Article Text

Abstract
Magnetic Resonance Imaging (MRI) is increasingly a fundamental component of the diagnostic pathway across a range of conditions. Historically, the presence of a cardiac implantable electronic device (CIED) has been a contraindication for MRI, however, development of MR Conditional devices that can be scanned under strict protocols has facilitated the provision of MRI for patients. Additionally, there is growing safety data to support MR scanning in patients with CIEDs that do not have MR safety labelling or with MR Conditional CIEDs where certain conditions are not met, where the clinical justification is robust. This means that almost all patients with cardiac devices should now have the same access to MRI scanning in the National Health Service as the general population. Provision of MRI to patients with CIED, however, remains limited in the UK, with only half of units accepting scan requests even for patients with MR Conditional CIEDs. Service delivery requires specialist equipment and robust protocols to ensure patient safety and facilitate workflows, meanwhile demanding collaboration between healthcare professionals across many disciplines. This document provides consensus recommendations from across the relevant stakeholder professional bodies and patient groups to encourage provision of safe MRI for patients with CIEDs.
Statistics from Altmetric.com
Scope
The aim of this joint multiprofessional societal guidance is to provide consensus recommendations for best practice management of patients with cardiac implantable electronic devices (CIEDs), who require investigation using MRI in the UK. With representation from all involved in the patient pathway (including patients), we aim to highlight areas of clear recommendations which should be adhered to, alongside consensus recommendations where no current guidelines exist or are perceived to conflict. This document provides a recommended protocol and workflow alongside specific guidance for the different personnel involved in the clinical pathway, outlining relevant responsibilities and procedures. Additionally, the risks associated with scenarios where particular conditions of MR Conditional CIEDs are not met or where the CIED system does not currently have regulatory approval to undergo MRI are summarised, to aid a local decision to scan patients in these scenarios where the clinical benefit outweighs the risk (figure 1). Suggested statements for consent of these patients are also provided. For each section throughout this document, points are presented as statements with distinction made between mandated and consensus recommendations.

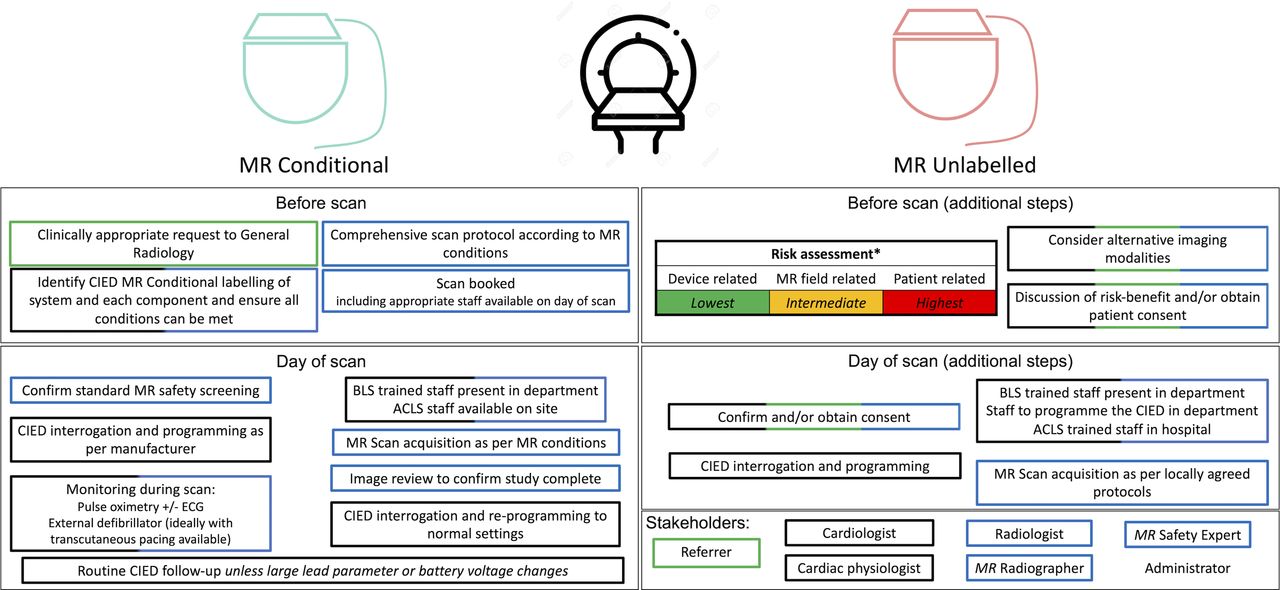
Recommendations for MRI workflows in patients with cardiac implantable electronic devices. *Higher risk scenarios include the presence of fractured, epicardial, abandoned leads; recent implantation; battery at elective replacement indicator; deactivated systems; lead parameters outside manufacturer recommendations, other implants present. ACLS, adult cardiac life support; BLS, basic life support; SAR, specific absorption rate.
This guidance aims to support the development of new providers of MRI services to patients with CIED (adults and children) and help the growth of existing services, in order to facilitate equitable provision for those patients in need wherever they may be in the UK. Guidance on MRI scanning of patients with CIEDs from other professional bodies have been considered in the production of these UK recommendations.1–8 This guidance is not intended to provide a comprehensive literature review, which can be found elsewhere.1 9
Background
Between 2016 and 2017, 3.7 million MRI scans were performed in England.10 MRI is one of the fastest growing imaging modalities with many diagnostic and treatment pathways increasingly dependent on MRI, including orthopaedics, neurosurgery and radiotherapy.10 Alongside this, implantation rates of CIEDs are rising—there are currently half a million people in the UK with cardiac permanent pacemakers or implantable cardioverter-defibrillators (ICDs) and over 40 000 new implants per year.11 These patients have historically been prevented from having MRI scans because of safety concerns, although half of this patient group are aged over 65 years and therefore have high clinical requirement for imaging due to comorbidities.12 Data suggest that 7%–17% of patients undergoing device implantation have MRI scans requested in the first 12 months post device implantation, highlighting the imperative to enable scanning where feasible.13 14 This demand for MRI in patients with CIEDs is growing rapidly at an estimated 10 000 scans a year based on annual growth in CIED implantations and MRI requests,10 11 15 highlighting the requirement for consensus recommendations for service delivery.
In response to this, industry has adapted the hardware and software in CIEDs to develop MR Conditional devices with regulatory approval for MRI scanning under strict conditions. Almost all CIED types are now available in MR Conditional models, and manufacturers report that currently almost all new CIED implants in the UK are MR Conditional. Provided all MR conditions are met including device reprogramming, these patients can safely undergo MR scanning. Alongside this, there is increasing clinical evidence that the risks associated with scanning a patient with a CIED that has not been formally tested and approved to undergo MRI, or where certain conditions of MR Conditional CIEDs are unmet, are lower than previously thought provided scans are performed under similar strict conditions to those required for MR Conditional CIEDs. Importantly, where there are no appropriate alternatives, MRI scanning is commonly justified and should be considered.
Barriers exist however at multiple levels from referrer to reporting radiologist—patients with CIEDs are approximately 50 times less likely to be referred for MRI than the general population, and workflows need to incorporate time and collaboration from multiple hospital departments with no established funding strategies that recognise service complexity.15–18 Progress has been made—a joint statement by the Clinical Imaging Board and British Cardiovascular Society demonstrates high-level consensus that new working practices are required.19 The 2018 British Heart Rhythm Society Standards for Implantation and Follow-up of Cardiac Rhythm Devices explicitly require CIED implantation centres to provide pacing support for MRI units.20 A recent survey of MRI departments in England showed that challenges to provision of MRI to patients with CIEDs persist—only 53% of units will scan patients with MR Conditional devices, and there remains an estimated 10-fold service underprovision.15 21
Clinical demand for MRI: a changing landscape
MRI has evolved as a powerful and versatile diagnostic imaging modality since its introduction into clinical use in the early 1980s. Technological advances have led to clinical application for diagnosis and treatment planning across all body areas and systems with profound impact on patient care. Consistent growth in referrals for MRI reflects the expanding clinical indications and incorporation into many guideline-recommended clinical diagnostic pathways.10 In the acute setting, timely provision of MR imaging is fundamental for diagnosis of a variety of conditions including acute ischaemic brain injury, spinal cord compression, spinal infection and trauma, while MRI is increasingly indicated in the oncology setting where it is first line for detection, characterisation and staging of many tumours including suspected clinically localised prostate cancer.22
Where MRI is unavailable, clinicians are generally forced to opt for alternate investigations that may be more invasive or have lower diagnostic accuracy, resulting in late or misdiagnosis with inherent clinical complications. Similarly, treatments that require pretherapy MRI planning such as neurosurgical procedures or MRI-guided stereotactic radiotherapy are unavailable to those patients where MRI is contraindicated, potentially impacting clinical outcomes.
Terminology
The following terms are defined by the international standard ASTM F2503-20, and are recognised and used globally by the MR community, medical device manufacturers and regulatory bodies.
MR Environment—the three-dimensional volume of space surrounding the MR magnet that contains both the Faraday shielded volume and the 0.50 mT field contour (5 G line). This volume is the area in which an item might pose a hazard from exposure to the electromagnetic fields produced by the MR equipment and accessories.
MR Safe—an item that poses no known hazards resulting from exposure to any MR Environment. MR Safe items are composed of materials that are electrically non-conductive, non-metallic and non-magnetic.
MR Conditional—an item with demonstrated safety in the MR Environment within defined conditions including conditions for the static magnetic field, the time-varying gradient magnetic fields and the radiofrequency (RF) fields.
No CIEDs are MR Safe, since they contain materials that are electrically conductive. However, the vast majority of CIEDs now implanted in the UK are now MR Conditional. This means that if all of the stated MR conditions are met, the manufacturer of the CIED is providing assurance that in terms of the MR safety issues related to that specific device, it is safe for the patient to undergo MRI.
MR Unsafe—an item which poses unacceptable risks to the patient, medical staff or other persons within the MR Environment.
The Medicines and Healthcare Productions Regulatory Agency (MHRA) guidelines for MR safety,23 the primary reference for MR safety guidance in the UK, additionally define the following term:
MR Unlabelled—an item without an MR Safe, MR Conditional or MR Unsafe label.
In the context of CIEDs, MR Unlabelled items have also been described as ‘conventional’, ‘legacy’, ‘MR non-conditional’ and ‘non-MR Conditional’.
Some MR Unlabelled items will clearly be unsafe in the MR Environment, for example, a ferromagnetic gas cylinder. Others will clearly be safe, for example, a saline bag. For many MR Unlabelled items, the MR safety risks will lie somewhere between these two extremes and may not be fully understood, particularly for implants. A key aspect of MR Unlabelled items is that no statement about MR safety is being made by the manufacturer of the item. Consequently, a local decision is required on whether to bring such items into the MR Environment based on a risk-benefit assessment.
Importantly, for MR Conditional items in scenarios where any of the MR conditions are unmet, again no statement about MR safety is being made. In such scenarios, these items should be managed in the same way as MR Unlabelled items, requiring a local decision to be made based on a risk-benefit assessment.23 Regarding CIEDs, the device system needs to be assessed in its entirety—as a whole—generator, lead(s) and any other system component in combination. Although individual components may be MR Conditional, manufacturers clearly stipulate the generator-lead combinations that have been tested and approved to be MR Conditional, and devices outside of these recommendations should be considered MR Unlabelled.
The MHRA safety guidelines defines the following terms that are used in this guidance23:
MR Responsible Person—someone who takes on the day-to-day responsibility for MR safety.
MR Safety Expert—someone who can adequately advise on the necessary engineering, scientific and administrative aspects of MR safety. Their knowledge of MR physics should enable them to advise on the risks associated with individual procedures and on methods to mitigate these risks.
For the purpose of this guidance, some of the tasks may be undertaken by persons other than the MR Safety Expert but who have the required scientific knowledge.
MR Operator—someone who is entitled to operate the MRI equipment. MR Operators are typically MR Radiographers, but may be assistant practitioners, radiologists, cardiologists or physicists.
For the purpose of this guidance, the term MR Radiographer will be used as it is recognised in the UK that Health and Care Professions Council (HCPC) registered radiographers perform the overwhelming majority of diagnostic MR scans. Where the MR Operator is not an HCPC registered radiographer services must ensure that clear governance processes are in place outlining roles, scope, supervision and responsibilities including responsibility for the safety of the patient during scanning.
Finally, the following term is defined in this guidance:
MR Clinician—any clinician responsible for reviewing appropriateness of referrals, protocolling and/or reporting the MRI scan of a patient with a CIED. For most sites these will be radiologists, but this may vary dependent on scan indication and setting, for example, a cardiologist for a cardiology-led MRI service or appropriately trained reporting radiographers. Departments scanning cardiac devices should ensure that more than one MR Clinician is trained and familiar with processes and procedures required for the safety and workflows of cardiac device MRI.
MR Conditional CIEDs
Historically, CIEDs were viewed as an absolute contraindication for MRI due to their perceived sensitivity to the strong static and time-varying magnetic fields produced by MRI scanners. These fields interact with medical devices in multiple ways, giving rise to various risks including mechanical forces (attraction, torque, vibration), heating, unintended stimulation and device malfunction. A number of technical developments have been incorporated into CIED design to mitigate these risks, including a reduction in the amount of ferromagnetic material, improved lead design and adapted software programming modes.24 In Europe, this resulted in the approval of MR Conditional pacemakers in 2008 and MR Conditional ICDs in 2014, with subsequent introductions into North America a few years later. Modern implantable cardiac monitors (including implantable loop recorders and implantable pulmonary artery pressure monitors) are MR Conditional, and this has been the case for the commonly implanted models for over a decade. Importantly, the conditions associated with MR Conditional cardiac monitors are relatively simple to meet without the need for the cardiology support that is required for MR Conditional pacemakers and ICDs, and many devices currently do not require data download prior to scanning.
Provided all the MR conditions are met, MR Conditional devices have been demonstrated to be safe for patients to undergo MR scanning and have regulatory approval as such. Various studies have demonstrated no clinically significant complications in patients with MR Conditional CIEDs randomised to MRI.25–28 Since their general introduction to our knowledge, there have been no adverse incidents associated with MR Conditional CIEDs undergoing MRI scanning when the MR conditions have been followed as per manufacturer recommendations.
Recommendations: standardised protocol for all MR Conditional CIEDs
Manufacturer conditions for patients with MR Conditional CIEDs to undergo scans include considerations at the time of device implantation, scan booking, on the day of the scan prior to MRI, during the scan and after completing the study (figure 2). These recommendations should be considered in addition to any MR conditions stated by the CIED manufacturer (routinely available on manufacturer websites). Services should consider how best to setup their systems to manage time points such that patient are triaged safely and effectively. In particular, attention should be paid to who is authorising, aware and facilitating these patients being booked.

Workflow for provision of MRI to patients with MR Conditional cardiac implantable electronic devices. ACLS, adult cardiac life support; BLS, basic life support; CIED, cardiac implantable electronic device; SAR, specific absorption rate.
Requirements at time of CIED implantation
All CIED implanting hospitals must adhere to British Heart Rhythm Society (BHRS) Standards for Device Implanting Centres to facilitate equitable provision of MRI to their patients.20 It is recommended that MR Conditional CIED systems (generator and leads in combination) are the default selection for all new implantations, unless there is strong reason to do otherwise, or there are other absolute contraindications to MR scanning. Similarly, at the time of upgrade or generator change, implanting cardiologists should ensure that lead and generator combinations maintained to be from the same manufacturer to ensure that conditions of the MR Conditional CIED can still be met. The basic implications of an MR Conditional CIED should be explained to the patient at the time of implantation, and there should be written confirmation on the device identification card stating whether the implanted CIED system is MR Conditional or not. This information should also be accessible in the medical notes of the patient. Each device has additional conditions that need to be fulfilled before a scan be performed (current device parameters acceptable, scanner and protocol conditions, etc), however these would be determined at the time of scan for patients with MR Conditional CIEDs.
For the rare scenarios where a fully MR Conditional CIED cannot be implanted (eg, where a patient’s cardiac anatomy necessitates a specific lead choice leading to manufacturer mismatch between the leads and generator, or the device must be implanted outside of the pectoral region), discussion with the patient regarding the risks and benefits should take place prior to device implantation and included in the formal consent process by the implanting cardiologist. Suggested consent statements are included in table 1. It should be explained to patients that having generator-lead manufacturer mismatch is no longer an absolute contraindication for MRI if there is sufficient clinical justification for the scan, although access to scans is likely to be more challenging as they are likely only be undertaken in centres that scan MR Unlabelled CIEDs. Transvenous CIED lead extraction has a procedure-related major complication rate reported of 0.19%–1.8%, including a mortality of 0.19%–1.2%.29 The risk of MRI scanning when appropriate protocols for MR Unlabelled CIEDs are adhered to appears to be very significantly lower than the risk of lead extraction, and so we would not recommend lead extraction solely to facilitate MRI.30–32
Suggested consent statement for implanting cardiologists when potentially implanting an MR Unlabelled device, or revising/upgrading a device that may then become MR Unlabelled (such as upgrading a pacemaker to a CRT using a lead from a different manufacturer to the existing leads and generator)
Each device centre must ensure that they have arrangements in place that allow patient access to MRI scanning. As per BHRS standards, CIED component details and MR Conditional labelling should be provided by the cardiology or device clinic to MRI departments on request to support the scanning process, and should be made available on easily accessible electronic healthcare record systems. For patients with MR Unlabelled CIEDs, arrangements may be required for MRI referrals to an external centre. Details of a registered referrals network can be found elsewhere (www.mrimypacemaker.com).33
Referral requirements and workflows
Identifying referrals
For all patients with CIEDs, the presence of a device must be flagged in the referral under all circumstances. All MRI units should have an established process in place to accept MRI referrals for patients with CIEDs, or have an established relationship with an external centre with a pathway for referral if there is no access to cardiology support locally. Clinically appropriate scan requests for patients with MR Conditional devices should not be declined without clear advice regarding how to access agreed referral pathways for alternative external sites, and MRI units within an institution that has CIED implantation services should not refer externally for MRI for MR Conditional devices. The referral process should be easily accessible to referring clinicians, although individual hospitals are likely to develop their own local protocols for accepting referrals. As many current electronic systems block requests if fields are checked for the presence of a CIED, a separate standardised booking proforma may be required. Work is currently in progress to update Royal College of Radiologists recommendations for electronic requesting systems (Order Communications) to facilitate MRI requests for patients with CIEDs, including fields for communicating the device details (including manufacturer and model) and MR Conditional labelling. An appropriate subspecialty MR radiologist should be available for discussion of the risk-benefit and potential for imaging using alternative modalities for referrals of patients with MR Unlabelled CIEDs. Staff availability should be checked prior to scan booking.
Device information to determine MR Conditional status
Device information should be provided to MRI units prior to booking the scan. This should include manufacturer, model and implantation date for generator and each of the leads. We recommend that the responsibility for obtaining the information lies principally with the referrer. MRI departments should not be obligated to accept referrals until they are satisfied that the data provided are sufficient to allow them to identify that the CIED is MR Conditional and to check the specific MR conditions for that device.
Ideally, device information should be recorded in the patient’s electronic patient record. However, many patients will have scans requested at hospital sites remote from where their device is followed up. In this situation, device information is best obtained from the patient’s usual CIED clinic, who should provide a copy of the implant report and/or the last device check. If this is not available, patients may provide a copy of their device identification card (issued at the time of implant), but the cardiology team will also need to ensure that all conditions are met at the time of interrogation prescan. All patients with CIEDs should be screened for the existence of abandoned leads or implantation of other metallic devices that may not result in MR conditions for the device being met. Where there is uncertainty related to the presence of additional hardware, a chest radiograph can be performed as part of screening, although this should not be required routinely.
An MR Conditional CIED must have both the leads and generators implanted by the same manufacturer in a combination that has been tested and verified to be safe within an MR Environment. An MR Conditional generator and MR Conditional leads from different manufacturers does not constitute an MR Conditional system. While the risk profile of such a combination may be comparable to a MR Conditional CIED,34 scanning should currently be performed as per protocols for MR Unlabelled CIEDs, see section MR Unlabelled CIED systems and MR Conditional CIEDs not fulfilling specified conditions. Device manufacturers offer verification tools which are centralised online (www.mrimypacemaker.com),33 and manufacturer representatives can also assist in the process. Verification of MR Conditional labelling should be performed by the most appropriate member of the team, but may be the cardiac physiologist, cardiologist, MR Radiographer, radiologist or MR Safety Expert. Ultimately, the MR Radiographer is responsible for the safety of the patient they are scanning and for ensuring all local procedures have been completed before the patient is brought into the MR Environment.
Prescan preparation
Consent
Patients with MR Conditional CIEDs do not require written consent prior to undergoing MRI when adhering to manufacturer conditions.
Device interrogation and programming
Standard MRI safety protocols should always be followed for all patients, with the additional steps outlined below for scanning MR Conditional CIEDs (apart from implantable cardiac monitors). A full CIED interrogation should be performed to identify any device problems or higher-risk features that have not been identified previously or may lead to MR conditions not being met. This device interrogation can then be used for baseline comparison in the event of device parameter abnormalities being detected post-MRI.
The CIED should then be programmed, ideally just before the MRI scan. CIED interrogation and programming should be performed by an appropriately trained cardiac physiologist (or cardiologist), and all prescan parameters should be documented to enable comparison for changes postscan.
The programming changes for MRI should adhere to manufacturer instructions by using an MRI mode. Within MRI mode, there are generally programming choices to enable patients both with and without stable underlying rhythm to be scanned safely. Typically, pacing should be programmed off with OVO or ODO modes if there is an adequate underlying rhythm; or asynchronous pacing with VOO or DOO modes if there is significant bradycardia or an unstable underlying rhythm.1 2 35 Decision-making regarding the CIED mode to be programmed for MRI will be led by the cardiac physiologist or cardiologist. If there is doubt about the risk of competitive rhythm, it may be necessary to observe the rhythm for a few minutes after programming and discuss the programming options with a cardiologist. For all ICDs, antitachycardia therapies will be disabled in all MR modes. If CIED programming occurs in a different department to the MRI scan, the patient may require monitoring during transfer depending on the risk of the programmed settings.
For some older implantable cardiac monitors, data should be downloaded prior to the MR scan as this may be corrupted following exposure to the strong magnetic fields. Where feasible, a record of the download should be made in the patient’s notes to alert radiography staff that this has been performed.
Scan protocol
The relevant MR healthcare professional should check that an appropriate comprehensive protocol is provided prescan both to minimise the risk of requiring repeat scanning and ensure that MRI scanning conditions are met. When scheduling and coordinating scans, all appropriate disciplines should be available at the time of the scan.
During scan
Monitoring during the scan
As with any patient, the risk of adverse events within the MRI scanner remains for the duration of the exam, and patients with CIEDs should be managed no differently. In the event of cardiac arrest or anaphylaxis due to contrast administration, the patient should be treated according to standard MRI department operating procedures. All staff must be familiar with evacuation protocols from an MR Environment.
Verbal communication with the patient is strongly recommended where possible. There is a low correlation of patient-reported symptoms and objective end points of lead parameter changes or MRI parameters associated with theoretically increased risk.35 Nevertheless, because the nature or timing of an event is unpredictable, communication for new symptoms or unresponsiveness may provide an early sign of deterioration.
Pulse waveform monitoring (plethysmography) is the recommended minimum method of monitoring heart rhythm, and is generally resistant to artefact from electromagnetic interference (EMI) during the scan. This can either be obtained via pulse plethysmography sensors built into MR scanners or via dedicated MR Conditional monitors. ECG or vector cardiography (VCG) monitoring is an important additional method that is recommended where feasible, and may be required to meet the requirements of some MR Conditional CIEDs. While some manufacturer guidance for MR Conditional CIEDs state only ECG monitoring is required, it may be difficult to monitor acute rhythm changes if there is artefact eon the ECG signal from the gradient fields. Blood pressure monitoring is not recommended as an alternative to ECG and pulse waveform monitoring. While this was performed in the MagnaSafe registry, cycling of a blood pressure cuff is likely to introduce delays to definitive assessment of an acute rhythm disturbance.
There should be a nominated physician responsible for the safety aspects available within the hospital at the time of scanning who is aware that a CIED MR is being performed. This may be a radiologist or cardiologist. There should also be both someone able to reprogramme the CIED and personnel who are adult cardiac life support (ACLS) trained available in the hospital at the time of the scan. For inpatient National Health Service facilities, the resuscitation team can generally provide the ACLS trained staff, but for other models of care specific arrangements will need to be made.
One staff member must be present who is able to monitor and detect a change in the patient’s rhythm from the available monitoring equipment. This could be a trained radiographer, trained nurse, cardiac physiologist or physician, provided they are capable of recognising significant changes in the heart rate/rhythm. The choice of staff member should be made locally, based on the knowledge and experience of the staff.
We recommend that staff with basic life support accreditation or above are present within the MRI unit for the duration of the scan. We recognise that other guidelines state a clinician with ACLS training is present with the patient from initial device programming to reprogramming after the MRI scan.1 These recommendations go beyond manufacturers’ guidelines, and some CIEDs permit auto-mode switching up to 48 hours prior to the MRI scan, and for up to 48 hours afterwards.36 Resources for CIED implantation or revision do not need to be available on the same site as the MRI facilities when scanning MR Conditional CIEDs.
Scan acquisition
At the time of writing, the most conservative conditions for MR Conditional CIEDs typically only require the MR Operator to ensure the MR scanner is in normal operating mode with regard to the specific absorption rate (SAR). There may be additional conditions including patient positioning, exclusion zones and field strength limits, although these can change as further manufacturer testing is performed. MR conditions often preclude the use of local transmit-receive coils directly over the CIED, such as a transmit-receive 31P-coil, but typically such coils are only used in research studies. The scan protocol should be decided prior to the patient arrival to include only the sequences required for a fully diagnostic examination. Metal artefact reduction strategies may be required to obtain diagnostic imaging, but are generally not required, especially for non-thoracic scans.37–39 To avoid patient recall and associated logistical issues, each radiology department should have a mechanism in place to check that the images acquired are diagnostic and sufficient for reporting, prior to scan completion.
Terminating a scan
In the event of a suspected arrhythmia, it is the responsibility of the attending MRI staff to evacuate the patient from the MR Environment as quickly as possible. Evacuation from the scanner is typically coordinated by the radiographer. One member of the team will administer basic life support while the cardiologist/cardiac physiologist interrogates the CIED or applies an external magnet to the generator. In the case of a bradycardia, the CIED can be programmed to pace asynchronously. In ventricular arrhythmias, the ICD can be programmed to deliver appropriate therapy. If there are any delays in CIED interrogation, ACLS protocol should be followed with the attendance of the cardiac arrest team.
Postscan
The CIED should be re-interrogated and programmed back to its original settings. If there is any significant change in a parameter, this should be communicated to the patient and ongoing follow-up should be arranged. It is left to the discretion of the cardiology team what constitutes a change that is not due to physiological fluctuation and measurement imprecision, and the timing of follow-up.35 40 All measurements should be documented.
It is also recognised that the beeper alarm function of CIEDs from several manufacturers may be permanently disabled after MRI (even in MR Conditional CIEDs), necessitating home monitoring or more frequent CIED follow-up particularly where devices are already under a manufacturer advisory. Cardiac physiologists should alert the patient and their usual device clinic if they feel that this loss of beeper function should lead to a change in routine follow-up protocols.
Table 2 summarises the key roles and responsibilities associated with individuals and departments regarding MR Conditional CIEDs. In some organisations, some of these responsibilities may be assigned to other individuals.
Summary of roles and responsibilities of each team member regarding MRI scanning of patients with MR Conditional CIEDs
Recommendations: infrastructure requirements
Personnel
Providing MRI for patients with CIEDs means that specialties need to work beyond traditional silos of practice. Staff involved in this service will include team members from the Departments of Radiology and Cardiology. Typically, this constitutes radiologists, MR radiographers, MR Safety Experts, cardiologists, cardiac physiologists. Other administrative and clerical staff also play a vital role, and their additional time and need for training must also be recognised. It may be useful to accelerate expertise and communication using named individuals, at least when establishing services. Institutions should have clearly defined protocols in place to ensure that these general recommendations account for the local environment and variations in service requirement. Local protocols must provide details regarding escalation procedures in the event of complications, with procedures for instituting basic and advanced life support where needed.
MR scanner
Up-to-date information regarding the MR conditions for scanning the CIED should be followed. MR conditions for MR Conditional CIEDs are relatively simple to meet on all current clinical MR systems. All devices allow for scanning within cylindrical bore 1.5 T systems and often 3 T scanning is accepted within the CIED manufacturer conditions. Other variations in MR scanner hardware/software (eg, maximum gradient amplitude) typically do not present a limitation for scanning patients with MR Conditional CIEDs. Advice from the MR Safety Experts can be sought if required.
Monitoring equipment
Patients must be monitored throughout the scans with a minimum of pulse oximetry waveform monitoring and/or ECG. The provision of MR Conditional monitoring equipment may require investment for units starting scanning patients with CIED, and sites procuring new MR Conditional monitoring equipment are encouraged to seek assurances that the equipment will provide robust data during MRI. Notably, most ECG monitoring systems— even many that are MR Conditional, are susceptible to significant signal artefact during some MR sequences. We therefore strongly recommend that continuous pulse oximetry waveform monitoring (which is generally resistant to artefact from gradient fields during image acquisition) is performed in all patients.
Although not approved for diagnostic purposes, MR scanners have their own monitoring systems with ECG and pulse oximetry waveform assessment for gating during image acquisition, and these may be sufficient for detecting changes in rhythm (rather than QRS/ST segment changes) needed for the purposes of monitoring patients with CIEDs. This approach has precedent given that it is currently routinely used during stress perfusion cardiac MRI, although this remains an off-label use of the scanner.
CIED programming units
All CIEDs except implantable cardiac monitors require programming before and after MRI. This requires the availability of a pacing system analyser (PSA), which is a portable unit that is able to interrogate and programme CIEDs. These are specific to the manufacturer and are available in all cardiac physiology departments or via manufacturers, but all are MR Unsafe. For patients with MR Conditional CIEDs, there should be a PSA available within the hospital at the time of scanning, however this does not need to be physically in the MRI department. Patients can be programmed within the cardiology or pacing department prior to arriving at the MRI unit.
Resuscitation equipment
A resuscitation trolley should be available within the MRI department. This should contain an external defibrillator. A manual defibrillator with the ability to transcutaneous pace may not be available in all MRI units, although is recommended when scanning patients with ICDs or those who are pacing dependent. For units scanning patients with MR Unlabelled devices, a manual external defibrillator with transcutaneous pacing capability must be available. Requirements should be discussed locally with the cardiology team. An external CIED magnet (available from CIED clinics) that can be applied to the CIED should also be available to enable reprogramming of the CIED to a default setting in an emergency situation.
Considerations and risks of device reprogramming in patients with MR Conditional CIEDs
For all patients with cardiac pacemakers, defibrillators or cardiac resynchronisation therapy devices, the CIED must be interrogated and reprogrammed into an ‘MRI mode’ prior to undergoing the scan in order to minimise the risk of complications from inappropriate pacemaker/defibrillator activation or inhibition of pacing. There are some additional considerations related to choice of CIED programming modes that should be adhered to in specific devices/patients.
Potential risks associated with changing CIED programming mode
Prior to scanning, it is important to ascertain the underlying heart rhythm and pacing requirement for patients with CIEDs in situ, even for patients with MR Conditional devices. Pacemaker-dependent patients have no underlying heart rhythm, or their intrinsic heart rate is sufficiently slow to cause symptoms and make the patient haemodynamically unstable, should pacing not be delivered.
Without appropriate device reprogramming, in pacemaker-dependent patients there is a risk that the device interprets EMI from the MRI scan as spontaneous myocardial activity (oversensing true cardiac electrical activity) and in response inhibits pacemaker function. To minimise this risk of oversensing, devices should therefore be programmed either to pace continuously (asynchronously) for patients with high pacing demand or those who are pacemaker dependent with no underlying rhythm, or alternatively with pacing programmed off for the duration of the scan where the patients’ underlying heart rhythm is stable.
For patients with an acceptable stable intrinsic heart rate and rhythm, there is a risk of arrhythmia either through unintentional pacemaker activation if the device is not reprogrammed into MRI mode, or with intentional programming to an asynchronous pacing mode that competes with the patient’s intrinsic rhythm. Pacing at the same time as intrinsic cardiac repolarisation risks ventricular arrhythmia (termed ‘R on T’), although asynchronous pacing is routinely performed during pacemaker lead threshold checks, with only extremely rare published cases of ventricular fibrillation precipitated by this (quoted risk <0.001%).41
Potential risks to patients with defibrillators
Defibrillator antitachycardia and shock therapies need to be programmed off for the duration of the MRI scan for all patients with ICDs and cardiac resynchronisation therapy-defibrillators (CRTDs). If defibrillator antitachycardia therapies are left activated for the MRI scan, this may result in inappropriate therapies or device malfunction. EMI is likely to be interpreted by the CIED as ventricular tachycardia leading to attempted delivery of therapy in the form of antitachycardia pacing or shocks. For this reason, all ICD therapies are automatically programmed off in all MR modes in all MR Conditional devices.
This does however mean that if a patient were to develop a ventricular arrhythmia while in the scanner, they would need to be evacuated and treated outside the MR Environment with external defibrillation or by reactivating the defibrillation therapies via reprogramming. ICD implantation is performed in patients at increased risk of ventricular arrhythmias—either for secondary prevention (in survivors of cardiac arrest or frequent ventricular arrhythmias) or primary prevention for patients with underlying cardiac conditions predisposing them to high risk of arrhythmias. For a 1 hour MRI scan in a patient with a standard primary prevention indication for ICD implantation, the risk of ventricular arrhythmia during an MRI scan is approximately ~0.0005%.42 43 Given this extremely low risk, patients with MR Conditional ICDs are treated as having a similar risk profile to patients with MR Conditional permanent pacemakers. If a recent clinically significant ventricular arrhythmia is detected prior to imaging, the cardiologist should be consulted to provide an opinion as to the risk of proceeding with the scan and programming the tachycardia therapies off.
Potential risks to patients with cardiac resynchronisation therapy pacemakers
Cardiac resynchronisation therapy-pacemakers provide biventricular pacing for patients with heart failure to maintain synchronous myocardial contraction, improve cardiac output and alleviate symptoms. Currently, ‘MRI-mode’ for most cardiac resynchronisation therapy-pacemakers permits only right ventricular (rather than biventricular) pacing, resulting in temporary loss of biventricular pacing. Although cardiac output will fall to a small extent while the device is programmed without biventricular pacing, the short duration of the scan means that the clinical risk of cardiac decompensation is negligible in haemodynamically stable patients undergoing MRI.
Potential risks to patients with implantable cardiac monitors
Implantable cardiac monitors include implantable loop recorders and pulmonary artery pressure monitors. There has been no reported harm to patients with implantable cardiac monitors undergoing MRI according to manufacturer stated conditions, and all modern devices are MR Conditional. For some implantable cardiac monitors, it is recommended that data are downloaded from the devices prior to undergoing MRI, but this is not needed for newer devices. Importantly, interrogation and reprogramming pre-MRI and monitoring during scans are not needed for patients with implantable cardiac monitors.
MR Unlabelled CIED systems and MR Conditional CIEDs not fulfilling specified conditions
Alongside CIED systems without MR safety labelling, there are many different scenarios where one or more of the specified conditions for an MR Conditional CIED are not met, each of which are associated with different levels of MR safety risk. Importantly, although the risks may be greater than when scanning patients with MR Conditional CIEDs where all the conditions are met, for many scenarios the lack of MR safety labelling reflect the limitations of testing, namely a lack of sufficient evidence to demonstrate that the device is safe under certain conditions, rather than any evidence demonstrating that it is unsafe. If the benefit to the patient outweighs these risks and there are no alternative modalities able to answer the clinical question, then the scan should be carried out, provided appropriate steps (as outlined below) are performed and documented. Risks should be mitigated where possible and the clinical decision should take into account the risks regarding onward clinical management if a decision is made not to perform the MRI (eg, both the risks of invasive biopsy and that of diagnostic uncertainty from incorrect or incomplete diagnosis).
For the many patients who find themselves in these scenarios, access to MRI currently can be particularly challenging.15 Given the availability of increasing safety data and the high clinical need for individual patients, some centres with good collaborative working between cardiology and radiology departments may wish to provide MRI scans for these patients. We aim to encourage a network of centres to cater for regional demand across the UK. This will permit centres to gain from efficiencies of scale, and centralisation of expertise.
The recommendations below are consistent with MHRA guidelines for scanning patients with implants where MRI may be contraindicated.23 figure 3 describes the suggested workflow when considering an MR request for a patient with an MR Unlabelled device or an MR Conditional CIED where one or more of the conditions cannot be met.

{kind=link}
{kind=link}
{kind=link}
Suggested additional steps required prior to performing MRI for patients with CIEDs that are MR Unlabelled or do not fulfil MR conditions. *Higher-risk scenarios include the presence of fractured, epicardial, abandoned leads; recent implantation; battery at ERI; deactivated systems; lead parameters outside manufacturer recommendations, other implants present. †Appropriate person confirming consent decided as per local protocol. ‡Consent can take place on the day of the scan, according to local protocols. For the purposes of this document, Present=present at scanner side. ACLS, adult cardiac life support; BLS, basic life support; CIED, cardiac implantable electronic device; ERI, elective replacement indicator.
Risk assessment and risk-benefit analysis
A risk assessment and risk-benefit analysis should be undertaken with involvement from a combination of the radiologist, cardiologist, referrer, MR Operator, MR Responsible Person and the MR Safety Expert.
The following points should be confirmed and documented prior to a decision to scan:
The MRI scan is likely to change patient management.
There is no appropriate alternative modality to answer the clinical question.
The potential benefit outweighs the risk of the MRI scan.
Risk-benefit analyses should incorporate individual patient, device and scan-related factors with specific scenarios as outlined below. The risks associated with a particular scenario can vary significantly depending on the individual circumstances, and consensus opinion is provided where clinical evidence is limited.
Metallic artefact from the CIED generator can provide additional challenges for anatomical regions that lie close to the device. This is a particular problem for cardiac MRI studies, however diagnostic imaging is generally feasible with published strategies.39 44 Artefact is generally more frequently encountered with ICD and CRTD devices, and MR Conditional labelling does not attenuate this problem or guarantee diagnostic image quality. Similarly artefact tends to increase at higher field strengths, hence imaging at 1.5 T rather than 3 T is recommended where available. For most MRI scans, artefact should not be a major factor in decision-making.
Risks associated with MRI in specific scenarios
A summary of the risks associated with the scenarios discussed below is provided in table 3.
Risk stratification of performing MRI in patients with MR Unlabelled CIEDs or MR Conditional CIEDs outside specified conditions
MR Unlabelled CIEDs
The risks associated with any MR Unlabelled active implantable medical devices include mechanical forces (attraction, torque, vibration), heating, unintended stimulation and device malfunction. CIED generators also may contain components sensitive to the magnetic field including reed switches, which may change position in an MR field leading to alterations in programming mode. Software corruption can occur due to electromechanical interference (EMI) known as ‘power-on reset’, causing the CIED to revert to a back-up mode of programming. Before the introduction of MR Conditional CIEDs, developments associated with CIED design had already gone some way to reducing these risks. Even for pacemakers with market release before 2002, the attractive force and torque experienced due to the magnetic fields associated with a 1.5 T MRI scanner were shown to be lower than the confining forces of surrounding tissue and hence low enough to present no safety risk.45 Technical developments associated with CIED generators generally (particularly ICDs) mean those implanted after approximately the year 2000 have reduced risk of heating, malfunction and electrical reset during MRI both in testing and from clinical data.45 Implantation dates before 2000 and 2002 were used as exclusion criteria for the two largest studies of MR scanning of patients with MR Unlabelled CIEDs.35 46
There is a significant and growing body of clinical evidence to support MR scanning of patients with MR Unlabelled CIEDs under strictly controlled conditions, similar to MR Conditional CIEDs. Three recent registries totalling 2859 patients with MR Unlabelled CIEDs undergoing MRI have reported no deaths or life-threatening arrhythmia.35 47–49 Patients were however excluded if they were pacing-dependent and had an ICD without asynchronous pacing capability. Fifteen of 2859 patients with CIED underwent partial or complete software resets (‘power-on resets’), many of which were transient or could be programmed around. One patient required a generator change as the patient did not undergo CIED reprogramming prior to an MRI scan.50 A recent meta-analysis of 5625 patients undergoing 7196 MRI scans similarly reported no deaths and no lead complications. There were 1.4% of cases with power-on resets, but none in devices that were released to market after 2005.51 Another meta-analysis of 5099 patients (overlapping with these studies) included one report of inappropriate ICD shock delivery (n=1).49
Although the number of patients included in published data is relatively large, it should be noted that the number of cases with a particular combination of generator and leads may be very small. To satisfy regulatory bodies that a particular combination can be labelled as MR Conditional typically involves modelling millions of such potential exposure conditions.52 53
These data highlight the low risk of MRI scanning, provided that strict protocols are followed, although quantifying personalised absolute risk is complex because of individual differences in pacing and device component factors. In summary, there is a significant body of clinical evidence to support MR scanning of patients with MR Unlabelled CIEDs implanted after 2002 under strictly controlled protocols similar to MR Conditional CIEDs, when clinically indicated. Patients with MR Unlabelled CIED generators with market release prior to this time appear to have a slightly greater risk from MRI including around 1.5% risk of electrical reset alongside other unpredictable complications,54 and therefore this should be considered in the risk-benefit assessment prior to scanning—particularly for patients with high pacing requirements. MRI is not recommended for patients who are pacing dependent and have an ICD without asynchronous pacing capability.
MR Conditional CIEDs with ‘mismatched’ CIED components
CIED generators and leads are manufactured and sold as separate components, meaning that implantation of a fully MR Conditional system requires operator selection of appropriate individual components. ‘Mismatched’ CIED systems are those with either only some components which are MR Conditional, or with fully MR Conditional components but produced by different manufacturers, and so will not have been formally tested in combination.
Manufacturers have performed formal MR safety testing of older leads that were previously MR Unlabelled, and have frequently shown them to be sufficiently safe when combined with MR Conditional generators from the same manufacturer to satisfy retrospectively relabelling the leads as MR Conditional. Comprehensive formal testing of every possible generator-lead combination (especially between different manufacturer components) is neither feasible nor appropriate meaning that this issue is unlikely to be eliminated.55
Patients with MR Unlabelled generators and leads are likely to require generator exchange before the battery reaches end of life (EOL) (5–10 years for the majority of CIEDs), and currently the majority will have a new MR Conditional generator implanted and connected to the original MR Unlabelled leads. Recent multicentre data have found no increased incidence of adverse effects of MRI with MR Unlabelled leads as compared with MR Conditional leads—both in terms of safety events and changes to lead parameters.34 These data (in combination with that from other studies with MR Unlabelled devices) suggest that the clinical risk of MRI in patients with MR Conditional generators is not increased by having MR Unlabelled leads connected. To facilitate equitable access to MRI, many centres currently scanning only MR Conditional CIEDs may choose to regard MR scanning for ‘mismatched’ devices with MR Conditional generators as a lower risk scenario so standard protocols for MR Conditional CIED systems are used, provided that there are no other high-risk features.
MR Unlabelled pin plugs
There are clinical scenarios when a patient does not require implantation of all of the leads that can be accomodated by a particular generator. In these situations, a pin plug is inserted into the generator to fill the port at the time of implantation. This serves the purpose of blanking off the port to ensure biological tissue does not enter and should not affect the electrical configuration of the device. Plug attachment types follow an industry standard and hence this compatibility between manufacturers can lead to implanted systems with a mismatched port plug. To form a complete MR Conditional pacing system, specific pin plug models have been tested by manufacturers in combination with other components. Consequently, use of pin plugs from a different manufacturer may invalidate an MR condition of the MR Conditional generator. However, these are considered a very low-risk scenario with no reported adverse effects, provided there are no other high-risk features.
Non-standard lead implants and additional leads
CIED leads are generally implanted permanently via venous access to the heart. However, leads can also be implanted with the intention of remaining temporarily, or may be implanted by differing access including surgically implanted leads that are attached to the epicardium of the heart. CIED leads can also malfunction, fracture or dislodge over the many years that they are implanted. To ensure ongoing device function and given the risks of lead extraction, additional leads may be implanted and the non-functioning lead removed from the generator but left in situ. A functional or non-functional lead that is left in place and is not connected to a CIED is termed an abandoned lead.29 If there is any doubt regarding the implanted hardware and associated risks, patients should undergo chest X-ray and there should be further discussion with a cardiologist with appropriate experience of CIEDs and MRI. The risks associated with MR scanning of patients with abandoned or fractured leads include the potential for induced voltages in the leads from the RF field (strongest in amplitude within the transmit RF coil) or the imaging gradients (strongest in amplitude around 30 cm away from magnet isocentre), causing lead heating (most likely at the lead tip) and/or direct stimulation of the cardiac muscle. One method to mitigate the risk from the RF field is through the use of transmit receive (T/R) coils. These ensure the majority of the RF energy is only imparted to a specific anatomical region within or covered by the coil and therefore, if positioned appropriately, can minimise the RF exposure to the CIED.
Abandoned or fractured transvenous permanent pacemaker or defibrillator leads
Experimental evidence to help quantify the risks of abandoned or fractured transvenous permanent pacemaker and defibrillator leads is mixed with some studies suggesting large temperature increases both in vitro56 57 and in vivo animal studies.58 More recently, in vitro testing at 1.5 T has demonstrated greater MRI-induced heating in abandoned leads (up to 29.9°C) compared with pacemaker-connected leads (up to 11.6°C),59 60 although temperature rises were strongly dependent on lead length and were generally higher when the abandoned leads were capped. A recent study performing electromagnetic simulations of numerical models with fractions of retained endovascular leads positioned at different imaging landmarks found temperature rises during a 10 min scan at all imaging landmarks remained <3°C at 1.5 T and <6°C at 3 T.61 Another numerical study at 1.5 T found the deposited power at the lead tip for fractured leads (increased up to a 16 times compared with non-fractured leads) was dependent on type of conductor break, and the design and location of the lead.62 Importantly, in vitro measurements demonstrating temperature rises up to 7°C around the lead tip were found to be insignificant when repeated in vivo, where there is a significant cooling effect from adjacent blood flow.45 Additionally, any localised RF heating is expected to be significantly less when the device/leads are located outside of the transmit RF coil.
Despite these experimental data, clinical reports have not described clinical or electrical evidence of CIED dysfunction, arrhythmia or pain as a result of MRI in patients with abandoned leads. Clinical studies have reported outcomes on patients with either abandoned leads alone, or in the presence of an additional functioning CIED, and so both scenarios are included in this recommendation. Currently, the largest clinical dataset available included 200 scans in 139 patients with CIEDs and abandoned leads, with no clinical complications, similar to other case series.63–65 Given the mixed evidence from simulations and preclinical work together with the relatively small clinical evidence of scanning patients with abandoned leads, this scenario is considered intermediate risk.
Permanent epicardial pacing leads
To our knowledge, currently no permanent (surgically implanted) epicardial pacing leads are labelled MR Conditional, due to the risk of RF heating at the lead tips, which has been demonstrated ex vivo.49 59 60 63 64 For these reasons, patients with surgically implanted permanent epicardial leads were excluded from large registries performing MRI scanning of patients with MR Unlabelled CIEDs. However, to our knowledge no clinical adverse events have been reported from scanning CIEDs with the presence of epicardial leads, and many units currently scan such devices using the additional precautions recommended for patients with MR Unlabelled devices.59 64 All patients with permanent epicardial pacing leads should be considered as a high-risk MRI scenario even if other components are MR Conditional.
Postoperative epicardial pacing wires
Temporary epicardial wires placed at the time of cardiac surgery are different to surgically implanted epicardial leads as part of a permanent CIED system. Where possible, temporary epicardial wires will be removed postoperatively. Alternatively, these may be cut at the skin after surgery leaving a short length of wire implanted chronically. A study including 51 patients who underwent MRI at 1.0 or 1.5 T with temporary epicardial pacing wires cut short at the skin found no reports of clinical events or symptoms suggesting arrhythmia or other cardiac dysfunction.66–69 Patients with postoperative epicardial pacing wires are fairly common, and given the low risk of complications, this should not be considered a contraindication to MRI scanning.
Temporary CIED system with externalised generator (‘temporary-permanent CIED’)
These are systems that are implanted temporarily (generally while patients are treated for systemic infection or where recovery of intrinsic electrical conduction is expected) and consist of a generator fixed to the external chest wall with a transvenous (usually active fixation) lead attached and implanted internally. There are few reports of such devices undergoing MRI,70 71 and although clinical complications have not been reported, these should be considered for a high risk MRI, and this should only be performed when MRI is considered essential to the patient’s clinical pathway.
Recent device implantation (within minimum duration specified by MR conditions)
Most MR Conditional CIEDs include the condition that scanning be performed a minimum of 6 weeks following implantation. This is often described as a period to allow fibrosis at the lead-myocardial interface. However, the theoretical risk of lead displacement is minimal given the lack of ferromagnetic components within MR Conditional leads, and hence negligible force on the lead tip.1 Clinical scans performed within 6 weeks have not been associated with complications,72 and similarly, no correlation between changes in lead performance (sensing, pacing threshold or impedance) and time from implantation was observed in cases from the MagnaSafe registry that included 17 cases in which MRI was performed within 30 days of implant, and 5 cases in which MRI was performed within 7 days of implantation.35 Some manufacturers now provide flexibility in their MR conditions for scanning during this period if clinically necessary. It is therefore appropriate to perform an MR scan earlier than recommended if the scan indication is required, but patient positioning should avoid arm elevation above shoulder level for the first week postimplant as per standard postimplant care to reduce the risk of traction on the lead resulting in displacement.
MR Conditional lead parameters that do not meet specified conditions
Manufacturers of MR Conditional pacemakers and ICDs generally stipulate device parameter conditions that must be fulfilled prior to patients undergoing MRI, such as measured lead threshold and impedance values. For CIEDs with parameters outside of these values, the cause of any abnormal lead parameter should be investigated before MRI scanning by the cardiac physiologist and cardiologist. If there is evidence of lead fracture, this should be considered a high-risk MR scan. For patients with high lead thresholds or low sensing, if these abnormalities are stable and a sufficiently increased safety amplitude window can be programmed (at least twice threshold), systems should be treated as MR Unlabelled CIEDs and patients consented for relatively higher risk of complications.
MR Conditional CIED generators with batteries close to depletion (elective replacement indicator or end of life)
Lead outputs are significantly increased as default with MRI modes (generally to 5.0 V at 1.0 ms), and a drop in battery voltage has been observed for some MR Unlabelled CIEDs undergoing MRI. Together this means that manufacturers of MR Conditional devices stipulate a minimum battery voltage that generators should have prior to scanning in order to fulfil conditions.73 Excessive battery depletion during MRI of devices with prescan low voltages (elective replacement indicator (ERI) or EOL) may risk CIED malfunction or automatic pacing mode switch if the device reaches EOL. More recently, a review of 9 non-pacing-dependent patients with MR Unlabelled CIEDs who underwent 13 MRI within 3 months of the ERI reported electrical reset in 2 patients, although both occurred in pacemakers implanted pre-2005.74 Generator change may be performed prior to MRI, where there is concern about the risks of mode switch or further battery depletion are high. Patients with batteries close to depletion should be considered to be at a higher risk of complications from MRI.
Inactive, battery-depleted generators
CIEDs may remain implanted with a depleted battery in patients without pacing requirements, where the clinical need for generator exchange is low. Although non-functioning, these devices are generally older and may therefore potentially still be at risk from MRI due to mechanical forces, heating, unintended stimulation. One case has been reported of tachycardia and chest pain on scan initiation within one large retrospective cohort (n=1148 MRI examinations).34 Patients with inactive, depleted generators should therefore be considered as an intermediate risk for MRI.
MR Conditional generators implanted outside of the pectoral region
CIEDs are generally implanted in the pectoral region but may (rarely) be implanted in other locations, including the abdomen. MR conditions generally stipulate that the generator should be implanted in the pectoral region, and the risks of MRI in patients with CIEDs in other anatomical locations are unlikely to have been tested by manufacturers. This means that such CIEDs, even if MR Conditional, should be considered as equivalent to MR Unlabelled devices, although the absolute clinical risk is not known. Given that patients may have abandoned hardware from previous implants in other locations, there may be other factors that increase the risk of MRI (eg, epicardial leads with an abdominal implant). Additionally, it is important to note any MRI exclusion zones will have been defined based on the specified device location.
Unmet condition for additional implanted devices
It is not possible for the manufacturer of an MR Conditional CIED to assess the potential interactions with all additional implanted devices. However, it is important to recognise that the risk of potential interactions between devices drops off significantly with separation distance, for example, ISO/TS 10974 only suggests an assessment for potential proximity enhancement from coupling between multiple electrodes is required when the separation distance is <2 cm. Although some MR Conditional CIEDs exclude the presence of any additional devices, others do not which suggests the risks associated with this scenario, particularly when the additional devices are well separated from the CIED, are low.
Scanner-related scenarios
Unmet condition for MRI field strength or MRI scanner type
The vast majority of clinical MRI scanners are closed bore cylindrical MRI systems operating at 1.5 T or 3 T. Although some MR Conditional CIEDs are labelled as MR Conditional at 1.5 T only, many now permit scanning at both 1.5 T and 3 T, although to our knowledge all are specified only for closed bore cylindrical MRI systems. There is little evidence available for MRI scanning of patients with CIEDs at other field strengths or on other MRI scanner types, for example, open MRI systems. Importantly, it is unlikely that the different RF frequencies associated with other field strengths will have been assessed by the CIED manufacturer and therefore this scenario presents an unknown risk in terms of RF heating, device malfunction and unintended cardiac stimulation. For sites unable to meet the conditions of an MR Conditional CIED for MRI field strength and MRI scanner geometry, onward referral to a centre that can meet this condition is likely to be the most practical solution, although centres scanning MR Unlabelled CIEDs may choose to scan locally with the additional steps recommended for scanning patients with MR Unlabelled devices.
Unmet condition for specific absorption rate (SAR)
Many MR Conditional CIEDs require the MRI scanner to be restricted to the normal operating mode for SAR (whole body SAR limited to 2 W/kg). In general, this is achievable for many clinical MR sequences without significantly impacting image quality, but there may be occasions where there is a clinical need to operate in the first level controlled operating mode for SAR (whole body SAR limited to 4 W/kg). There is growing evidence to support safe MRI scanning of patients with CIEDs at these SAR levels. A study of 1464 patients with non-MR Conditional CIEDs who underwent 2028 MRI examinations without SAR restrictions found no evidence of an association between RF energy deposition, dB/dt, or scan duration and changes in device parameters.75 76 Consequently, for scenarios where there is a clinical need to operate with SAR levels above the normal mode, the incremental risk appears to be relatively low.
Unmet patient positioning exclusion zone condition or with thoracic isocentre
Some MR Conditional CIEDs include an exclusion zone, to avoid positioning the device such that it is exposed to the highest levels of RF during the MRI scan. This may reflect conservative conditions that were incorporated into some clinical trials supporting regulatory approval of MR Conditional CIEDs, rather than confirmed evidence of risk. Indeed, many MR Conditional CIEDs no longer include this condition, suggesting the associated risks are low.
Unmet patient decubitus condition
Some MR Conditional CIEDs provide limited conditions for the patient decubitus during the MRI scan, for example, supine or prone. This is likely to reflect the limitations of MR safety testing and the simulations performed. To our knowledge, there have been no increased risks identified with different patient positioning and given several manufacturers of MR Conditional CIEDs do not state any such MR Conditional, the expected risk is low.
Recommendations: additional protocol for MR Unlabelled CIEDs or MR Conditional CIEDs outside the specified conditions
Prescan preparation
Referral
Patient and device factors that identify patients to be at higher risk for undergoing MR scanning should be identified before booking a scan (table 3). In addition to the particular risks posed in the MR Environment by CIEDs, it is important to note that CIEDs should be viewed as only part of the whole. Other MR contraindications are just as commonplace with patients with CIEDs as the general population, therefore a full MR safety questionnaire should always be completed prior to entering the scan room.
Consent
Informed written patient consent should be obtained and documented. However, local sites may decide that written consent is not necessary for lower risk scenarios as listed in table 3. The process should include discussion of the potential risks of scanning based on the specific CIED characteristics, and the benefits of the scan. Information therefore must be available for the person taking consent (who may be the radiologist or cardiologist dependent on local protocols) regarding the patient, device, clinical necessity and feasible alternatives to MR scanning. Ideally, information about the risks should be provided to the patient in advance of the MRI via a written patient information leaflet. Suggested phrases for consent in more common scenarios are provided in table 4. Other scenarios, not included in table 4 and which depend on the CIED, patient and MRI characteristics can be viewed as a spectrum from lower to higher risk relative to these data (table 3).
Suggested statements to use when describing risk during consent for patients with different non-MR Conditional CIEDs
Device interrogation and programming
CIED programming changes need to be performed manually for MR Unlabelled generators, including disabling all advanced features and all tachycardia therapies and shocks for defibrillators. This requires careful, individualised programming strategies that incorporate patient and CIED factors. For MR Unlabelled CIED programming, a monitor mode (OVO or ODO) should be used if there is an adequate underlying rhythm; or VOO, DOO if there is presence of bradycardia (<40 bpm).1 2 35 It is important that the initial programmed CIED settings are recorded prior to programming for the MRI scan, in order to ensure appropriate settings are restored post-MRI and in the event of software reset.
During scan
There should be at least one healthcare professional available within the MRI department for the duration of the scan who has basic life support training. Additionally, there should be personnel able to reprogramme the CIED if required in the department. In practice, this may be the same healthcare professional (commonly the cardiac physiologist or cardiologist). Personnel who are ACLS trained should be available in the hospital at the time of the scan.
Patients should be monitored verbally and with both continuous ECG and pulse oximetry monitoring for the duration they are in the MR Environment. When planning the MRI protocol, scans should be abbreviated and steps taken to reduce risk where feasible (eg, reduced SAR, choice of field strength), guided by the MR Safety Experts. In order to minimise the risk of needing to recall patients (and hence expose them to potential additional clinical risk), there should be a mechanism in place to check completeness of the image acquisition in real-time prior to scan completion and removing the patient from the scanner.
Postscan
MR Unlabelled CIEDs should be interrogated and programmed back to pre-MRI initial settings. This is a more manual process than MR Conditional CIEDs and therefore requires careful checking of each parameter. If there is any significant change in a parameter, this should be communicated to the patient and ongoing follow-up should be arranged. Suggested lead parameters classified as significant are: a decrease in sensed P wave amplitude ≥50%; a decrease in sensed R wave amplitude ≥25%; an increase in capture threshold ≥0.5 V; an absolute change in pacing lead impedance ≥50 Ω; an absolute change in high-voltage lead impedance ≥3 Ω; a decrease in battery voltage ≥0.04 V. This is based on a small test-retest substudy of the MagnaSafe registry (n=30). In this study, there were no P wave amplitude decreases ≥1.0 V, no R wave amplitude decreases ≥2.0 V and no pacing threshold increases of ≥0.5 mV—suggesting these sensitivity thresholds are real. Pacing lead impedance changes ≥50 Ω were noted in 3.6% of leads; and shock impedance changes ≥3 Ω were observed in 17.6% of defibrillator leads.35 40
Other considerations
Emergency scanning of CIEDs
There are several medical conditions where emergency out of hours scanning may be requested for diagnosis and treatment planning (for example suspected spinal cord compression). However if such emergency scans are required in patients with active (functional, non-battery depleted) CIEDs, the same protocols must be followed as per elective scanning. There are no clinical circumstances where MRI without reprogramming of active CIEDs and adequate supervision can be recommended. Alternative imaging modalities should be explored, and for most conditions, treatment can be initiated empirically. There is recognition of need for prompt emergency MRI in some scenarios and the aim should be for provision of scans (at least regionally within a network) as soon as possible, although the standard pathways for device reprogramming and monitoring as detailed above should be followed.
Reporting suspected safety events
Previous work has highlighted an under-reporting safety events.50 Any possible safety events related to the CIED should be reported to the Medicines and Healthcare products Regulatory Agency using the Yellow Card system with addition data collection for audit of local practice.77
Information for patients
Patients with MR Conditional devices have the right to expect access to MRI services locally where the clinical indication is reasonable. For patients with MR Unlabelled devices or MR Conditional devices where the conditions cannot be met, patients should encourage clinicians to collaborate with specialist centres to ensure access to MRI if there is clear potential benefit to mitigate the potential risk. Patients (and/or their carers) have a duty to make their referring clinician and the MRI department aware that they have a cardiac implantable electronic device to facilitate safe planning of the MRI scan. Because of the complexity of the service, this usually requires coordination of different medical teams and may introduce some delays, but this should account for the clinical urgency of the scan. Where local services are not available (particularly for patients with MR Unlabelled devices), further information on specialist regional centres can be found at www.mrimypacemaker.com. Charitable and patient bodies including the Arrhythmia Alliance (www.heartrhythmalliance.org) and Cardiomyopathy UK (www.cardiomyopathy.org) can provide support and guidance.
Areas for further research
Significant progress has been made in recent years to develop strict protocols for patients with CIEDs undergoing MRI. There are still significant logistical burdens associated with performing MRI for this patient group, and development of protocols and tools to alleviate these burdens are needed. There is a growing appreciation of a spectrum of risk associated with MRI for patients with MR Unlabelled CIEDs or MR Conditional CIEDs with unfulfilled MR conditions. A growing body of experience will help to inform clinical decision-making in individual scenarios. It is likely some scenarios will be regarded as having similar risk profiles to fully MR Conditional CIEDs, while other scenarios will have higher-risk profiles. Given that patients with MR Unlabelled CIEDs or MR Conditional CIEDs with unfulfilled MR conditions will require urgent diagnoses reliant on MRI for many decades, service provision should be developed to reduce the health inequality in MRI access. This will require appropriate design of infrastructure and health economic data to inform policy. Patients with CIEDs are typically not included in research trials which incorporate MRI, even if the CIED is MR Conditional. This compounds the health inequality that patients experience. MRI protocols should be developed for clinical trials and ethics submissions should reflect the changing practice for patients with CIEDs, particularly in the context of cancer or neurological disease.
Conclusion
These multisocietal Consensus Recommendations outline guidance for safe delivery of MRI to patients with CIEDs, and aim to improve provision to address current inequities of service delivery. The majority of patients with CIEDs should now be able to undergo MRI, although it is anticipated that patients with MR Unlabelled devices or MR Conditional devices where it is not possible to meet all the specified conditions a local risk-benefit decision is needed. Collaborative interdisciplinary working is required to facilitate safe workflows and these guidelines incorporate recommendations from all stakeholders, including patients, to drive widespread adoption and encourage service expansion.
Supplemental material
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @mrimypacemaker, @#tcasl
Contributors AB drafted the work. CM chaired the Working Group. All authors were involved in the Working Group, reviewed the work critically, distributed and collated feedback from their respective professional societies. Each professional society reviewed the manuscript and approved the final version. All authors gave final approval of the version to be published.
Funding This study was funded by British Heart Foundation (HFHF_016).
Competing interests AB and CM are recipients of a British Heart Foundation Grant (BHF HfHF_016) to make MRI available for patients with pacemakers. All other authors have no conflict of interest.
Provenance and peer review Commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.