Article Text

Abstract
Objective Treatment of acute myocardial infarction (MI) requires rapid transfer of people with chest pain to hospital, however, unscheduled care pathways vary in their directness (the minimal number of contacts to hospital admission). The aim was to examine unscheduled care pathways and the associations with mortality in people admitted with MI.
Methods Retrospective population study of all people admitted to Scottish hospitals with a diagnosis of MI between 1 January 2015 and 31 December 2017. Linked data for all National Health Service Scotland unscheduled care services (NHS24 telephone triage service, primary care out of hours, ambulance, emergency department (ED)) was used to define continuous unscheduled care pathways (pathways), which were categorised by initial contact, and whether they were ‘direct’ (had minimum number of contacts between first contact and admission). Analysis estimated ORs and 95% CIs in adjusted models in which all covariates were included.
Results 26 325 people admitted with MI (63.1% men, 61.6% aged 65+ years), of whom 5.6% died from coronary heart disease within 28 days. For 47.0%, the first unscheduled care contact was ambulance, 23.3% attended ED directly and 18.7% called telephone triage. 92.1% of pathways were direct. Pathways starting with telephone triage were more likely to be indirect compared with other initial contacts (adjusted OR (aOR) 1.97, 95% CI 1.61 to 2.40). Compared to direct pathways, indirect pathways starting with telephone triage were associated with higher mortality (aOR 1.97, 95% CI 1.61 to 2.40) as were indirect pathways starting with another service (aOR 1.55, 95% CI 1.19 to 2.01), but not direct pathways starting with telephone triage (aOR 0.87, 95% CI 0.74 to 1.02).
Conclusion Unscheduled care pathways leading to admission with MI in Scotland are usually direct, but those starting with telephone triage were more commonly indirect. Those indirect pathways were associated with higher mortality.
- Myocardial Infarction
- Telemedicine
- Quality of Health Care
- Delivery of Health Care
Data availability statement
Data are not publicly available but may be obtained from the Data Controller - Public Health Scotland electronic Data Research and Innovation Service (eDRIS).
Statistics from Altmetric.com
Introduction
Case fatality rate and overall mortality due to myocardial infarction (MI) have reduced over the past 20 years, although MI remains a significant cause of mortality.1 Improved diagnostics2 3 and reduced time to effective treatment have contributed to this reduction, through the standardisation of care pathways and treatment algorithms.4 The UK National Institute of Clinical Excellence (NICE) recommends percutaneous coronary intervention (PCI) within 12 hours of symptom onset for patients with ST elevation myocardial infarction (STEMI) and immediate coronary angiography for unstable patients with non-STEMI or unstable angina.5 All age groups are thought to benefit from an early invasive strategy,6 7 and delays to recommended care are associated with increased mortality.8
Atypical symptoms, multimorbidity and complex care needs impact how care is accessed, as well as timely diagnosis.8–10 Older populations are less likely to get PCI despite proven benefits.10 In addition, atypical symptoms may delay recognition of serious problems by patients and professionals, leading to treatment delays,11 12 while increased use of telephone triage has the potential to increase the number of healthcare contacts and delay diagnosis.13–15
Sources of delay include how patients access unscheduled care (UC) and the number and pattern of service contacts they have prior to hospital admission. Many patients with chest pain choose to call an ambulance or attend emergency departments (EDs) directly meaning they have rapid access to definitive diagnosis, but in the UK many use telephone triage services.13 During the current pandemic, there has been an increased use of telephone triage,16 and the National Health Service (NHS) in England now aims for NHS telephone triage to be the primary route into UC, with an ‘expectation’ that 70% of those triaged to attend the ED by NHS telephone triage will receive a booked time slot.17 Similar changes have happened in other UK countries during the COVID-19 pandemic.
Understanding UC pathways for people diagnosed with MI, and associated outcomes, is important for informing future design of UC services, particularly if ‘telephone first’ strategies persist after the pandemic.18 The aim of the study was, therefore, to examine direct and indirect pathways to care, in the context of the initial UC service contacted and associations with mortality in all patients admitted to a hospital with an MI in the years 2015 to 2017.
Methods
Study design and data sources
The study is a retrospective, population study using the Scotland-wide Unscheduled Care DataMart (UCD), which links data from NHS24 telephone advice and triage (the Scottish NHS telephone triage service), the Scottish Ambulance Service, Primary-Care-Out-of-Hours (PCOOH), EDs, emergency acute hospital admissions (Scottish Morbidity Records 01 (SMR01)), mental health admissions (SMR04) and National Records of Scotland (NRS) death registration. The Community Health Index (the NHS Scotland unique patient identifier) number was used to link episodes of care across all datasets. Linkage was carried out by NHS Scotland Information Services Division. Data on contacts is electronically collected by all services and is complete.19 A continuous UC pathway (pathway) is a series of UC contacts for a single person.19 Pathways terminate when there is no further contact with any UC service for 24 hours. Each emergency and urgent care service is assigned a code letter: N=NHS24 telephone triage, O=Primary-Care-Out-of-Hours, S=Scottish Ambulance Service, E=Emergency Department, A=Acute hospital emergency-admission. Pathway names are the chronological sequence of contacts. For example, the pathway NOSEA represents NHS24 telephone triage, followed by Primary-Care-Out-of-Hours (O), then Scottish Ambulance Service, then ED attendance terminating with an acute hospital emergency admission.
Setting and patients
The cohort consisted of all patients admitted to Scottish hospitals between 1 January 2015 and 31 December 2017 with MI (defined as ICD-10 codes I21 and I22 recorded as the primary discharge diagnosis). Demographic information, the pathway before admission, whether the patient had been admitted with a previous MI, and mortality data from National Records Scotland were then linked.
Outcomes
Two outcomes were examined: (1) whether the initial UC service was with NHS24 telephone triage or another UC service (ED, ambulance, PCOOH or direct medical admission) and (2) death from coronary heart disease (defined as ICD-10 code I20–I25 recorded as underlying cause of death) within 28 days of admission date.
Other variables
In both analyses, other variables examined were age (in 5-year increments but with <50 years and >80 years combined because of small numbers), sex, patient socioeconomic status (SES) (defined by the Scottish Index of Multiple Deprivation (SIMD) grouped into quintiles), urban/rurality (defined by the Scottish Executive Urban Rural Classification (SEURC) grouped into primary city/urban, accessible, remote and very remote, where the latter three categories are defined by drive time to an urban area of <30 min, 30–60 min and >60 min respectively) and whether the patient had experienced a previous MI.
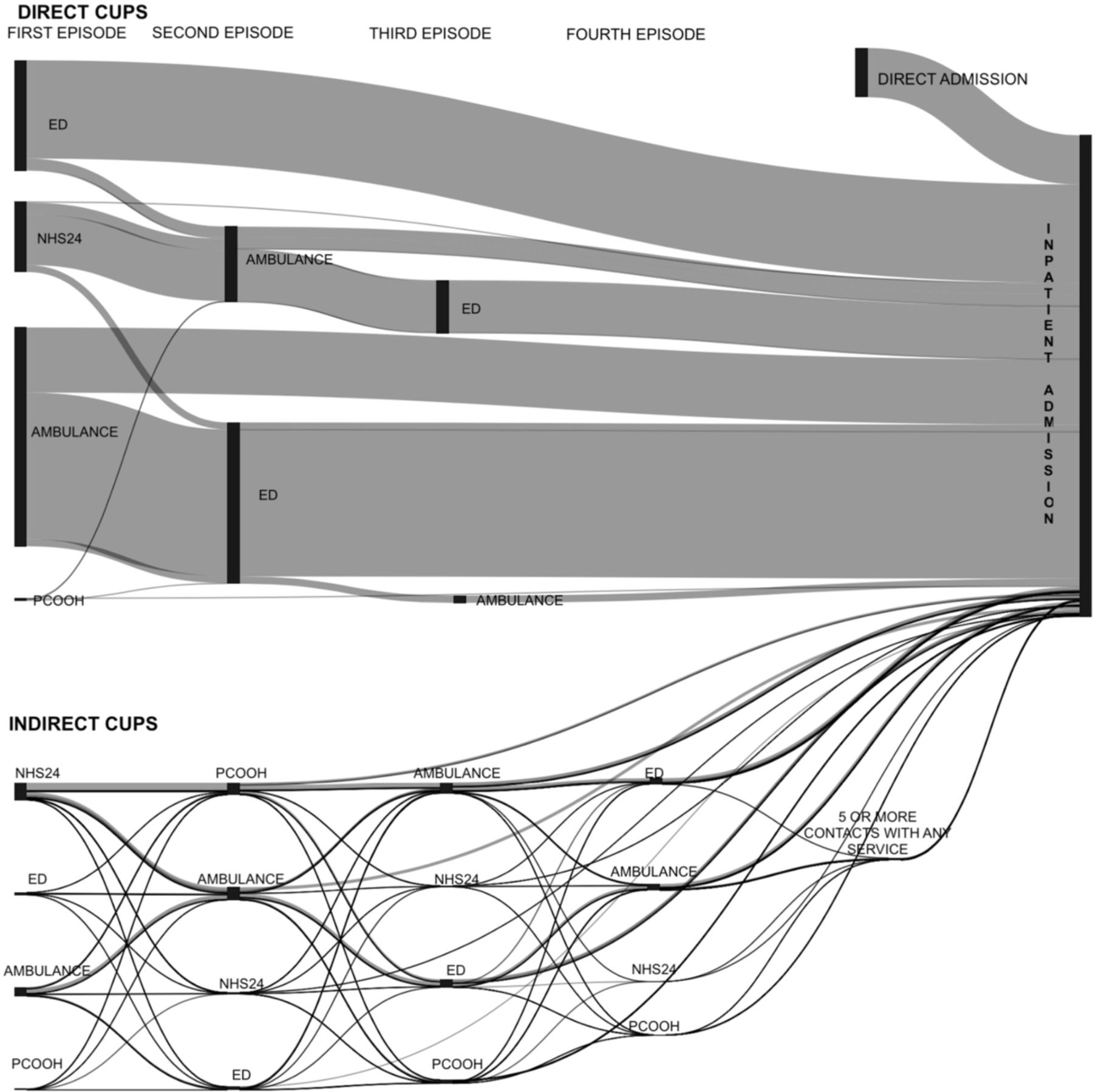
For the mortality analysis, pathways were categorised based on whether they were considered ‘direct’ or ‘indirect’. The number of service contacts before admission varies depending on which service the patient initially accesses. The assumption was made that a higher number of contacts results in an increased time to treatment, and so pathways were defined as direct if they used the minimal number of contacts before admission for each type of initial contact and otherwise as indirect (more than the minimal number of contacts). For example, the pathway ‘SEA’ is direct, as the patient calls an ambulance, attends ED and is admitted, whereas the pathway ‘SEEA’ is indirect as two separate ED attendances occur before inpatient admission. Similarly, the pathway ‘NSEA’ is ‘direct’ as the patient chooses to call NHS24 telephone triage and is then taken by ambulance to ED and admitted, whereas the pathway ‘NOSEA’ is ‘indirect’ as a PCOOH attendance is an additional contact with a service which cannot make a definitive diagnosis (although it may help avoid unnecessary ED attendances by those without MI). Of the 370 unique patterns of pathway observed, 15 were direct and 355 indirect (table 1 and figure 1). Direct and indirect pathways were further categorised based on whether the initial service contacted was NHS24 telephone triage or another UC service.

{kind=link}
Unscheduled care pathways leading to inpatient admission with myocardial infarction. ED, emergency department; PCOOH, primary-care-out-of-hours.
Direct and indirect pathways
Data analysis
Data were managed and analysed using R V.3.6.1 and SPSS V.24. Demographics were described using summary statistics, and pathways between initial UC contact and admission with MI examined. For the binary outcome variables (death and NHS24 telephone triage initial contact vs another UC initial contact), logistic regression modelling examined associations between outcomes and sex, age group, SIMD, SEURC and previous MI; and for the mortality analysis, pathway type (direct vs indirect). The dataset was complete for all variables other than SIMD and SEURC, for which 198 cases (0.75%) had missing data. These were excluded from analysis given the small number. Analysis estimated ORs and 95% CIs in both univariate (unadjusted) models and adjusted models in which all covariates were included. Multicollinearity and model fit were assessed for with Nagelkerke R squared and Akaike information criterion (online supplemental appendix 1).
Supplemental material
Patient and public involvement
No patient or public involvement.
Results
Of 26 325 hospital admissions with a primary diagnosis of MI, 63.1% were for men (table 2). Almost one in ten (8.9%) of admissions were in people aged <50 years, 61.6% in people aged 65+ years, 25.0% in people aged 80+ years (table 1). People living in the most deprived 20% of postcodes comprised 24.1% of MIs, compared to 15.3% in those in the least deprived quintile. Two-thirds (68.4%) lived in an urban area compared with 4.2% living in a remote area. Previous MI was recorded in 16.6% (table 2).
Characteristics of patients admitted to hospital with MI
For 47.0% of patients, the first contact with UC was an ambulance call, 23.3% attended the ED directly, 18.7% called NHS24 telephone triage, 10.1% had a direct inpatient admission (assumed to be the result of a daytime GP emergency referral) and 0.8% presented directly to PCOOH (which is allowed in some areas although not encouraged) (table 3) (figure 1). Half of pathways were either ‘SEA’ (ambulance→ED→admission—29.9%) or ‘EA’ (ED→admission—20.1%) (table 3), 81.3% consisted of three or less UC contacts (including admission), 14.8% four contacts and only 3.9% ≥5 contacts. In total, the 15 direct pathways accounted for 24 244 (92.1%) of all pathways, whereas the 355 indirect pathways accounted for 2081 (7.9%) (figure 1). Pathways beginning with an ED attendance were direct in 96.7% of cases, and those that began with an ambulance were direct in 94.9%. In comparison, 76.9% of pathways starting with NHS24 telephone triage were direct compared with 62.0% of those starting with a PCOOH attendance (table 3).
Characteristics of continuous unscheduled care pathways before admission with myocardial infarction
Associations of patient characteristics and prior unscheduled care pathway with mortality from CHD within 28 days of admission
Initial descriptive analysis showed a greater proportion of men with MI attended the ED directly, whereas a greater proportion of women had an initial telephone triage contact. A higher proportion of people with MI living in very remote areas had a first contact with NHS telephone triage compared with urban counterparts. Proportionally more younger people with MI had a first contact with the ED compared with older patients, more of whom contacted NHS24 telephone triage or an ambulance (table 1). On logistic regression analysis, people over 80 years of age were more likely to call NHS24 telephone triage as their first UC contact (compared with those aged 55–59 years, adjusted OR (aOR) 1.21, 95% CI 1.08 to 1.36) (table 4). Those living in the most affluent areas were more likely to call NHS24 telephone triage as their initial point of contact (aOR 1.16 (1.05 to 1.29) compared with those living in the least deprived areas), as were women (aOR 1.36 (1.27 to 1.45)) and those living in the most remote areas (aOR 0.70 (0.58 to 0.83) compared with those living in cities).
Associations of patient characteristics with choice of NHS24 as first UC contact
In total, 5.6% people admitted with MI died from coronary heart disease within 28 days of admission (table 5). Compared with direct pathways starting in any service except NHS24 telephone triage (other direct), direct pathways starting with NHS24 telephone triage were not associated with increased mortality (aOR 0.87 (0.74 to 1.02)) (table 5). Indirect pathways that began with another UC service were associated with increased mortality (aOR 1.55 (1.19 to 2.01)), with indirect pathways starting with NHS24 telephone triage having the highest odds of mortality (aOR 1.97 (1.61 to 2.40)). Increasing age was associated with large increases in mortality, with a stepwise increase from 1.3% aged <50 years dying to 12.3% of those aged ≥80 years (aOR 8.36, CI 6.16 to 11.35 compared with age group 55–59 years). In unadjusted analysis, there was no association between socioeconomic deprivation and mortality, but in adjusted analysis those living in the least deprived areas had lower odds of mortality (aOR 0.82 (0.69 to 0.98)) compared with those living in the most deprived areas. There was no association between remoteness from an urban centre and mortality. In unadjusted analysis, women had an increased odds of mortality (OR 1.53 (1.37 to 1.69)), although this was smaller and not statistically significant after adjusting for other variables (aOR 1.07 (0.96 to 1.20)).
Discussion
Summary
One in twenty (5.6%) patients diagnosed with MI died from coronary heart disease within 28 days of hospital admission. Notably, indirect pathways that began with NHS24 telephone triage were associated with the highest mortality, followed by indirect pathways initiated by contact with another UC service. Increasing age was associated with higher mortality, as was living in the most deprived areas, but living in remote areas was not.
Most (92.1%) patients had a direct route to definitive care regardless of which service they chose to initially contact, with five direct pathways (SEA, EA, SA, NSEA, A), out of a total of 15 direct pathways, accounting for 83.6% of all patient journeys. Differences in the characteristics of people with MI were noted in terms of choice of NHS24 telephone triage as the first point of UC contact. Men, people living in more deprived areas, those who had had a previous MI and those living most remotely were the least likely to call NHS24 telephone triage as their first UC contact. In contrast, older people (aged >80 years) were more likely to call NHS24 telephone triage first, although also more likely to call an ambulance first and less likely to attend ED first compared with other age groups.
Strengths and limitations
The key strength of the study is that the UCD allows for a comprehensive analysis of linked UC attendances for the entire Scottish population. However, we cannot be certain that linked episodes in a pathway are actually for the same problem, since pathways are defined as sequential episodes over a short period of time regardless of why the person calls or attends. This means that certain pathways may have been indirect in practice, such as separate attendances at an ED (Emergency Department→Ambulance→Emergency Department→Admission), but were considered direct as it was thought they more likely represented an inter-hospital transfer given the rural nature of many of Scotland’s hospitals. A further weakness is that in only including patients admitted to hospital, those who die from MI prior to admission are not counted. Furthermore, in not including patients who have symptoms suggestive of MI but do not receive a diagnosis, a full analysis of the triage process is not possible. Non-ST elevation myocardial infarction (NSTEMI) is common in older people with multimorbidity and has more atypical presentations, both of which would be expected to be associated with ‘indirect’ pathways and higher mortality. However, hospital discharge coding does not reliably distinguish between STEMI and NSTEMI, meaning we cannot explore this. A further limitation is that information on individual cardiovascular risk factors and presenting symptoms was not included, the prevalence of which may influence associations with mortality. This underscores the fact that claims of causality cannot be made. Previous MI was included but the risk of selection bias was present since such patients may be more likely to seek medical attention in the first place and more likely be assessed for potential MI. Finally, the exact time of a person’s first contact with unscheduled was not available, meaning that while it may be inferred that indirect pathways can lead to treatment delays, this could not be precisely quantified.
Comparisons with existing literature
The mortality rate is in keeping with other studies20 21 as is the ratio of men to women in terms of incidence of MI and mortality.1 22 23 The associations between increasing age and lower SES have been found previously.22–24 Differences include a previous finding that men with symptoms of MI were more likely to call an ambulance25 as opposed to little difference in this study, and a previous study showing older patients had decreased use of NHS24 telephone triage, although it did include all calls.26 Public health campaigns have been effective in raising awareness among the public of typical symptoms of MI and the importance of seeking prompt treatment.27 Men and younger people are more likely to experience typical symptoms,9 which likely explains some of the patterns of UC use observed here. However, other contextual factors are also likely to be at play, including transport and mobility issues which may underlie the observation that younger people were more likely to attend ED as first contact, whereas older people were more likely to call NHS24 telephone triage or call an ambulance. It is unsurprising that age is associated with increased odds of mortality given the increased levels of frailty, multimorbidity and increased likelihood of atypical symptoms making initial diagnosis more difficult.1
Implications for research and practice
As we emerge from the current COVID-19 pandemic, the findings have implications for how UC services are organised in the future. The NHS ‘Think 111’ campaign is encouraging the public to use telephone triage as a single point of access for all UC services, with the aim of managing patient flow and avoiding crowded waiting rooms, and NHS England intends NHS telephone triage to be the primary route into UC in the future.17 In a younger cohort, triage of chest pain by NHS24 telephone triage has been shown to be effective13 but in higher risk populations, caution is required to ensure triage does not inadvertently lead to either more complex UC pathways and treatment delays in people with MI or increasing numbers of people without MI being sent to the ED for urgent assessment.
The question of why pathways that begin with NHS24 telephone triage are more likely to be indirect with higher mortality, and whether this is related to patients having atypical symptoms, or to having complex multimorbidity and alternative anticipatory care plans, is an area for future research, as does the possibility that the relationship between telephone triage and mortality is causal. In addition, this paper has analysed those admitted to hospital with MI but research into the UC contacts of those who die from MI prior to admission is required to give a fuller picture of initial service contact in relation to mortality. Furthermore, NHS24 telephone triage and PCOOH do not have access to diagnostic tools such as troponin and ECG. Pre-hospital use of these investigations by emergency medical services has been shown to aid conveyance decisions,28 but further research is needed as to whether access to point-of-care troponin in ambulance services and PCOOH would improve outcomes and reduce referrals. Research is also needed to examine the characteristics and outcomes of patients that each service discharges as well as those that are referred to other UC services for further assessment, particularly if telephone triage is to become the single point of entry for those attempting to access UC. Finally, there are other service level factors which will influence mortality, such as rates of invasive coronary angiography and rates of prescription of medical therapy. Future research utilising data linkage to investigation and prescribing data may help further elucidate the impact of indirect pathways on mortality.
Conclusion
This study found that 92.1% of people admitted to hospital with MI have a direct pathway to inpatient admission irrespective of which service they first contact. Indirect pathways that began with NHS24 telephone triage were associated with the highest mortality, followed by indirect pathways initiated by contact with another UC service. Increasing age had the biggest overall influence on mortality. Further research to understand the safety and effectiveness of telephone triage services is required if they are to become the single point of access for UC.
Key messages
What is already known on this subject?
Myocardial infarction (MI) remains a significant cause of death despite improved diagnostics and reduced time to effective treatment.
Unscheduled care pathways can be complex and have the potential to lead to treatment delays.
The COVID-19 pandemic has led to increased use of telephone triage in unscheduled care.
What might this study add?
Most care pathways had the minimum number of unscheduled care interactions expected between first service contacted and hospital admission with MI.
Care pathways that involved more than a minimum number of unscheduled care contacts were associated with higher mortality from MI, particularly if the initial service was NHS24.
How might this impact on clinical practice?
In patients with atypical symptoms for MI, or complex care needs, caution is required to ensure telephone triage does not inadvertently lead to either an increase in unscheduled care contacts or delays to accessing appropriate treatment.
Data availability statement
Data are not publicly available but may be obtained from the Data Controller - Public Health Scotland electronic Data Research and Innovation Service (eDRIS).
Ethics statements
Patient consent for publication
Ethics approval
Public Benefit and Privacy Panel for Health and Social Care approval was granted to the project (reference 1617/0307).
Acknowledgments
NHS Scotland and Public Health Scotland for providing the Urgent Care Datamart.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @PeteHodgins
Contributors PH and BG conceived the idea for the study and were the main authors. MM provided data management and statistical analysis. Expert review was provided by AS, MJR and SM. BG is responsible for the overall content as guarantor.
Funding The study was funded by the University of Edinburgh.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.