transoesophageal echocardiogram; TTE, transthoracic echocardiogram.
A review article by Arnold and McCann8 provides an overview of the utility of cardiac magnetic resonance (CMR) imaging for the practicing cardiologist. CMR imaging increasingly is a key element for diagnosis in patients with cardiomyopathies, uncertain myocardial viability, right ventricular dysfunction and valvular heart disease (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Clinical applications of CMR modalities summary of the role of CMR modalities in diagnosis and directing therapy. ACS, acute coronary syndrome; ARVC, arrhythmogenic right ventricular cardiomyopathy; CAD, coronary artery disease; CMR, cardiovascular magnetic resonance; HCM, hypertrophic cardiomyopathy; LGE, late gadolinium enhancement.
Footnotes
Contributors All authors contributed.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.