Article Text

Statistics from Altmetric.com
Learning objectives
To understand the definition and simplified pathophysiology of HFpEF.
To understand the appropriate diagnostic work-up for those patients with suspected HFpEF.
To understand contemporary pharmacological and non-pharmacological therapies for HFpEF.
This paper covers part of the ESC Core Curriculum for the General Cardiologist (2013)41 :
2.17 Heart Failure Objectives:
To recognise the impact of heart failure on morbidity and mortality in the individual patient and in the population at large
To recognise heart failure and the different underlying causes
To perform specialist assessment and treatment of patients with heart failure
To work with patients and their families’ primary care physicians, sub-specialists, nurses, and other healthcare professionals
To organise structured follow-up of patients after diagnosis
Introduction
Heart failure (HF) is a clinical syndrome with typical symptoms of breathlessness, fatigue, reduced exercise tolerance, body swelling and signs of fluid retention such as increased jugular venous pressure (JVP), pulmonary congestion and peripheral oedema. They are the consequences of impaired myocardial function, causing inability to maintain cardiac output in response to metabolic demand. HF affects 1%–3% of people worldwide.1 HF prevalence in the USA is estimated at 2.5% with 6 million patients having a confirmed HF diagnosis.2 According to a study of 4 million people in general practice in UK, 1.6% of population have HF.3 There is, however, a cohort of patients who are undiagnosed and the true prevalence of HF is likely higher.4 It is estimated that 50% of patients with HF have heart failure with preserved ejection fraction (HFpEF).5 HFpEF is associated with multimorbidity, with as many as 50% of patients having five or more significant comorbidities.The hallmark of HFpEF is the presence of increased left ventricular (LV) stiffness with impaired relaxation. This pathology develops with older age; hence, the prevalence of HFpEF is projected to increase as a consequence of the ageing population.6 The European Society of Cardiology (ESC) estimates the prevalence of HFpEF in the population aged >60 years at 4.9%.7 People with HFpEF have a higher prevalence of hypertension, diabetes mellitus (DM), chronic kidney disease (CKD), atrial fibrillation (AF) and non-cardiovascular (CV) comorbidities (such as obesity and chronic obstructive pulmonary disease (COPD)) than those with heart failure with reduced ejection fraction (HFrEF). Women with HFpEF significantly outnumber men, leading to a gender ratio of approximately 2:1, supporting the notion that gender plays a crucial role in this condition.8
Regardless of the type, HF is associated with very high 5-year mortality reaching 50%–75%.1 Outcomes in HFpEF are comparable with those in heart failure with reduced ejection fraction; therefore, intervention should be implemented early to prevent mortality, morbidity and poor patient-reported outcomes. Mortality due to non-CV causes is increased in those with HFpEF.1 Although HFpEF is thought to have better survival than HFrEF based on findings from clinical trial data,9 most observational studies show that this difference is ’negligible’.4 There is no difference between HFpEF and HFrEF in terms of hospitalisation rate, hospitalisation duration and impact on quality of life (QoL).9 The rate of hospital admissions is high, with an average one admission per year from initial HF diagnosis. Management of comorbidities and diuretic therapy have long been central in the treatment of HFpEF, with the aim of reducing symptom burden and preventing hospitalisation. However, breakthrough RCT data on sodium–glucose cotransporter-2 inhibitors use in HFpEF (EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Preserved Ejection Fraction (EMPEROR-Preserved), Dapagliflozin in PRESERVED Ejection Fraction Heart Failure (PRESERVED-HF) and Dapagliflozin Evaluation to Improve the LIVEs of Patients With PReserved Ejection Fraction Heart Failure (DELIVER)) show improved patient-reported outcomes and reduced heart failure hospitalisations (class 2a recommendation 2022 American College of Cardiology HF guidelines).
In view of these data, HFpEF is recognised as a growing epidemiological issue7 due to high mortality, increasing costs from high hospital admission rates, poor patient reported outcomes impacting QoL and years lost in employment. As such, it is important for clinicians to have a good understanding on how to diagnose and treat HFpEF.
Definition
Contemporary definitions of HF distinguish HF types based on differences in the left ventricular ejection fraction (LVEF).4 10 Current international guidelines (ESC and American Heart Association (AHA)) divide HF into HFrEF with LVEF of <40%, heart failure with mildly reduced ejection fraction (HFmrEF) with LVEF between 41% and 49%, and HFpEF with LVEF of >50%.4 10 11 Figure 1 presents internationally accepted definition and diagnostic criteria distinguishing types of HF.4 10 11 Per this definition, HFpEF is a clinical syndrome consisting of symptoms and signs of HF, with evidence of structural and/or functional cardiac abnormalities and/or raised natriuretic peptides (NPs), and with an LVEF of ≥to 50%.4 What is worth noting though is that NP may not be raised in about 20% of patients presenting with true HFpEF. In the Diagnostic process section, we provide further explanation of the underlying causes of normal NP in patients with HFpEF.

Types of HF according to differences of LVEF based on internationally accepted universal definition of HF.4 10 11 HF, heart failure; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; LV, left ventricular; LVEF, left ventricular ejection fraction.
Prior to use of the term HFpEF, ’diastolic dysfunction’ term was used to describe this complex clinical syndrome; however, its use has been discouraged since it became clear that diastolic dysfunction is not unique to HFpEF, but it coexists in HFrEF and HFmrEF too.9 Originally, HFpEF was viewed as a disorder due solely to abnormalities in LV diastolic function; however, the understanding has evolved such that HFpEF is now understood as a systemic syndrome, involving multiple organ systems, likely triggered by inflammation and with an important contribution of ageing, lifestyle factors, genetic predisposition and multiple comorbidities.12
Pathophysiology
The pathophysiology of HFpEF is complex, and systemic changes related to comorbid conditions drive myocardial dysfunction. Various mechanisms have been suggested as causing the pathophysiology of HFpEF, either individually or in combination with LV diastolic dysfunction.13 Over the last decade, a new paradigm has been presented, describing a sequence of events leading to HFpEF. A systemic proinflammatory state induced by concomitant comorbidities is thought to be at the core the pathological process in HFpEF.12 As illustrated in figure 2, HFpEF is a caused by diverse underlying conditions and comorbidities, resulting in a population of people with diverse characteristics. Future vision for the treatment of HFpEF is a personalised approach including precise risk stratification, using targeted therapies and preventative intervention.

Illustration of the many faces of the HFpEF phenotype reflecting heterogeneous and complex underlying pathophysiology in HFpEF syndrome. In the future, HFpEF treatment should be based on personalised approach, precise risk stratification with targeted therapies and preventative intervention. Graphic inspired by Professor C Miller, with permission. HFpEF, heart failure with preserved ejection fraction.
In HFpEF, the myocardium displays a number of functional and structural abnormalities.7 Comorbid conditions initiate a systemic proinflammatory state which leads to coronary microvascular endothelial inflammation. This inflammation ignites a cascade of changes at the molecular level that promotes myocyte hypertrophy and interstitial fibrosis. These contribute to increased LV diastolic stiffness, which slows LV relaxation. LV diastolic filling pressures increase, leading to impaired cardiac output, which gives rise to symptoms of HF.7 12 Altered intramyocardial signalling, energetic abnormalities and impaired density and autoregulation of the microcirculation have also been noted. The remodelling in HFpEF differs from that seen in HFrEF, driven primarily by a loss of cardiomyocytes.
Diagnostic process
The most common symptom in HFpEF is breathlessness on exertion and reduced exercise capacity. Therefore, it is important to collect a detailed clinical history focusing on change in exercise capacity over time and current exercise tolerance. Although breathlessness on exertion is highly sensitive in diagnosing HF, it has only 50% specificity for identifying a cardiac cause4; hence, clinical history should focus on all non-cardiac causes of breathlessness, such as lung disease and deconditioning.
The assessment of a patient presenting with symptoms and/or signs of HFpEF includes detailed clinical history with consideration of current comorbidities such as obesity, hypertension, DM, COPD, CKD, coronary artery disease (CAD), AF, metabolic syndrome, poor physical activity, deconditioning and all modifiable risk factors. Importantly in women, it must focus on history of eclampsia, pre-eclampsia, therapies for breast cancer.14 Medication history should focus on all prescribed drugs potentially precipitating HFpEF (chemotherapy and immune modulating drugs) and over-the counter drugs such as non-steroidal anti-inflammatory medication, supplements and herbal remedies.15 Family history should focus on history of CAD, HF of all causes, cardiomyopathy, amyloidosis and genetic conditions (hypertrophic cardiomyopathy and muscular dystrophies).
Clinical examination should focus on examination of radial pulse rhythm and rate and blood pressure (BP). Signs of volume overload (raised jugular venous pressure (JVP), peripheral oedema and pulmonary crepitations) may not be obvious in early stages of HFpEF. Cardiac auscultation may reveal systolic flow murmurs or murmurs from valvular abnormalities. Assessment of body build with weight, body mass index and presence of central obesity is essential. While there are no specific ECG findings to indicate HFpEF, ECG is recommended to detect AF and left ventricular hypertrophy (LVH).
First-line laboratory blood tests should include NP, full blood count, ferritin and transferrin saturation to exclude anaemia, which may precipitate symptoms of breathlessness. Renal function including urea, creatinine, electrolytes and estimated glomerular filtration rate (eGFR), and HbA1c must be checked. Liver function tests, thyroid function tests and lipid profile are useful in assessing the risk of metabolic syndrome. Although NP levels have been shown to have high negative predictive value in excluding HF (when levels are <125 pg/mL for N-terminal pro B-type natriuretic peptide (NT-proBNP) and <35 pg/mL for brain natriuretic peptide (BNP) as per ESC guidelines and for UK practitioners NT-proBNP level less than 400 pg/mL as per National Institute for Health and Care Excellence (NICE) guidelines), approximately 20% of patients with HFpEF will have normal NP levels.7 The reason for normal NP levels in HFpEF is due to the mechanism in which NPs are released. NPs are released due to high LV diastolic wall stress. Bearing in mind that the LV diastolic wall stress is inversely proportional to the wall thickness, in cases with mild LVH (which is common in HFpEF), the effect of diastolic LV wall stress may be diminished and NP may not be released. In contrast to HFpEF, the LV diastolic wall stress in HFrEF more commonly triggers release of NP in patients with dilated LV and thinned myocardial walls. Another reason for NP levels below the cut-off thresholds is obesity.16 It is worthwhile noting that NP levels can be raised due to a variety of cardiac and non-CV causes other than HF. Pathological processes leading to the increased LV diastolic stress or myocardial injury, resulting from acute ischaemia, inflammation or iatrogenic causes (eg, cardioversion), can cause high levels of NP. Non-cardiac conditions can increase serum NP via indirect mechanisms such as impaired metabolism, low creatinine clearance, systemic hypoxia, starvation and dehydration. Figure 3 highlights the cardiac and non-cardiac causes of raised NP levels.

Cardiac and non-cardiac causes of raised natriuretic peptides (serum levels >125 pg/mL for N-terminal probrain natriuretic peptide or >35 pg/mL for brain natriuretic peptide). *Denotes hypertrophic or restrictive cardiomyopathy. ACS, acute coronary syndrome; COPD, chronic obstructive pulmonary disease; ICD, implantable cardioverter–defibrillator; LV, left ventricular; PE, pulmonary embolism.
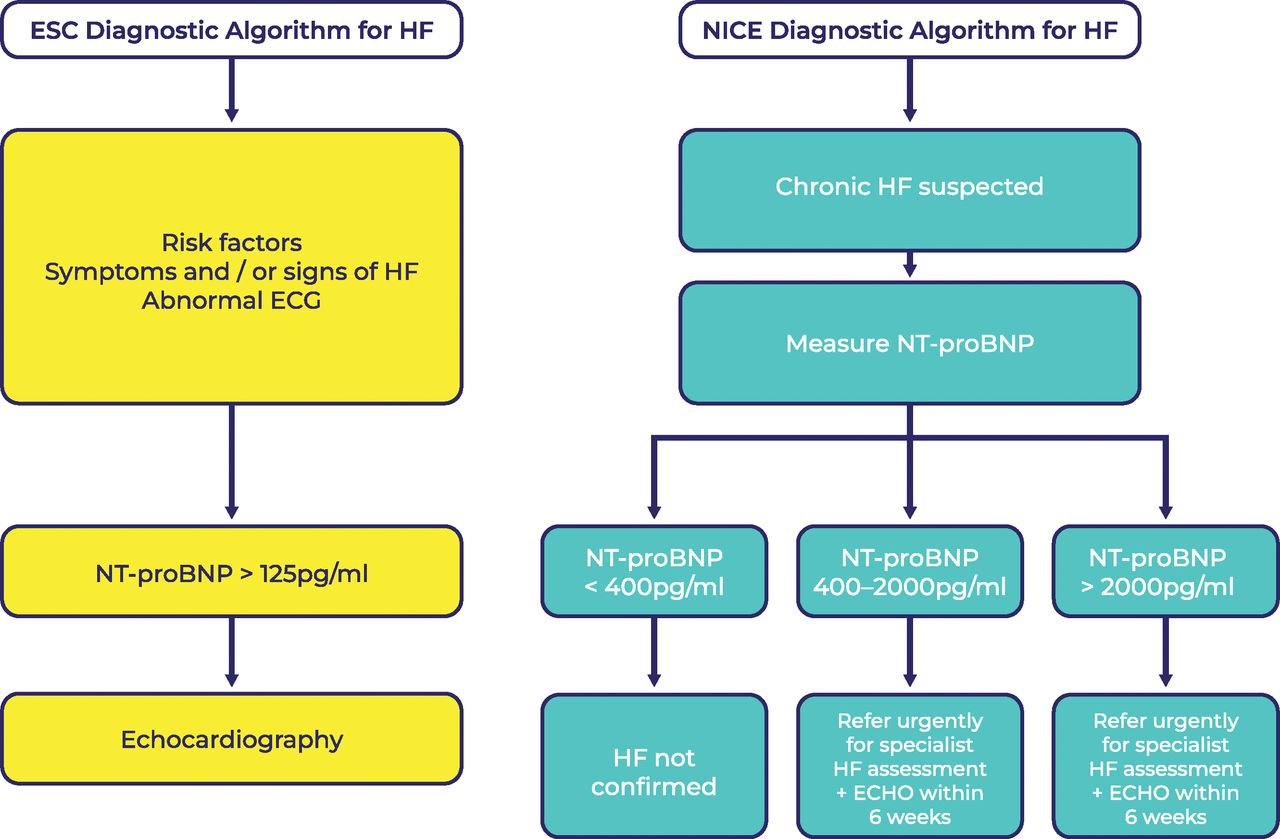
We would like to point out that there is a discrepancy in the cut-off points for NT-proBNP and BNP levels between ESC and NICE HF guidelines.17 In figure 4, we present the differences between the ESC and NICE diagnostic algorithm for HF, which would be of particular use to the UK-based practitioners. Despite higher cut-off points for NT-proBNP levels, NICE recommends a discussion with a physician with subspecialty training in HF, if a clinical suspicion of HF persists in patients with NT-proBNP levels of <400 pg/mL.

Diagnostic algorithms for HF: European Society of Cardiology 2021 HF guidelines4 and NICE 2018 HF guidelines.17 Reproduced with permission from Br J Cardiol 2022;29(suppl 2):S3–S6, doi: 10.5837/bjc.2022.s06. ECHO, echocardiogram; ESC, European Society of Cardiology; HF, heart failure; NICE, National Institute for Health and Care Excellence; NT-proBNP, N-terminal probrain natriuretic peptide.
Transthoracic echocardiogram (ECHO) should be offered to every patient presenting with symptoms suggestive of HF and elevated NP levels. ECHO is useful in identifying other causes of breathlessness such as HFrEF, valvular heart disease and right ventricle pathologies, such as primary and secondary pulmonary hypertension. All ECHO measurements should be performed in accordance with the most recent guidelines of the European Association of Cardiovascular Imaging or American Society of Echocardiography.18 19 Of note, reduced longitudinal strain is a good predictor of HF, and poor longitudinal strain is strongly linked to worse outcomes in HFpEF.20 Diagnosis of HFpEF may pose a challenge for clinical centres with no access to specialist tests and/or HF expertise. Thus, there has been a key change to the ESC 2021 HF guidelines,4 which recommends a simple three-step diagnostic pathway to enable effective detection of HFpEF.
Simple three-step diagnostic pathway:
Signs and symptoms of HF.
An LVEF of ≥50%.
Objective evidence of cardiac structural and/or functional abnormalities consistent with LV diastolic dysfunction/raised LV filling pressures, including raised NPs (see table 1).
Objective evidence used in the diagnosis of HFpEF
If resting ECHO and laboratory indicators are inconclusive, a diastolic stress test can help. Invasive haemodynamic exercise testing is used to confirm the diagnosis of HFpEF. A pulmonary capillary wedge pressure (PCWP) of ≥15 mm Hg at rest or ≥25 mm Hg with exercise or LV end-diastolic pressure of ≥16 mm Hg (at rest) is deemed diagnostic.
Current guidelines do not require gold standard testing in every patient to make a diagnosis of HFpEF. Because in majority of patients the diagnosis can be made based on the combination of symptoms, signs, ECHO findings and NT-proBNP level, further testing is often not necessary. However, for those cases where patients present with persistent symptoms but simple tests do not confirm a diagnosis of HFpEF, we can consider either exercise stress ECHO or invasive haemodynamic exercise testing.21 Unfortunately, there are no real-world data suggesting how frequently the invasive haemodynamic exercise testing is used in clinical practice.
Because many patients with HFpEF have only symptoms during exertion, acquiring ECHO during exercise can unmask LV diastolic and systolic functions.7 Two most studied parameters indicative of increase in PCWP and pulmonary artery systolic pressure are early diastolic transmitral flow velocity to early diastolic mitral annular tissue velocity (E:e') ratio and the tricuspid regurgitation peak velocity.21 Guidelines emphasise that the larger the amount of non-invasive indicators of raised LV filling pressures, the greater the likelihood of a diagnosis of HFpEF.4
Therapy for HFpEF
The goals of therapy for patients with HFpEF are to reduce symptoms, improve functional status and lower the risk of hospital admission.
Diuretics: the cornerstone of therapy
Patients with HFpEF and documented volume overload should be offered diuretic therapy.4 10 Therapy is initiated with loop diuretics, type and dose depending on the severity of volume overload. For those patients with diuretic resistance, sequential nephron blockade can be achieved using thiazide/thiazide-like diuretics and/or mineralocorticoid receptor antagonists (MRAs), the latter of these has been included in the 2022 AHA HF guidelines with class 2b level of recommendation for treatment of HFpEF.10
Treating underlying comorbidities
Up until 2022, the core of therapeutic recommendations in HFpEF was a focus on delivering therapy for underlying comorbidity and treating modifiable HF risk factors. Hypertension, AF, CAD, hyperlipidaemia, obesity, anaemia, DM, CKD and sleep apnoea are conditions that are frequently associated with HFpEF. There is no evidence for HFpEF-specific management of these conditions.
Even though multiple randomised controlled trials (RCTs) using ACE inhibitors (ACEis), angiotensin II receptor blockers (ARBs), MRAs, beta blockers and angiotensin–neprilysin inhibitors (ARNI) in patients with HFpEF did not show mortality benefit or reduction in hospitalisation,4 their effects on the course of HFpEF were shown in subgroup analyses.22 23 Therefore, in selected patients with HFpEF, MRAs, ARBs and ARNIs may be considered to decrease hospitalisations, particularly among patients with LVEF on the lower end of this spectrum, and their use is given a class 2b recommendation in 2022 HF guidelines from AHA/American College of Cardiology (ACC)/Heart Failure Society of America(HFSA).10
Hypertension
Hypertension is the leading cause of HFpEF, with a prevalence ranging from 60% to 89%,4 and BP control is well established for preventing HF. Effective treatment leads to regression of LVH, with ARB, ACEi and calcium channel blockers, causing more effective LVH regression than beta blockers or diuretics. Poorly controlled hypertension may precipitate episodes of decompensation.4 Patients with HFpEF frequently have an exaggerated BP response to exercise and may present with hypertensive acute pulmonary oedema. Exact BP targets are uncertain in HFpEF, and typically the goal is similar as for the general population. Evaluation of the patient’s age and comorbidities (ie, diabetes, CKD, CAD, valvular heart disease and stroke) should guide personalised choice of antihypertensive agents. In the case of uncontrolled HF symptoms or repeated hospitalisations despite reasonable BP control, the target should be reduced. When treating to a lower BP goal, carefully monitor dose adjustments as patients with HFpEF can have an exaggerated hypotensive response to vasodilator therapy.
Diabetes
Despite favourable benefits of sodium–glucose cotransporter-2 (SGLT2) inhibitor in individuals with HFpEF (see the SGLT2 inhibitor use in HFpEF section), these medicines are recommended as primary type 2 diabetes treatment only for patients at highest CV risk or if metformin is contraindicated or not tolerated.24 To reduce the risk of hypoglycaemia when treating with SGLT2 inhibitor in patients on insulin or on sulfonylureas, the dose of these may need to be reduced. SGLT2 inhibitor should be avoided in all patients with type 1 DM and type 2 DM and prior diabetic ketoacidosis (DKA) or a condition predisposing to DKA (including pancreatic insufficiency, drug or alcohol addiction, and prolonged fasting). Use is not recommended if eGFR is <15–20 mL/min/1.73 m2.
Chronic kidney disease
Patients with HFpEF and CKD should be treated with evidence-based therapies that reduce the progression of CKD by renin–angiotensin–aldosterone system inhibitors and SGLT2 inhibitor therapy. There is an expected initial decline in eGFR on initiation of SGLT2 inhibitor of approximately 4 mL/min/1.73 m2; however, in longer term, the rate of eGFR decline is slowed compared with patients not on SGLT2 inhibitor. In the Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) trial, patients with CKD, with or without diabetes, had a lower risk of a decline in estimated GFR of at least 50%, end-stage kidney disease, or death from renal or CV causes when treated with dapagliflozin versus placebo.25 We invite readers to a position paper from the ESC ad hoc task force on SGLT2 inhibitor on cardiac, renal and metabolic effects of SGLT2 inhibitor.26
Chronic coronary syndrome
Despite CAD and ischaemic heart disease being more strongly associated with HFrEF, CAD is also common in HFpEF, with prevalence in epidemiological and registry studies of 35%–60%.9 Due to exercise intolerance and the impact of increasing end-diastolic LV pressures, it can be challenging to document ischaemia using non-invasive and invasive testing in patients with HF. To determine the existence and degree of CAD and to assess the need for revascularisation, CT coronary angiography should be considered in patients with a low to intermediate pretest probability of CAD or those with equivocal non-invasive stress tests, while invasive coronary angiography may be considered in patients with an intermediate to high pretest probability of CAD.4 There are no prospective trials of revascularisation in patients with HFpEF. Medical therapy with beta blockers, long-acting nitrates, calcium channel blockers, ivabradine, ranolazine, trimetazidine, nicorandil and their combinations should be considered in HFpEF for angina relief.4
Atrial fibrillation
There is a lack of large RCT evidence to guide specific therapy for individuals with HFpEF and AF. It is recommended that patients with HFpEF and chronic AF have adequate rate control, with beta blockers and non-dihydropyridine calcium channel blockers frequently used as first-line agents. Recently, Rate Control Therapy Evaluation in Permanent Atrial Fibrillation (RATE-AF), an open-label trial in elderly patients with AF and symptoms of HF (most with HFpEF), compared the use of bisoprolol to digoxin.27 The primary outcome of QoL was comparable between the two groups at 6 months. However, numerous secondary QoL objectives, including functional ability and NT-proBNP decrease, preferred digoxin at 12 months, with both groups having a comparable decrease in heart rate. Beta blockers caused more adverse effects, such as dizziness, drowsiness and hypotension, than digoxin.
RCTs comparing rate control to rhythm control with antiarrhythmic medications have not demonstrated an advantage of rhythm control. Recent RCTs involving ablation indicate that ablation may be better to antiarrhythmic medicines for rhythm control strategies. If rate and rhythm control strategies fail, patients with HFpEF and difficult-to-control heart rates may benefit from atrioventricular node ablation and placement of a permanent pacemaker; when LVEF is >50%, there is no evidence that cardiac resynchronisation therapy (CRT) is superior to right ventricular pacing.10 This paper does not cover the entire care of AF, and we refer readers to ESC practise guidelines on AF-specific care.28
SGLT2 inhibitor use in HFpEF
The landmark trials EMPEROR-Preserved,29 PRESERVED-HF30 and DELIVER31 showed the positive impact of SGLT2 inhibitor on outcomes in patients with HFpEF. The EMPEROR-Preserved trial showed 21% reduction in the primary composite endpoint of time to HF hospitalisation or CV death in the empagliflozin arm. The benefit of empagliflozin first reached statistical significance at 18 days after randomisation and maintained significance thereafter. While there was no benefit on all-cause mortality, empagliflozin resulted in a significant reduction in total HF hospitalisations, a decrease in the slope of the eGFR decline, and a modest improvement in QoL at 52 weeks. Importantly, the benefit was similar, irrespective of the presence or absence of diabetes at baseline.
PRESERVED-HF demonstrated that treatment with dapagliflozin significantly improved symptoms, physical limitations and exercise function on 6 min walking distance in patients with HFpEF with and without type 2 diabetes.30 The results have implication on clinical practice, and they were reflected in the new 2022 HF guidelines from AHA/ACC/HFSA,10 stating that SGLT2 inhibitor can be beneficial in decreasing HF hospitalisations and CV mortality (class 2a).
Dapagliflozin reduced the combined risk of worsening HF or CV death in patients with HF and mildly reduced or preserved ejection fraction,31 with a relative risk reduction of 18%. The results of this trial will have impact on future clinical HF guidelines on pharmacotherapy in HFpEF.
The benefit of SGLT2 inhibitor on mortality and hospitalisation has been shown in patients with HFrEF in the DAPA-HF trial. Patients who received dapagliflozin had a 26% reduction in the primary endpoint (CV death, hospitalisation or urgent HF visit) compared with patients who obtained standard treatment alone, with significant reduction in both worsening HF and CV death components of the primary endpoint. In both diabetics and non-diabetics, identical outcomes were seen.32
SGLT2 inhibitors are not currently included in most recent European guidelines on treatment of HF, as the results of the trials were available after the guidelines were published. However, there are two guidelines currently in development by NICE in the UK: ‘Empagliflozin for treating chronic heart failure with preserved or mildly reduced ejection fraction [ID3945]’33 and ‘Dapagliflozin for treating chronic heart failure with preserved or mildly reduced ejection fraction [ID1648]’.34 The expected date of publication of aforementioned guidelines is yet to be confirmed. As mentioned earlier, SGLT2 inhibitors are recommended though in patients with type 2 DM who do not tolerate metformin.24
Follow-up for patients with HFpEF
The frequency of clinical evaluation in ambulatory patients with HFpEF is determined by the severity of HF symptoms and comorbid conditions (eg, CKD), but it is recommended that patients with HFpEF have a clinical review every 6 months. Patients should be reviewed quickly with deterioration of clinical status, within 2 weeks of medication change, and within 7–14 days of hospital discharge after HF decompensation29 to significantly reduce the chance of readmission. It is important to evaluate patients with worsening HF signs or symptoms for cardiac (eg, rhythm disorders and ischaemia) and non-cardiac (eg, worsening diabetes and hypothyroidism) causes of HFpEF exacerbation. NP level may be useful during symptom re-evaluation. However, low levels of NP can be present even in very symptomatic patients; hence, testing should not be guided by NP levels alone.
Patient education
The management of a patient with HFpEF requires a multidisciplinary approach and good patient education. In addition to pharmacological treatment, patients with HFpEF should be offered a comprehensive guide and support in implementing and maintaining lifestyle changes and self-care strategies. Programmes for managing chronic diseases and instruction in self-management may lower the probability of hospital admission for people with HFpEF.35
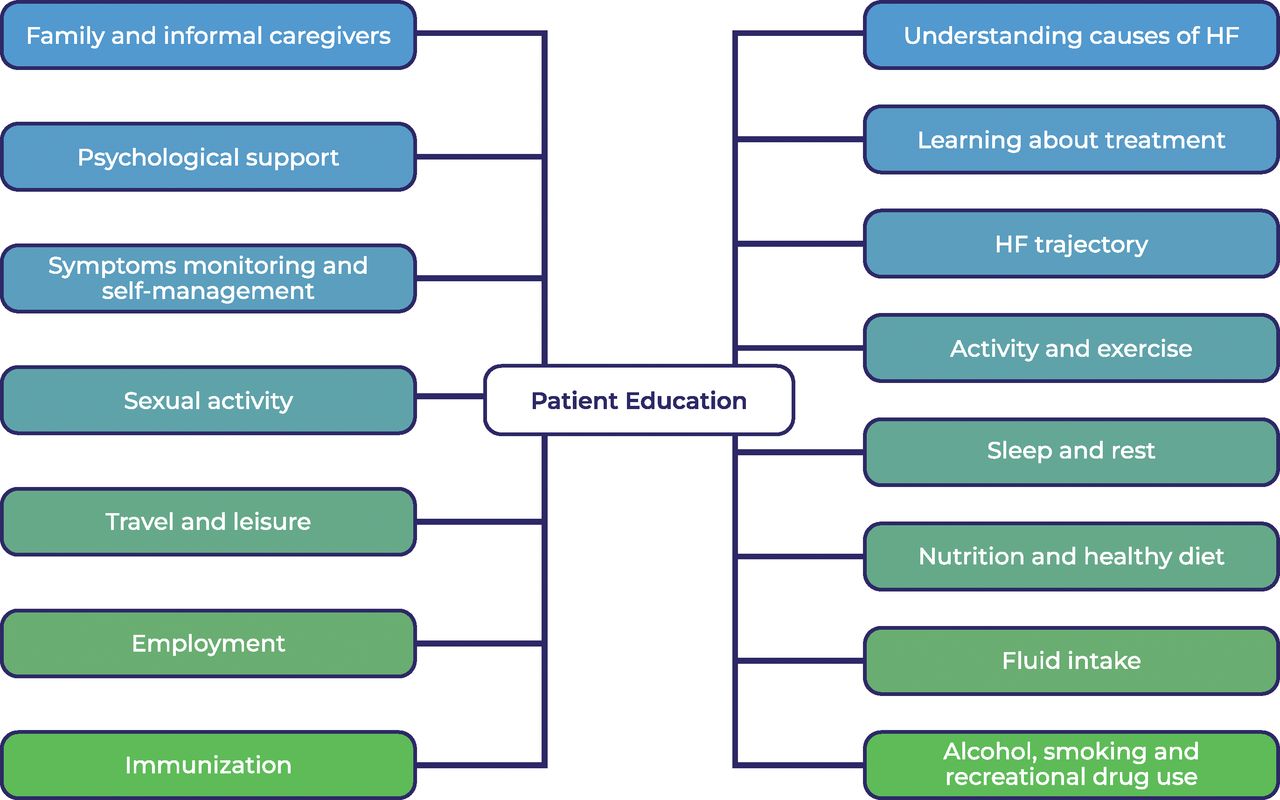
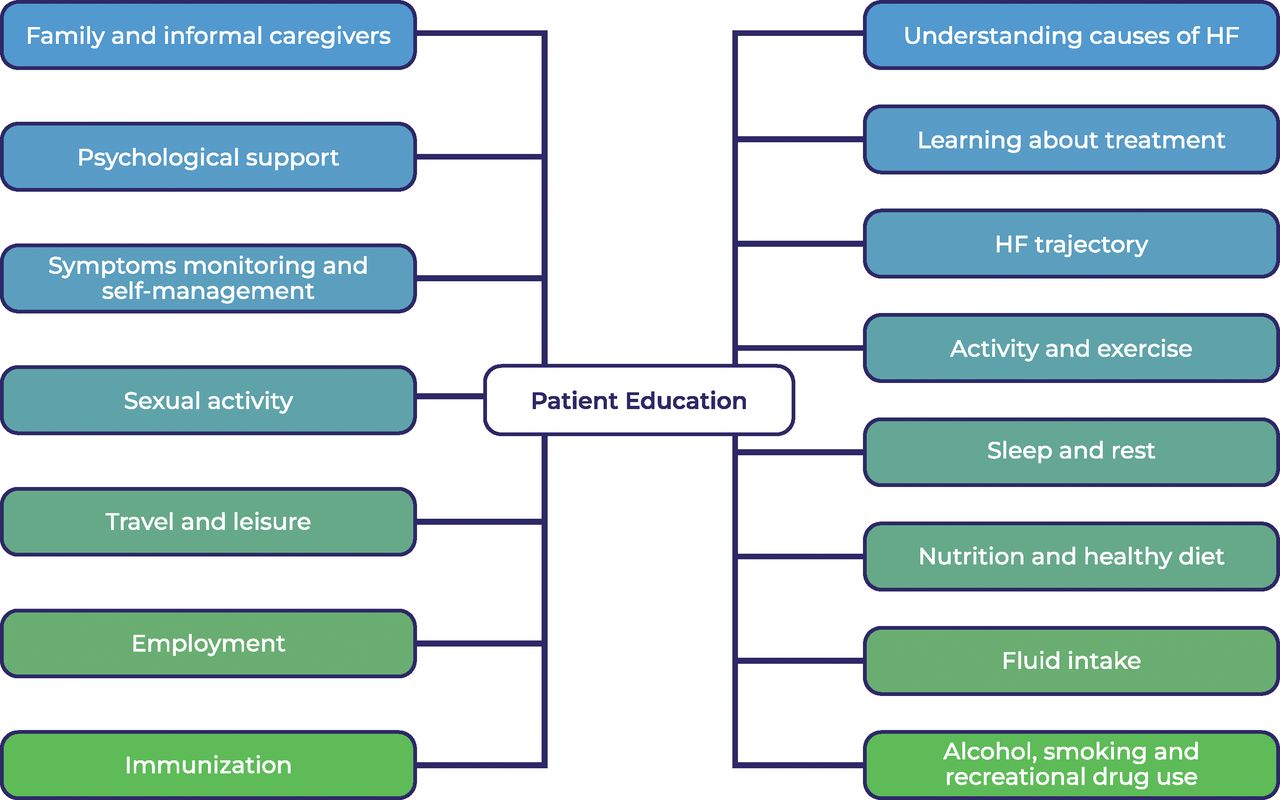
Participation in structured exercise-based programmes, cardiac rehabilitation, weight loss programmes and dietary interventions not only can lead to improved exercise tolerance36 but also is associated with lower odds of all-cause mortality, hospitalisations, incident stroke and incident AF in patients with HFrEF and HFpEF.37 Meta-analyses of multidisciplinary team (MDT) care demonstrate a reduction in death as well as hospital admissions in favour of MDT care.38–40 The studies included in the analyses rarely excluded patients with HFpEF; therefore, MDT therapy may also improve survival as well as reduce hospital admissions. Until recently, many HF MDT services intentionally exclude patients with HFpEF due to a perceived lack of effective treatments. Given the restricted availability of high-quality structured programmes for patients with HF, it is extremely difficult to determine which individuals with HFpEF are most likely to benefit or should be given priority access, as well as how to deliver suitable services. However, it is worth stressing that HF experts agree that patients with HF, of any type, ideally should have access to rehabilitation programmes. Figure 5 summarises important aspects of the patient education. Each contact with the patient should be seen as an opportunity to ensure that patients understand their condition and know how to manage it to achieve and maintain a high QoL.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Education and self-care topics to be covered by the multidisciplinary team caring for patients with HF. HF, heart failure.
Expert’s glimpse of what the future should hold
With the recent publication of the DELIVER trial results in combination with those of EMPEROR-Preserved and PRESERVED-HF, we expect to see an update of the ESC guidelines to reflect the use of SGLT2 inhibitor for patients with HFpEF. Due to variations in coexisting comorbid conditions driving the condition, multiple clinical phenotypes and underlying pathophysiologies are responsible for the manifestation of HFpEF. Despite this, current clinical practice lacks personalised and targeted treatment options for patients with this complex clinical syndrome. Future clinical practice should strive to deliver personalised therapy for this highly prevalent and growing cohort of patients.
Summary
The pathophysiology of HFpEF is complex, and systemic changes related to various comorbid conditions drive myocardial dysfunction in myriad differing ways. The diagnosis of HFpEF can seem complex, but recent guidelines recommend use of a simple three-step diagnostic pathway to enable effective diagnosis in the majority of cases. For patients whose initial testing is inconclusive, referral to specialist centres for additional exercise testing should be considered. Regardless of LVEF, a diagnosis of HF has significant negative effects on both the quality and quantity of life. HFpEF represents 50% of all HF cases, and these patients are currently recognised as having the greatest unmet need in cardiology, with many HF services not offering care to this patient group. Due to an ageing population and increasing prevalence of comorbidities, HFpEF incidence is rising. Outcomes in HFpEF are comparable with those in HFrEF; therefore, intervention should be implemented early to prevent mortality, morbidity and poor patient reported outcomes. HFpEF is associated with multimorbidity, with as many as 50% of patients having five or more significant comorbidities. Management of the comorbidities and diuretic therapy have long been central in the treatment of HFpEF with the aim of reducing symptom burden and preventing hospitalisation, but without clinical trial data in support of this. However, breakthrough RCT data on SGLT2 inhibitor use in HFpEF (in particular EMPEROR-Preserved and DELIVER) show improved patient-reported outcomes, and reduction in the primary endpoint of heart failure hospitalisations and CV death. SGLT2 inhibitor therapy for HFpEF has been given a class 2 a recommendation in the 2022 AHA HF guidelines, and we would expect an update in future European HF guidelines and NICE clinical guidance.
Key messages
Approximately 50% of patients with heart failure (HF) have preserved ejection fraction.
The incidence of heart failure with preserved ejection fraction (HFpEF) increases with age; other risk factors include female gender, hypertension, obesity, metabolic syndrome and coronary artery disease.
HFpEF is associated with multimorbidity, with as many as 50% of patients having five or more significant comorbidities (including hypertension, diabetes mellitus, chronic kidney disease, atrial fibrillation and anaemia).
Elevated natriuretic peptide (NP) levels are a feature for most patients; however, an estimated 20% have normal NP levels.
Outcomes in HFpEF are comparable to those for HF with reduced ejection fraction; hence, early intervention should be implemented to prevent mortality, morbidity and poor patient-reported outcomes.
Therefore, accurate and prompt diagnosis is critical.
Use of a simple three-step diagnostic pathway can enable an HFpEF diagnosis for the majority of patients.
For those with inconclusive results, referral to specialist centres for exercise testing should be considered.
Treatment of fluid overload and targeted therapy for associated comorbid conditions is recommended.
The results of EMPEROR-Preserved and PRESERVED-HF clinical trials support the use of sodium–glucose cotransporter-2 inhibitors as a new treatment option in patients with HFpEF, with class 2a recommendation for use in the 2022 American Heart Association/American College of Cardiology/HFSA HF guidelines.
The results of DELIVER trial show that use of SGLT2 inhibitors in patients with HFpEF showed reduction of the combined risk of worsening HF or cardiovascular death.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the 'Take the Test' link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Many thanks to Professor Christopher Miller for kind permission to adapt his infographic illustrating phenotypes and contributing pathophysiology in heart failure with preserved ejection fraction.
References
Footnotes
Twitter @apiadlo, @drpmcampbell
Contributors There was equal contribution from both authors. The final document reviewed and edited by PC.
Funding This work was supported by the Public Health Agenacy and Health and Social Care Research and Development Department in Northern Ireland [grant number EAT/5495/18, 2018]; Southern Health and Social Care Trust, Research and Development Department .
Competing interests AJ-P was a recipient of a Doctoral Fellowship Award from the Research and Development department of the Public Health Agency, Health and Social Care in Northern Ireland and received speaker honorarium from Vifor-Pharma. PC received speaker honoraria from Novartis, Boehringer Ingelheim, Vifor-Pharma, Pfizer and AstraZeneca and institutional research funding from AstraZeneca and is a member of the advisory board for EMPEROR-Preserved.
Provenance and peer review Commissioned; externally peer reviewed.
Author note References which include a * are considered to be key references.