Article Text

Statistics from Altmetric.com
Many studies suggest there is a higher risk of cardiovascular disease (CVD) in individuals who are lonely, not married or living alone.1–4 But which is it: a feeling of loneliness, living by yourself or being married that counts? And is this association mediated by psychological factors; lifestyle behaviours such as diet, exercise and not smoking; or variation in healthcare use including CVD risk reduction treatments? Additionally, are biological factors important? For example, it has been hypothesised that telomere length, which is a marker of biological ageing and psychological distress, might explain the association between living alone and CVD risk.
In this issue of Heart, Chen and colleagues5 examined the relationship between marital status, leucocyte telomere length (LTL) and incidence CVD using data from over 10 000 participants in the Swedish Twin Registry. Compared with people who were married or cohabiting, people living singly (living alone, widowed, divorced or separated) had shorter LTL and an about 20% higher risk of CVD (HR 1.21, 95% CI: 1.08, 1.35). However, the association between marital status and CVD risk appeared to be independent of telomere length. Moreover, the risk of living singly was attenuated by adjustment for age, sex, educational attainment, body mass index, smoking, physical activity, diabetes, hypertension and dyslipidaemia (HR 1.12, 95% CI: 1.00 to 1.26).
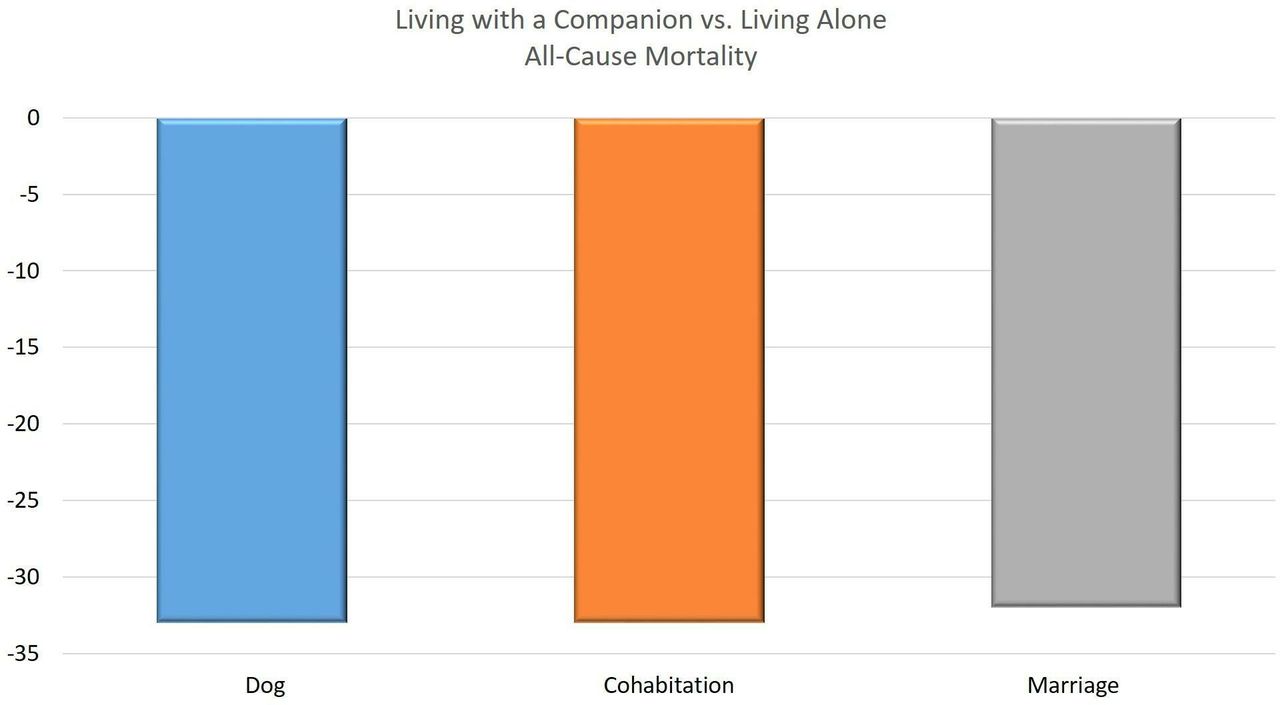
In an editorial, O’Keefe et al 6 summarise previous studies on marital status and CVD risk, including a meta-analysis of 34 prospective cohort studies with a total of over two million participants which showed a 40% increased risk of CVD in unmarried, compared with married, men and women.1 In addition to lower psychosocial stress and higher resilience, they suggest that ‘an individual who is cohabitating is more likely to a) seek healthcare earlier and more often; b) be more adherent to prescribed treatment; and c) be encouraged by their partner to adopt healthier behaviours.’ Interestingly, looking at results of different studies the benefit of marital status appear to be similar to the benefit of cohabitation or dog ownership7 for people living singly (figure 1). They conclude: ‘the advantages of cohabitation for one’s cardiovascular health and longevity might help inform a decision about the pros and cons of living with another person or a canine companion. Two may or may not live as cheaply as one, but two together will probably live longer than one alone.’ Still, it likely is the healthy lifestyle behaviours that go with living together that make the difference, not marital status.

Risk reduction of all-cause mortality by type of companionship. Dog ownership: people living singly with a dog versus singly with no dog; cohabitation: living with a partner versus singly; marriage: married and living together versus living singly regardless of marital status (never married, divorced or widowed).
Another clinically relevant article in this issue of Heart addresses the discordance in physician perceptions of CVD risk versus actual risk for patients who are overweight or obese.8 Litwin and colleagues used data from the Prospective Multicenter Imaging Study for Evaluation of Chest Pain trial including over 10 000 patients, approximately half of whom were obese, who had stable symptomatic coronary artery disease (CAD). In addition to stress and coronary imaging data, CVD outcome data were used to compare physicians’ clinical impression of risk versus actual CVD risk stratified by body mass index (BMI). Although physicians’ clinical impression of risk increased progressively for patients with a higher BMI, actual CVD risk was highest for overweight (not obese) patients (figure 2). For each 10% increase in the Diamond-Forrester probability of CAD, the adjusted OR for obstructive CAD was 1.5 (95% CI 1.4 to 1.5) in patients with a BMI <35 kg/m2, but only 1.2 (95% CI 1.1 to 1.3) in those with BMI ≥35 kg/m2 (interaction p<0.001). The authors conclude ‘Obesity is very common in contemporary populations undergoing CAD evaluation and higher degrees of obesity are associated with substantial differences in risk factor burden, symptoms and pretest risk assessment. Discordances exist between physician assessment of risk, pooled risk scores and actual event rates that are more pronounced as BMI rises.’ These data suggest that clinical risk prediction rules need to be recalibrated to reflect our current, increasingly overweight and obese, populations.

Pooled risk models versus physician assessment of probability of obstructive coronary artery disease (CAD). Percentage of patients in each body mass index category who were classified as being at high risk of having obstructive CAD by the treating physician or by the updated Diamond-Forrester prediction model.
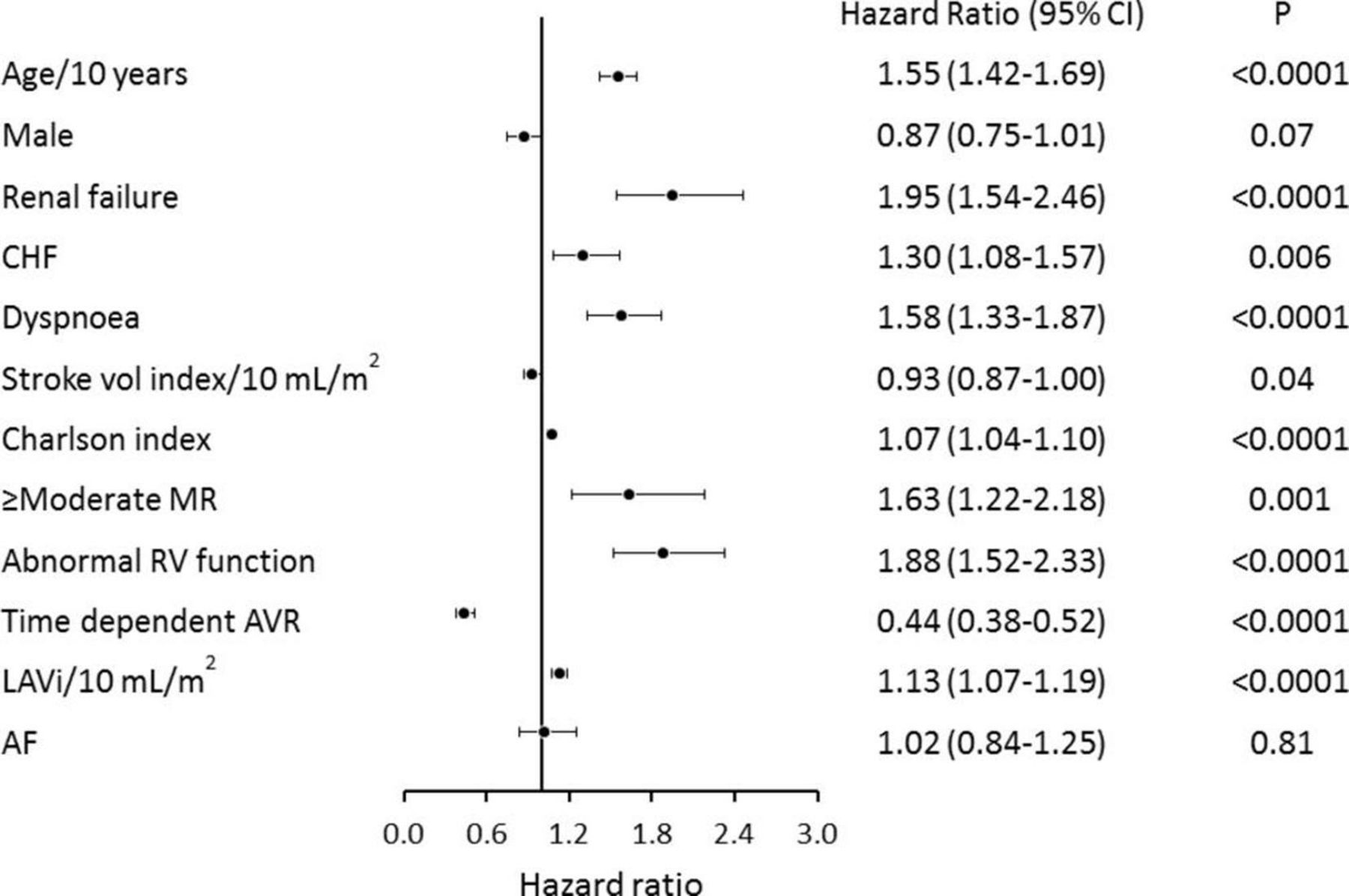
Atrial fibrillation (AF) is present in up to 35% of adults with aortic stenosis (AS) yet it has been unclear if this simply is due to the overlapping incidence of two common diseases in the elderly or whether AF is a marker of AS disease severity. In a cohort of 1847 patients with severe AS, of whom 16% were in AF, Zhang and colleagues9 found a lower survival rate at 5 years in those with AF compared with those in sinus rhythm (age-adjusted and sex-adjusted HR=1.66 (1.40 to 1.98), p<0.0001). However, on multivariate analysis with correction for age, symptoms, mitral regurgitation, right ventricular function, left atrial size and aortic valve replacement, AF was not an independent predictor of mortality (HR=1.02 (0.84 to 1.25), p=0.81).(figure 3). The authors conclude that ‘Symptoms in patients with severe AS and AF may be better attributed to AS. Presence of AF should prompt evaluation for associated structural heart diseases which, when present, further increase risk of mortality without aortic valve replacement.’
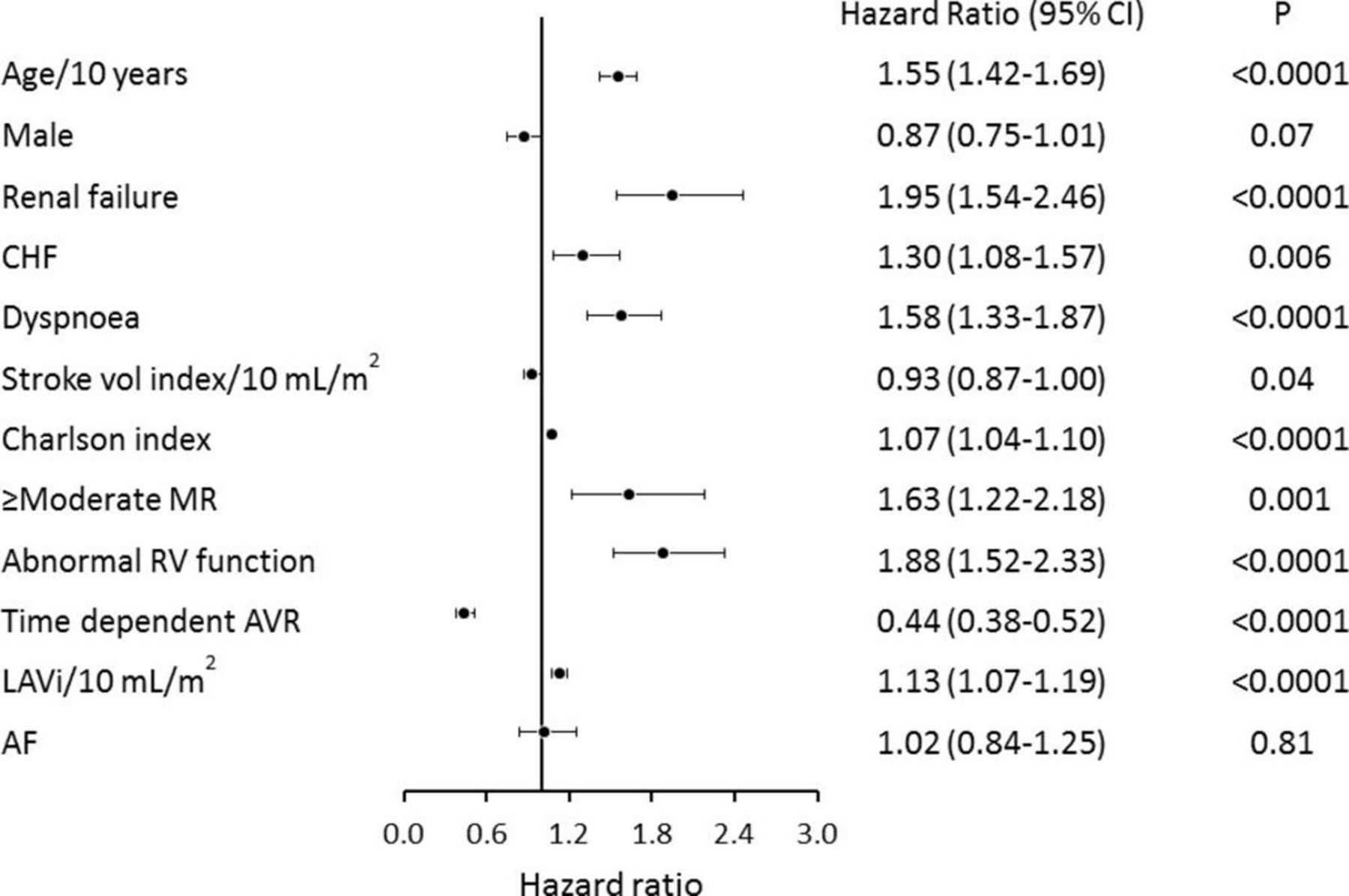
Forest plot of multivariable predictors of overall survival. HRs, 95% confidence limits and p values from the multivariable analysis are illustrated. AF, atrial fibrillation; AVR, aortic valve replacement; CHF, congestive heart failure; LAVi, left atrial volume index; MR, mitral regurgitation; RV, right ventricular.
A point-counterpoint set of editorials in this issue of Heart debates the role of high-sensitivity cardiac troponin (hs-cTn) measurements in clinical practice.10 11 Collinson et al 10 discuss their concerns with the troponin measurements in the CHARIOT (Current Threshold for Diagnosis of ‘Abnormality’, Including Non-ST Elevation Myocardial Infarction, Using Raised Highly Sensitive Troponin Appropriate for a Hospital Population) study.12 They emphasise that: ‘It is important to remember that hs-cTn assays are extremely sensitive for myocardial injury, and that myocardial injury does not always (in fact most often), does not equate acute myocardial infarction (MI). The diagnosis of MI remains clinical but the diagnostic process should be circular rather than linear, as illustrated in figure 4.’ Mariathas and Curzen11 agree that troponin tests can be used to rule-out MI but caution that the manufacturer listed 99th centile level is ‘not the ‘true’ 99th centile for all comers at a hospital, despite the fact that in the vast majority there was no clinical suspicion of MI or myocardial injury.’ That conclude that given the results of the CHARIOT study, ‘we call into question whether using troponin assays outside this clinical context is of real clinical value in most cases, particularly outside the context of a history of cardiac chest pain?’

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Holistic assessment of patients with suspected myocardial injury. ACS, acute coronary syndrome; AMI, acute myocardial infarction.
The Education in Heart article in this issue13 reviews the anatomy, pathophysiology, complications and indications for intervention for atrial and ventricular septal defects, as well as patent ductus arteriosus.
The Image Challenge question14 asks you to make the diagnosis from a colour M-mode echocardiographic tracing; historical perhaps, but illuminates the pathophysiology.
References
Footnotes
Contributors All authors contributed.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.