Article Text

Statistics from Altmetric.com
Sex differences in clinical management and outcomes of patients with cardiovascular disease sometimes are due to healthcare inequities (which should be eliminated) but also might be due to sex-related differences in aetiology and pathophysiology. For example, the optimal medical dose for management of heart failure with reduced ejection fraction (HFrEF) may be lower in women compared with men. In a study of 561 women and 615 men with a new diagnosis of either HRrEF or heart failure with preserved ejection fraction (HFpEF), Bots and colleagues1 found that although 79% of women and 86% of men with HFrEF were prescribed an ACE inhibitor (ACEI) or angiotensin receptor blocker (ARB), the average dose was only about 50% of the recommended target dose for both sexes. A lower ACEI/ARB dose was associated with higher survival outcomes in women, but not men, with HFrEF. In patients of both sexes with HFpEF, there was no relationship between medication dose and survival (figure 1).

Central figure summarising the design and main findings of this study.
In the accompanying editorial, Hassan and Ahmed 2 comment that: ‘Sex differences in HF outcomes may be further exacerbated by differences in medication pharmacokinetics and pharmacodynamics, with female-specific physiological factors including lower body mass, as well as decreased renal excretion and gastrointestinal enzymatic activity, leading to higher medication bioavailability. As a result, the administration of sex-neutral medication doses leads to greater drug exposure in female patients, which may subsequently lead to a higher incidence of adverse drug reactions. This raises the possibility of sex-based HF treatments to improve clinical outcomes. However, current guidelines adopt a ‘one size fits all’ approach, with an emphasis on target-dosed therapy. In this era of precision medicine, is it time to redefine optimal HF therapy based on the sex of the patient?’
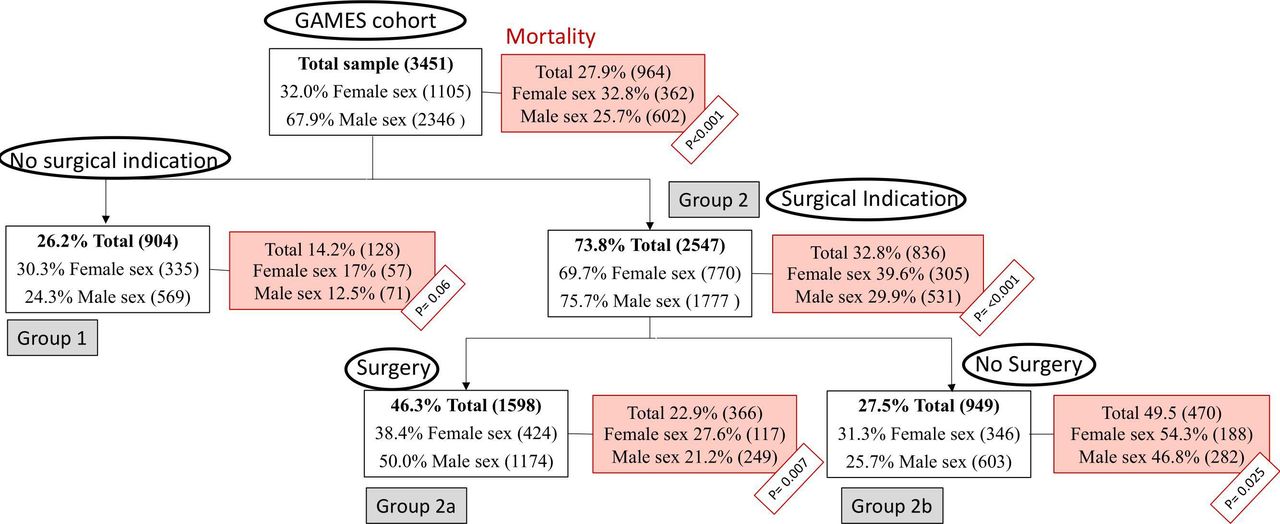
On the other hand, adverse outcomes in women with infective endocarditis likely are related to bias and healthcare inequities. In a multicentric Spanish cohort of 3541 patients3 diagnosed with endocarditis between 2008 and 2018, women underwent surgical intervention less often than men (38.3% vs 50%) despite the increasing recognition that earlier surgical intervention often is beneficial as recommended in current guidelines (figure 2). The lower likelihood of surgery in women persisted after propensity matching for age and surgical risk (OR 0.74; 95% CI 0.59 to 0.91; p=0.05). In addition, women had a higher in-hospital mortality compared with men, even after adjusting for possible confounders (OR 1.41; 95% CI 1.21 to 1.65; p<0.001).

Stratification of the GAMES (‘Grupo de Apoyo al Manejo de la Endocarditis Infecciosa en España’ or ‘Spanish Collaboration on Endocarditis’) cohort according to surgical recommendation between sexes. Overall and stratified mortality is displayed in each group.
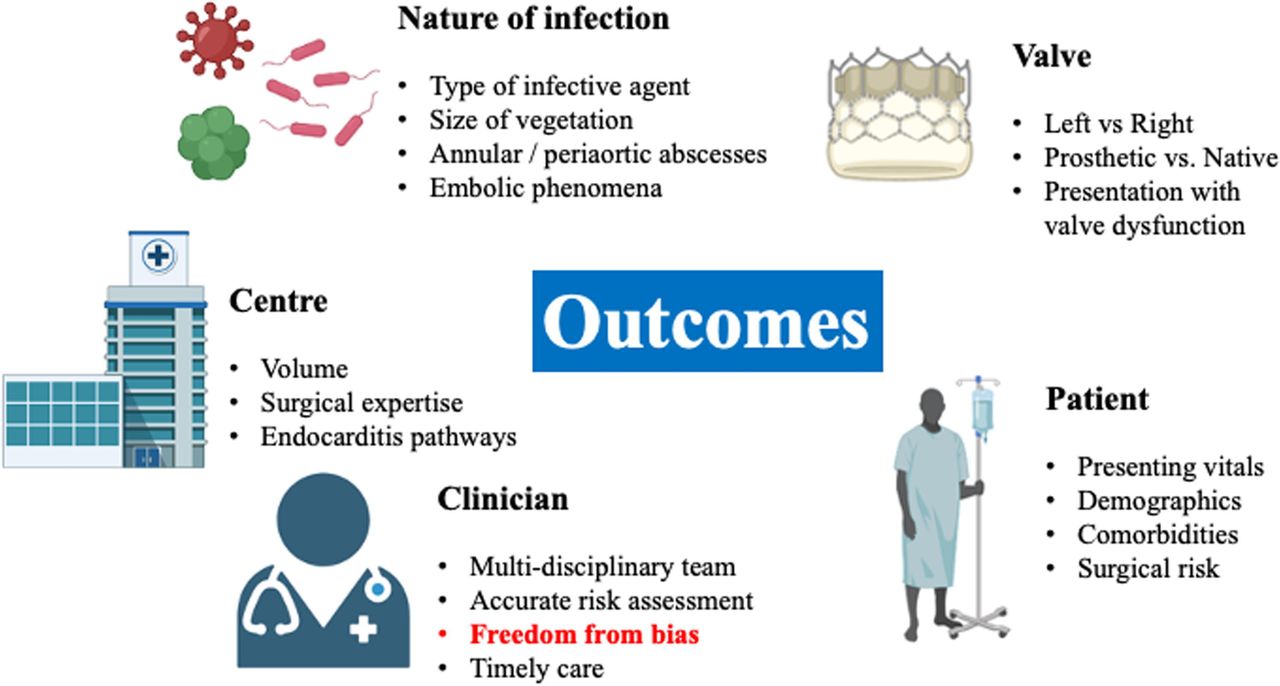
Van Spall, Jaffer and Mamas4 remind us of the many factors to be considered in the decision to recommend surgical intervention in a patient with endocarditis (figure 3). However, as they conclude: ‘Disparities in referral and receipt of surgical intervention, along with differences in aetiology, microbiology and comorbidities, may be responsible for the higher risk of mortality in women than in men with IE. Ultimately, awareness of these issues should prompt a self-evaluation of biases on the part of clinicians such that objective, timely surgical referrals are made and interventions are offered regardless of demographic group. While the biology is not modifiable, the biases and care disparities are.’

{kind=link}
{kind=link}
{kind=link}
Factors associated with infective endocarditis outcomes.
Another interesting paper in this issue is the study by Sung and colleagues5 showing a positive, graded association between higher levels of physical activity and a higher prevalence, with more rapid progression, of coronary artery calcification (CAC). These findings were based on a cohort of 25 485 Korean men and women with a median interval between CAC measurements of 3 years. In discussing these seeming paradoxical findings, Gulsin and Moss6 point out that although CAC is a surrogate marker for calcified atherosclerosis and is associated with a higher risk of myocardial infarction, treatment with a statin also accelerates deposition of calcified plaque, similar to the effects of physical activity in the current study. They also remind us that: (1) the severity of CAC at baseline is a key predictor of progression rates, (2) an increase in CAC score is not the same an accelerated rate of total atherosclerotic plaque progression, and (3) the risk of plaque rupture and clinical events is greatest within the necrotic core of noncalcified plaques. Thus, it is possible that an increase in CAC scores reflects a protective response and a transition to a more stable plaque morphology rather than more extensive atherosclerosis. They conclude: ‘Sung and colleagues5 have produced a timely manuscript that highlights the complexity of interpreting coronary artery calcium scores in patients who have implemented recommendations on physical activity or commenced on statin therapy. While proponents would argue that it is an effective tool to screen for subclinical atherosclerosis in asymptomatic individuals, clinicians should be cautious regarding the overuse of this test in otherwise healthy individuals. The coronary artery calcium paradox should not result in paradoxical care for our patients.’
The Education in Heart article7 in this issue provides an overview for clinicians to detect and manage mental issues in their patients with cardiovascular disease (CVD) . There is a reciprocal relationship between mental disorders and CVD: patients with mental disorders have a 1.5- to 3.0-fold higher risk of developing CVD and, conversely, the onset of CVD increases the risk of a developing a mental disorder by 2.2-fold.
The Cardiology in-Focus topic in this issue is a step-by-step guide to writing a Image Challenge question, authored by our Image Challenge Editor.8 We encourage both cardiology trainees and clinicians to submit Image Challenge questions to Heart, using this basic guide, because this type of question accelerates learning for both the author and the reader (table 1).
Key components of an image challenge question
Ethics statements
Patient consent for publication
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; internally peer reviewed.