Article Text

Statistics from Altmetric.com
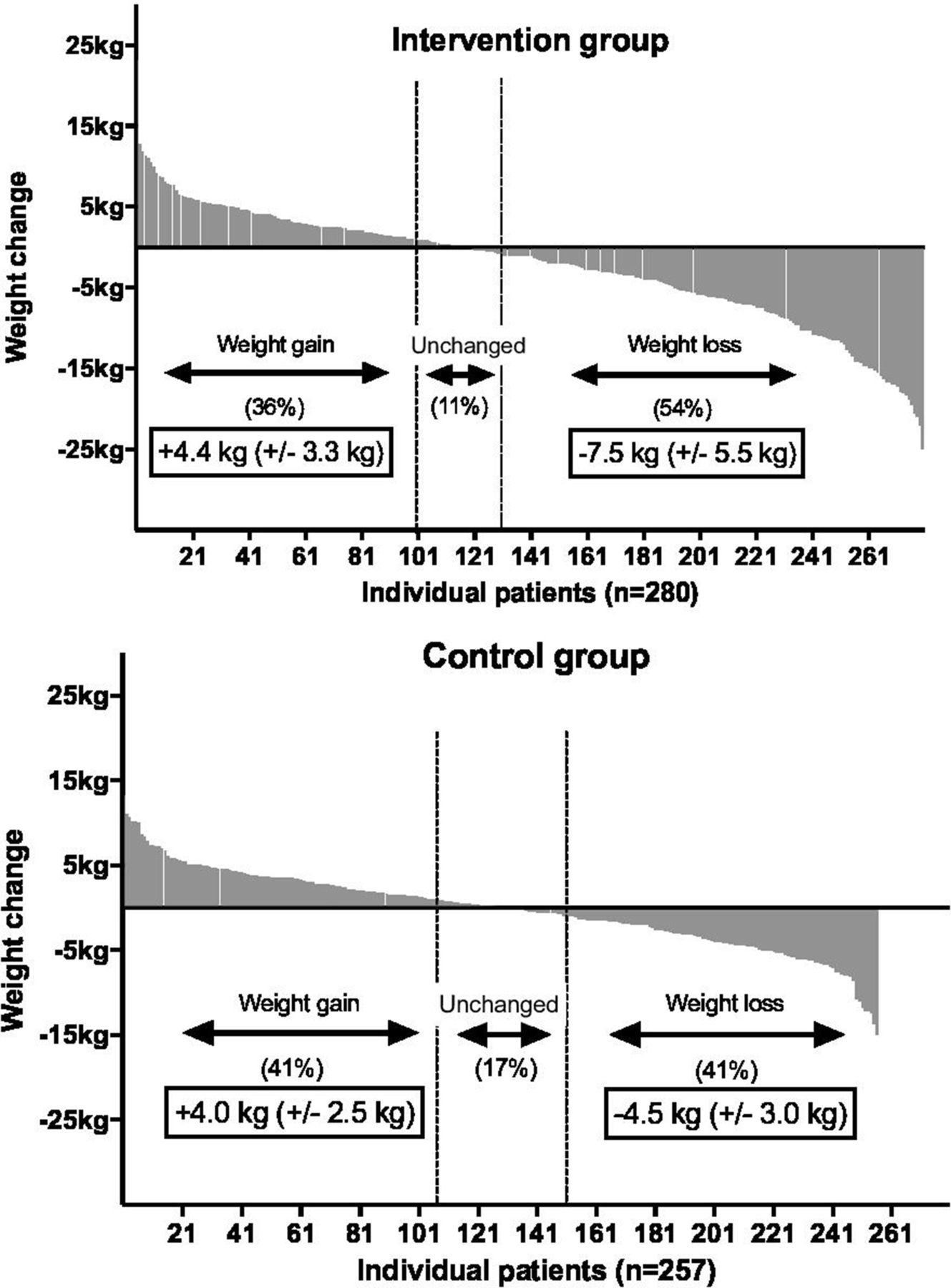
Overweight and obesity are major risk factors for cardiovascular disease (CVD) and meaningful weight loss is associated with a reduction in CVD risk. Yet patients’ efforts at weight reduction often are frustratingly futile. In this issue of Heart, Tijssen and colleagues1 evaluated weight change from baseline to 12-month follow-up in the subgroup of overweight patients (BMI ≥27 kg/m2) with coronary artery disease in the Randomised Evaluation of Secondary Prevention by Outpatient Nurse SpEcialists-2 (RESPONSE-2) multicentre randomised trial. The 280 patients in the intervention arm were offered community-based programmes to achieve weight reduction, increase physical activity and stop smoking in addition usual care, which included cardiology visits, cardiac rehabilitation and counselling on secondary prevention. Although there was wide variation in weight loss for patients in both the intervention and usual care groups, participation in a weight loss programme was associated with weight loss of ≥5% (OR 3.33 compared with usual care) (figure 1). Other factors associated with meaningful weight loss were older age, lower educational level, not smoking and motivation to start weight loss at the baseline visit.
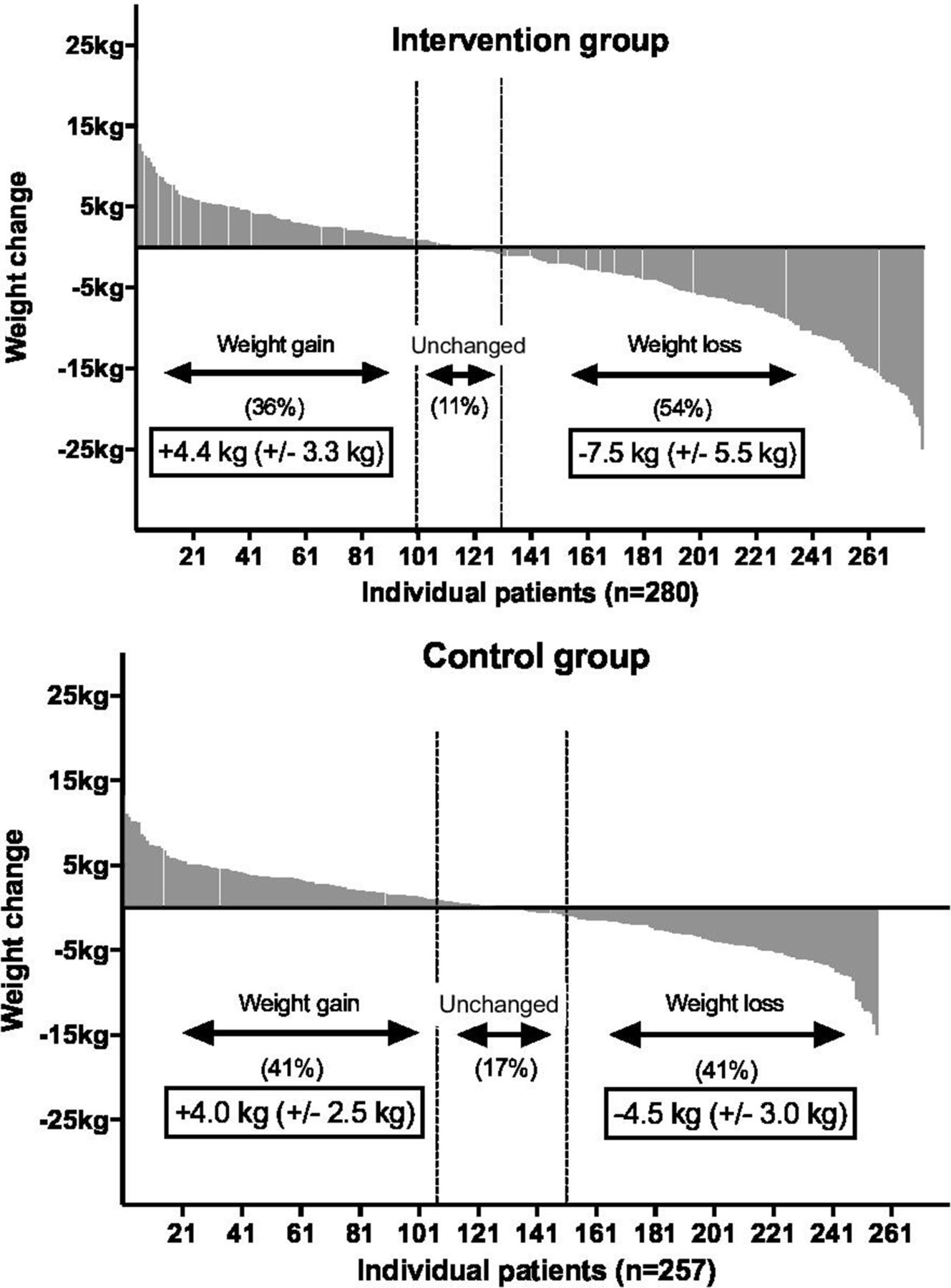
Waterfall plots; weight change from baseline to 12-month follow-up stratified by randomised treatment allocation.
This data supports the wider use of community-based weight loss programmes as a feasible and low cost approach to meaningful weight reduction in our patients with CVD. However, as Kelsey and Pagidipati comment in an editorial2 “Beyond behavioural and psychosocial characteristics, molecular and genetic factors also play a role in response to weight loss interventions” (figure 2). They argue that “Development of a personalised approach can and should match patient to treatment to obtain maximally effective and durable weight loss results.”
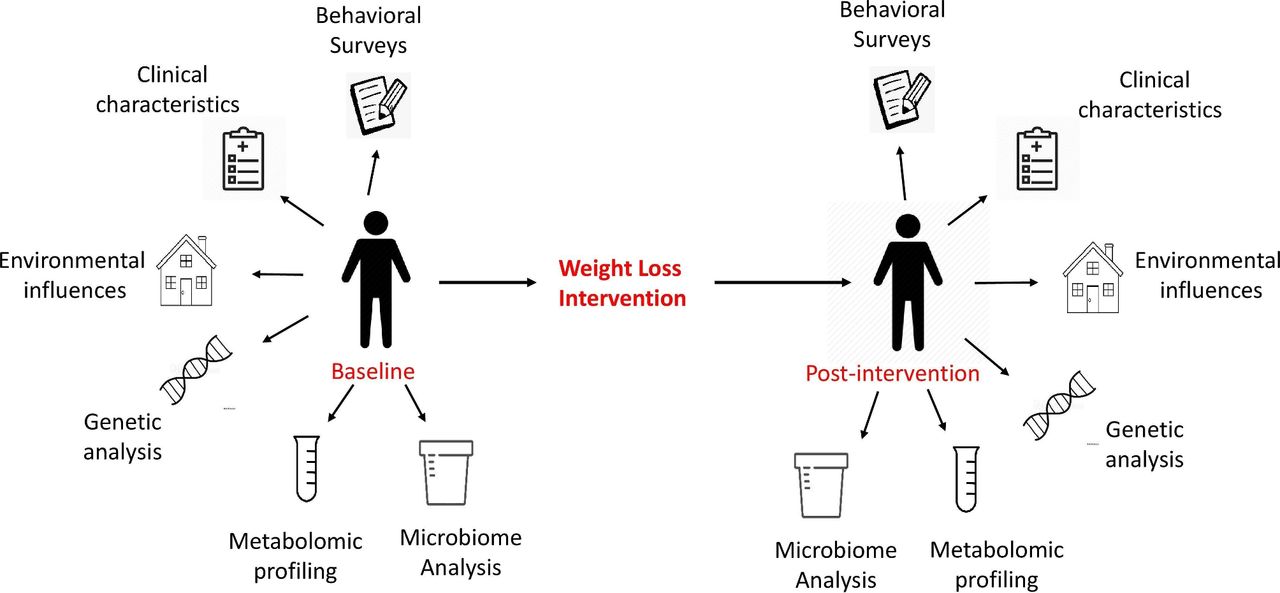
Proposed phenotyping of individuals before and after weight loss interventions.
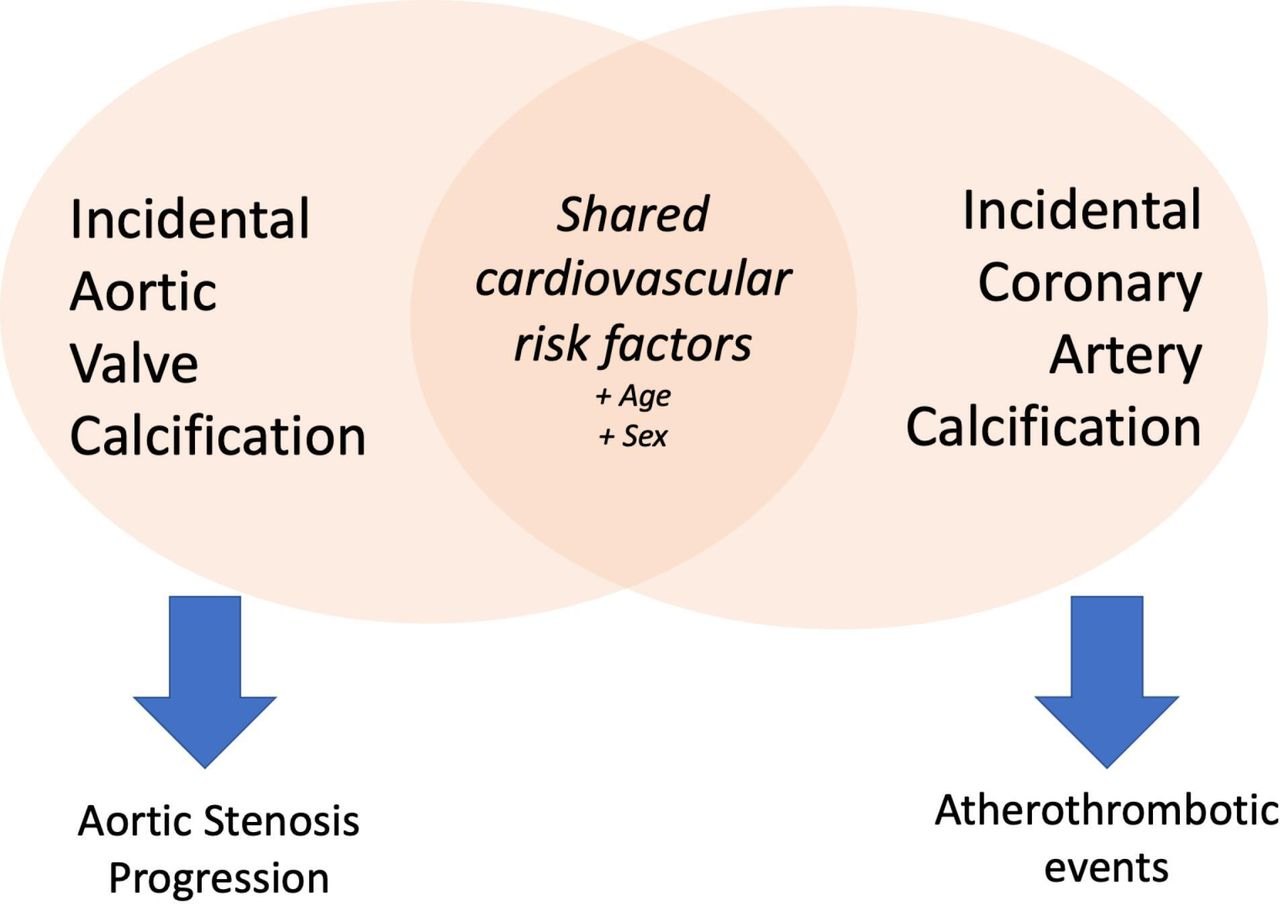
Both coronary artery (CAC) and aortic valve calcification (AVC) are associated with an increased risk of CVD events but it remains unclear whether this simply reflects shared clinical risk factors or whether AVC scores provide additive predictive value, independent of CAC score, for CVD events.3 In a study of 14 073 men aged 60 to 74 years of age in the DANish CArdioVAscular Screening and intervention trial (DANCAVAS), AVC was present in 58% with 1.5% having an AVC score ≥1200 (suggestive of severe aortic stenosis). After accounting for CAC scores, the only CVD risk factors independently associated with AVC were older age, hypertension, obesity, known CVD and serum phosphate levels.
Williams and Dweck4 point out that “90% of patients with aortic valve calcification also had coronary artery calcification, and 62% of patients with coronary artery calcification also had aortic valve calcification.” Putting these findings in context of previous studies, we also know that “while atherosclerosis risk factors are associated with incident aortic stenosis, they are not associated with the propagation phase of the disease and aortic stenosis progression. This is important when considering the development of novel aortic stenosis therapies that will need to slow disease progression rather than initiation if they are to be successful” (figure 3).

Aortic valve calcification and coronary artery calcification share overlapping risk factors, but whether this is due to association or causation remains uncertain.
The study by Buoro and colleagues5 in this issue of Heart provides reference values for normal pericardial fluid that will become a new clinical standard. This data shows that cell counts and levels of protein, albumin and lactate dehydrogenase that are considered inflammatory for other biological fluids are, in fact, normal for pericardial fluid. As Fender and Zack6 comment, “The findings of the study highlight the potential for diagnostic errors when interpretive tools are used outside of their validated purpose.”
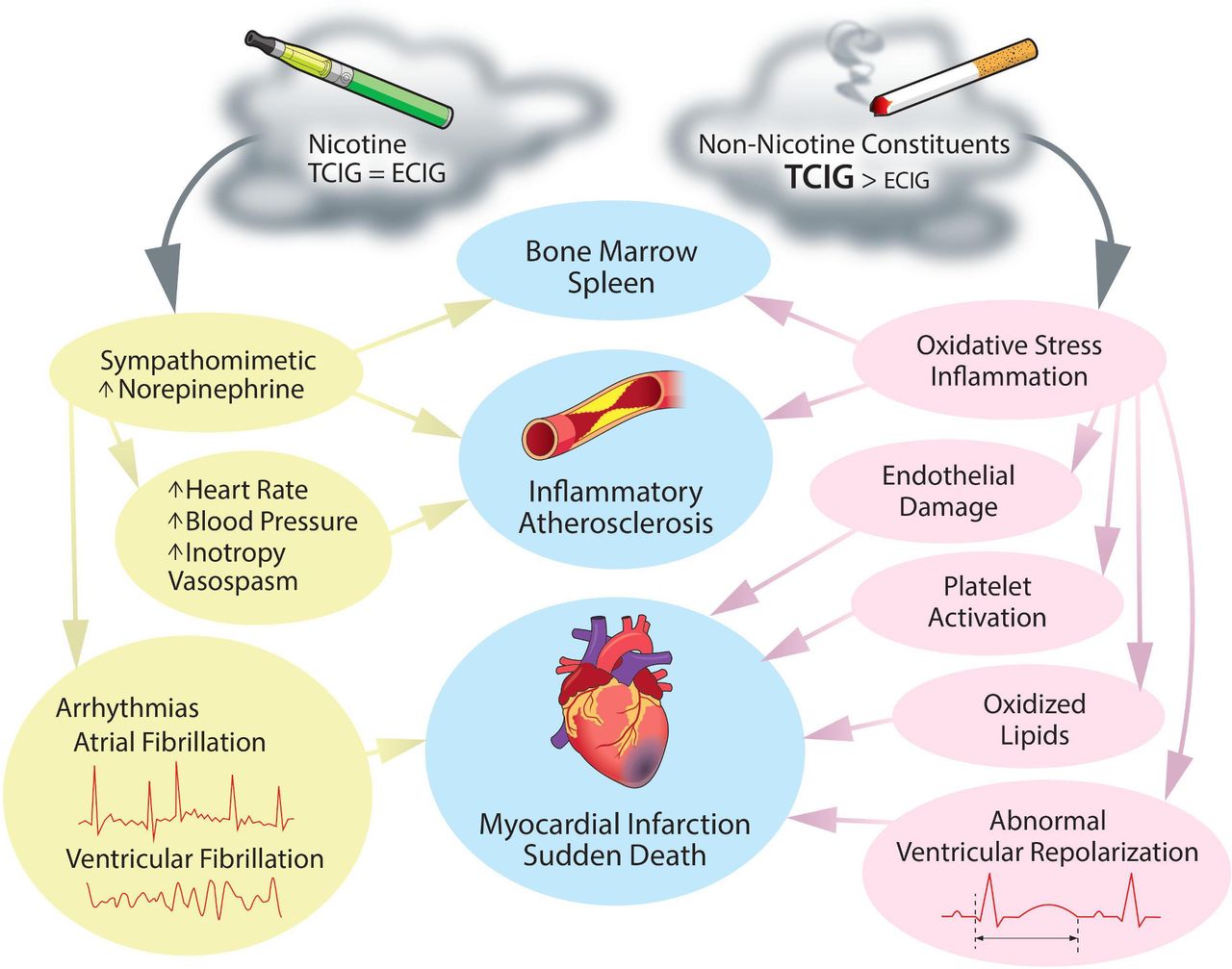
A review article in this issue of Heart by Shahandeh, Chowdhary and Middlekauff7 summarises the published evidence related to vaping and cardiac disease, including potential adverse physiological effects of electronic cigarettes (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cardiovascular effects of tobacco cigarettes (TCIGs) and electronic cigarettes (ECIGs). In considering the cardiovascular risks of tobacco cigarettes and electronic cigarettes, it is best to divide the risks into those largely attributable to nicotine and those largely attributable to non-nicotine constituents in their respective emissions. Cardiovascular effects associated with nicotine are attributable to nicotine’s sympathomimetic effects, including increases in heart rate, blood pressure and inotropy, potentially accompanied by vasospasm, leading to ischaemia. Additionally, increased sympathetic tone is linked to heightened risk of arrhythmias, both atrial and ventricular. Increased sympathetic tone may be the instigator of activation of the splenocardiac axis, increasing inflammation, and once again increasing the risk of inflammatory atherosclerosis and ischaemia.25 Potential cardiovascular effects of non-nicotine constituents include increased oxidative stress and inflammation, leading to endothelial damage, platelet activation and lipid oxidation, increasing the risk of inflammatory atherosclerosis and ischaemia. Further, non-nicotine constituents may have adverse effects on ventricular repolarisation, once again increasing the risk of arrhythmias.
The Education in Heart article8 in this issue reviews the diagnosis and management of cardiac sarcoidosis with useful clinical algorithms and examples of imaging findings.
Be sure to take a look at the short Cardiology-in-Focus article 9 announcing the winner and finalists for the 2021 Heart Best Research Paper Award. Join me in congratulating these investigators on their dedication to the highest research standards and the value of their clinical research data.
Ethics statements
Patient consent for publication
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; internally peer reviewed.