Article Text

Abstract
Objective The primary objective was to study the risk of acute myocardial infarction (AMI) and coronary heart disease (CHD) in patients with familial hypercholesterolaemia (FH) and compare with the risk in the general population.
Methods Patients with an FH mutation but without prior AMI (n=3071) and without prior CHD (n=2795) were included in the study sample during 2001–2009. We obtained data on all AMI and CHD hospitalisations in Norway. We defined incident cases as first time hospitalisation or out-of-hospital death due to AMI or CHD. We estimated standardised incidence ratios (SIRs) with 95% CIs with indirect standardisation using incidence rates for the total Norwegian population stratified by sex, calendar year and 1 year age groups as reference rates.
Results SIRs for AMI (95% CIs) were highest in the age group 25–39 years; 7.5 (3.7 to 14.9) in men and 13.6 (5.1 to 36.2) in women and decreased with age to 0.9 (0.4 to 2.1) in men and 1.8 (0.9 to 3.7) in women aged 70–79 years. Similarly, SIRs for CHD were highest among patients 25–39 years old; 11.1 (7.1–17.5) in men and 17.3 (9.6–31.2) in women and decreased 2.4 (1.4–4.2) in men and 3.2 (1.5–7.2) in women at age 70–79. For all age groups, combined SIRs for CHD were 4.2 (3.6–5.0) in men and 4.7 (3.9–5.7) in women.
Conclusion Patients with FH are at severely increased risk of AMI and CHD compared with the general population. The highest excess risk was in the youngest group aged 25–39 years, in both sexes.
- acute myocardial infarction
- lipoproteins and hyperlipidemia
- coronary artery disease
- genetics
- cardiac risk factors and prevention
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- acute myocardial infarction
- lipoproteins and hyperlipidemia
- coronary artery disease
- genetics
- cardiac risk factors and prevention
Introduction
Heterozygous familial hypercholesterolaemia (FH) is an inherited condition with elevated circulating low-density lipoprotein levels from birth.1 2 It affects approximately one in every 200–300 people3 4 and increases the risk of premature coronary heart disease (CHD).5–10 Patients with FH are recommended a healthy lifestyle and statin treatment from age 8 to 10 years,11 12 but uncertainty remains about any residual risk in treated subjects.4 13–17 Large cohorts and long follow-up are needed to generate such data, which is difficult to establish for FH.18 In one large cohort study, the relative risk for coronary mortality in patients aged 20–59 declined from an 8-fold increased risk prior to statins became available to 3.7-fold thereafter.13 The primary aim of the present study was to relate the incidence of acute myocardial infarction (AMI) and CHD per year in the complete cohort of all patients with genetically proven FH in Norway to the incidence of these diseases in the total Norwegian population of about 5 million people. We used standardised incidence ratios (SIRs) during 2001–2009 for the primary aim. The secondary aim was to estimate SIRs for the associated procedures: percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG) and total coronary revascularisation (CR) procedures during the same period.
Methods
Study design
This is a registry-based prospective cohort study of all genotyped patients with FH in Norway. The study was perfomed according to the protocol approved in 2011 (supplementary file 1). We followed all patients who were included in the Unit for Cardiac and Cardiovascular Genetics (UCCG) Registry at 31 December 2009 for first time incident AMI and CHD events as well as first-time event of PCI, CABG and total CR during the period 2001 throughout 2009.
Patient involvement
We planned and discussed the study in meetings with the patient organisation for patients with FH in Norway who informed their members through a bi-annual paper magazine sent to all members.
UCCG registry
All patients with genetically diagnosed FH in Norway are included in the National UCCG Registry after written informed consent. Prior to the registry linkage all patients received a letter and were offered to be removed from the list and not participate in the registry linkage (supplementary file 2). At 31 December 2009, there were 4273 patients with FH registered of whom 8 were homozygous and of whom 3 had CHD.19 Sex, birth year, date and age of genetic diagnosis were extracted from the registry. The frequency of the most common mutations in the cohort and the registry is further described elsewhere.20–22 After the time of diagnosis, total serum cholesterol mean (SD) was 220 (58) mg/dL (5.7 (1.5) mmol/L), low-density lipoprotein cholesterol (LDL-C) was 151 (50) mg/dL (3.9 (1.3) mmol/L) and 89.1% used lipid-lowering drugs in the cohort.20
Cardiovascular outcomes and data linkage
We obtained data on all hospitalisations in Norway during 1994–2009 for AMI, CHD, PCI, CABG and total CR from the Cardiovascular Disease in Norway project (CVDNOR, http://www.cvdnor.no), a collaborative project between the University of Bergen and the Norwegian Knowledge Centre for the Health Services. Patient’s sex, age, date and time of admission and discharge, discharge diagnoses and diagnostic and surgical procedures are included in the database. We obtained data on death from the Norwegian Cause of Death Registry (NCoDR) containing information on date and cause of death (underlying, contributing and immediate causes) for all deaths among Norwegian residents.
We followed patients for endpoints through linkage with the NCoDR and CVDNOR by using the unique personal identification number for each Norwegian resident. Data were given according to the International Classification of Diseases, version 9 (ICD9) or version 10 (ICD10). Definition of AMI is the ICD9 code 410 or the ICD10 codes I21 and I22. CHD is defined as the ICD9 codes 410–414 or ICD10 codes I20–I25.
An incident event of AMI is defined as a hospitalisation with AMI as main or supplementary diagnosis or a death with CHD as the underlying cause of death without any prior hospitalisations with AMI. During 1994–2009, the definition of AMI in Norway changed. During the 1990s, the WHO criteria of 1979 for AMI was used.23 From 2000, AMI was defined according to the new American College of Cardiology/European Society of Cardiology definition.24 In 2007, the Universal Definition of MI was implemented.25
We defined an incident event of CHD as a hospitalisation with CHD as main or secondary diagnosis or a death with CHD as the underlying cause of death without any prior hospitalisations with CHD.
PCI was defined as code FNG in the Nordic Medico-Statistical Committee (NOMESCO) classification of medical (NCMP) and surgical (NCSP) code FNG or as codes 3294, 3236 or 3239 in the Norwegian classification of medicinal procedures; third edition, 1995 (SIF-95). CABG definition is NCMP/NCSP codes FNA–FNF or codes 3112–3129 in SIF-95. Total CR definition is NCMP/NCSP codes FNA–FNG and codes 3112–3129, 3294, 3236 and 3238 in SIF-95.
To analyse the first time events, we required 7 years of observation free of events prior to the start of follow-up. Patients registered in the UCCG later than 31 December 2009 and patients with any endpoint in question before 2001 were excluded from the analyses. Previous studies have shown that a washout period of 7 years results in only 3%–4% overestimation of incident events of AMI.26
We counted events among patients with FH from after the day they were included in the UCCG register and calculated the incidence of first occurrence of the endpoint in question, death from other causes or end of follow-up, whichever came first, during the period 1 January 2001 to 31 December 2009 for patients with FH and the entire Norwegian population. The follow-up time for each individual was split over calendar years and the attained age for each individual was updated for each calendar year.
Statistical analysis
We calculated unadjusted incidence rates for each endpoint in 2001–2009 stratified by sex and age. For each age stratum, the incidence rates were calculated as the number of events per 1000 person-years of follow-up for patients with FH and the entire population. We calculated SIRs for each endpoint using indirect standardisation with incidence rates for the total Norwegian population as reference rates.27 Expected number of incident events was calculated for each combination of 1 year age group and calendar year in the UCCG Registry as time spent in the cohort multiplied by the incidence rate for the same combination of birth year and calendar year in the total Norwegian population. Calculations were performed for men and women separately and in combination. Total expected number of incident events for men and women were obtained by summing expected number of events over 1 year age groups and calendar years.
SIR was calculated as the observed number of events divided by the expected number of events. Confidence limits were obtained using the normal approximation to the Poisson distribution.
Linear trend in SIR for AMI and CHD across calendar periods (2001–2003, 2004–2006 and 2007–2009) were tested using orthogonal polynomial contrasts after Poisson regression models with observed number of events as the outcome, the logarithm of expected number of events as offset and calendar period as a three-level factor variable. P <0.05 were considered statistically significant. All analyses were performed using Stata V.14.
Results
Table 1 shows the characteristics of the study sample. Mean (SD) age at the time of genetic diagnosis was 32.7 (18.6) years, 31.2 (18.1) years for men versus 34.1 (18.9) years for women (P<0.001).
Characteristics of the patients with familial hypercholesterolaemia (FH) in the Unit for Cardiac and Cardiovascular Genetics (UCCG) Registry
We excluded 1069 of the 4273 patients registered because they were below 25 years of age during the complete follow-up period for accurate calculation of CHD. Further, we excluded 329 because they had an event before inclusion in the registry and 80 patients because they had an event during the 7-year wash-out period prior to 2001. Thus, we analysed a cohort of 2795 patients for their first incident CHD during 2001–2009.
Likewise, for MI calculations, we excluded 1069 patients younger than 25 years during the study period, 108 had an AMI event before inclusion in the registry and 25 had their first AMI event in the wash-out period, leaving a cohort of 3071 patients for analyses of incident AMI.
Mean (SD) age at first AMI and CHD event were 56.2 (13.4) and 55.1 (13.0) years, respectively. Tables 2 and 3 show the SIRs for AMI and CHD in patients with FH according to sex, and figure 1 shows the SIRs for AMI and CHD for both sexes combined. In total, SIR for AMI (95% CI) was 2.3 (1.8–3.0) in men and 2.3 (1.6–3.2) in women. SIR for CHD (95% CI) was 4.2 (3.6–5.0) in men and 4.7 (3.9–5.7) in women. Both the SIRs for AMI and CHD were highest in the youngest age group 25–39 years in both sexes.
Acute myocardial infarction during 2001–2009
Coronary heart disease during 2001–2009
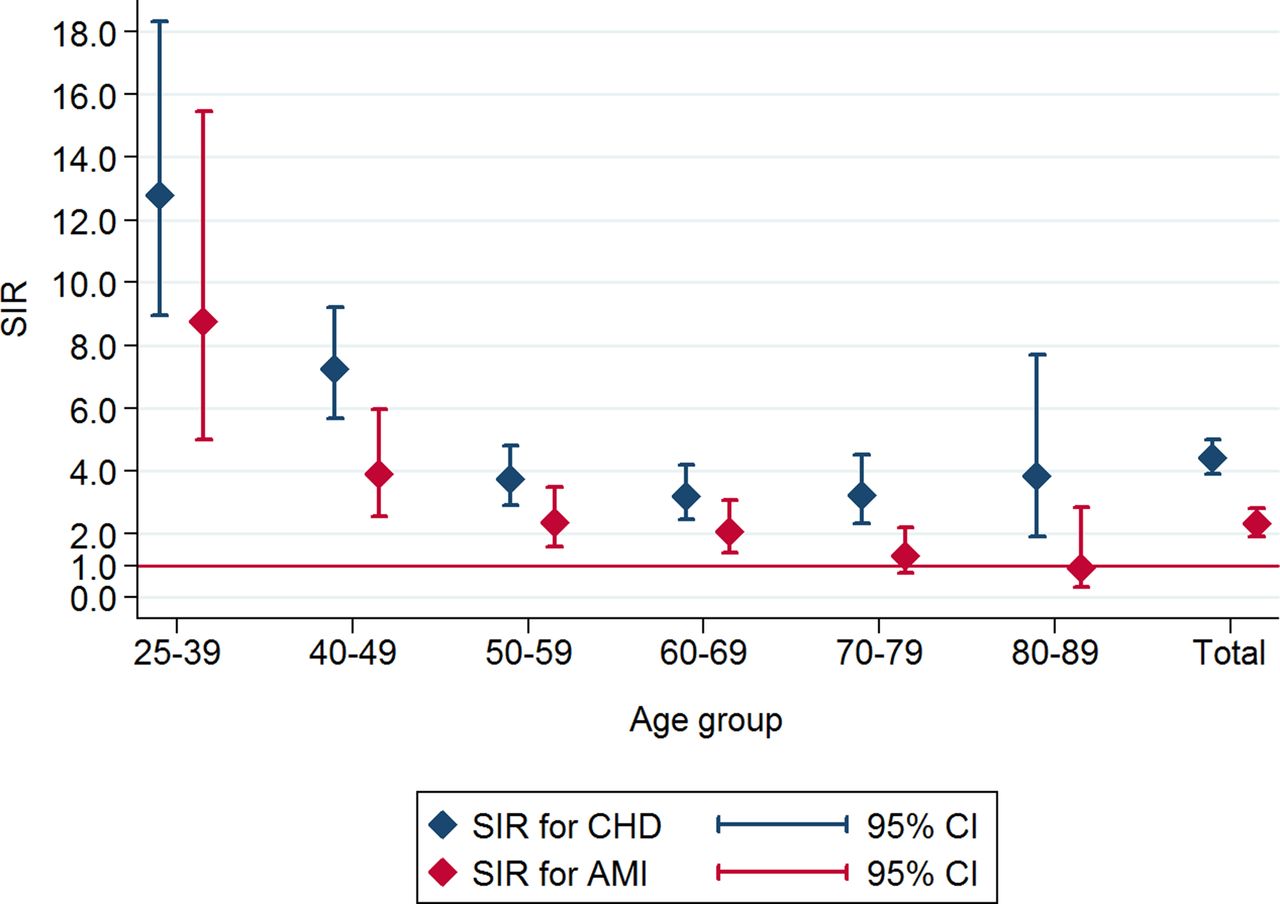
Standardised incidence ratios (SIRs) with 95% CIs for acute myocardial infarction (AMI) and coronary heart disease (CHD) in patients with familial hypercholesterolaemia during 2001–2009. Age-standardised and sex-standardised within each age group.
Mean (SD) time from inclusion in the UCCG Registry to the first AMI or CHD event were 5.9 (4.8) and 6.2 (5.0) years, respectively, suggesting a mean duration of lipid-lowering treatment prior to event of about 6 years.
Figure 2 displays the trends in SIRs according to sex and calendar period. For AMI, no significant trends over time were found (P=0.21 for both sexes combined, P=0.78 in men and P=0.08 in women). For CHD, there was a significant decrease over time for both sexes combined (P=0.03) and for men (P=0.02), but not for women (P=0.46).
The SIRs for PCI, CABG and total CR procedures were clearly higher in younger than in older patients as shown in tables 4, 5 and 6.

{kind=link}
{kind=link}
Trends in standardised incidence ratios (SIRs) for acute myocardial infarction (AMI) and coronary heart disease (CHD) in patients with familial hypercholesterolaemia during 2001–2009. (A) Trend in SIRs (95% CI) for CHD in men. (B) Trend in SIRs (95% CI) for CHD in women. (C) Trend in SIRs (95% CI) for CHD in both sexes. (D) Trend in SIRs (95% CI) for AMI in men. (E) Trend in SIRs (95% CI) for AMI in women. (F) Trend in SIRs (95% CI) for AMI in both sexes.
Percutaneous coronary intervention during 2001–2009
Coronary artery bypass grafting during 2001–2009
Total coronary revascularisation* during 2001–2009
Discussion
We observed an increased risk of AMI and CHD in FH compared with the general population. Importantly, the youngest age group had the highest excess risk in both sexes including the need for PCI, CABG and total CR. Both the Simone Broome Register Group and us have previously reported an increased risk for CHD death before the age of 40.13 28 As recently shown,14 our study show the severity of carrying an FH mutation in both sexes and particularly at young age.
We previously reported that 88% of the Norwegian patients with FH who died actually used statins at time of death but still with too high LDL-C.15 Statins were used by 89.1% of the Norwegian FH population as studied in 2006 (n=956),20 and it is reasonable to estimate that about 90% of the present study cohort used statins. Taken together with other recent studies, this emphasises the importance of early diagnosis and treatment in FH.29 30
During the observation period, SIR for CHD decreased slightly in men but not in women indicating a particular need to focus attention on the excess risk in young FH women. Statins were used for 6 years or more in those who experienced an event assuming that treatment was initiated at the time of genetic diagnosis. However, the mean age of genetic diagnosis was 32.7 years, unfortunately too late. A previous study reported a near normalisation of CHD risk in statin-treated patients older than 55 years, in fact they observed a risk of MI approaching that of the general population.17 Importantly, the present study add new information on the risk in young patients with FH. Any excess risk in young patients cannot be detected in a study of patients older than 55 years, and here we report a particularly high excess risk in patients with FH younger than 40 years.
We observed a significant reduction in the trend for CHD in patients with FH on top of the reduction in the general population (figure 2). However, trends in SIRs for CHD decreased only in men with FH, not women, suggesting that young women with FH need particular attention.
Strengths and limitations
Important strengths were the high number of genotyped patients with FH and the complete follow-up. All AMI and CHD hospitalisations and the corresponding reported deaths from the NCoDR for the entire Norwegian population during 2001–2009 were included. However, patients with FH who died before genetic testing were not registered.
Data on all hospitalisations in Norway were included in the analyses, but patients not hospitalised due to, for example, misdiagnoses were not included but there should be no difference between people with or without an FH mutation in this respect. Information on AMI subtypes is not available. Further, important factors that influence AMI morbidity and hospitalisation frequencies were not accounted for, that is, smoking habits, body mass index, LDL-C values, statin treatment, dietary habits or participation in coronary rehabilitation programmes after discharge. Patients were mainly Caucasian as 92.4% of the patients in the FH cohort are native Norwegians. Error rates in Patient Administrative Data (PAS) were, for AMI and stroke, previously reported to be 0.8% and 0.9% for time of admission, 4.7% and 4.9% for the main diagnosis, and 1.7% and 2.9% for index diagnosis, respectively.
Selection bias is important in register studies. Participants in the present study account for almost one-third of the total number of patients with FH in Norway, given a prevalence of 1:300. A large proportion of the total number reduce the possibility of any major selection bias. Further, most patients in the register were diagnosed by cascade screening due to family ties to an index patient. These patients are typically unaware of their FH prior to diagnosis, living normal lives without any special precautions further reducing the risk of any heavy selection bias in our cohort. Lastly, all physicians may request genetic testing of FH. Testing is free of charge for physicians and patients in Norway probably reducing the risk for bias due to economic issues.
In conclusion, Norwegian patients with FH have significantly higher incidences of AMI, CHD and related intervention procedures than the general population. This is true although statins are widely used. The youngest age group had the highest excess risk, underlining the need for early diagnosis and preventive treatment in FH.
Key messages
What is already known on this subject?
Familial hypercholesterolaemia (FH) leads to increased risk of coronary heart disease (CHD), but little data exist on the impact of age on the excess risk.
What does this study add?
A particularly high excess risk of CHD in young patients with FH was observed. The standardised incidence ratio (95% CI) for CHD was highest among patients 25–39 years old; 11.1 (7.1–17.5) and 17.3 (9.6–31.2) in men and women, respectively. In all age groups combined, standardised incidence ratio was 4.2 (3.6–5.0) in men and 4.7 (3.9–5.7) in women.
How might this impact on clinical practice?
The highest excess risk for cardiovascular disease was at age 25–39 years. More action is needed to find and treat patients with FH early in life.
Supplemental material
Supplemental material
Supplemental material
Acknowledgments
The authors thank Tomislav Dimoski at the Norwegian Knowledge Centre for Health Services, Oslo, Norway, for his contribution by developing software necessary for obtaining data from Norwegian hospitals, conducting the data collection and quality assurance of data in this project. We thank the patients for allowing us to study the data presented here and in particular Margaretha Hamrin who is the leader of the patient organisation for FH Norway (FH-Norge) for the important contribution in informing the Norwegian patient through the bi-annual FH-magazine (http://www.f-h.no/). We thank all referring physicians for many years of shipping samples for testing and we thank the staff at the UCCG and at the Lipid Clinic in Oslo for their effort over many years to generate the data presented here.
References
Footnotes
Contributors LJM, JI and KBH were responsible for the conceptual design of the study. LJM, JI, MBV, KBH, LO, RMS, TW, ISK, GST, TPL and KR were responsible for analysing and interpreting data. TPL was responsible for providing data from the UCCG registry. GST and JI were responsible for the CVDNOR data. LO, KBH and others contributed with blood samples from the Lipid Clinic. JI, MBV, RMS, ISK, TW and GST were responsible for the statistical analyses. LJM, KR and JI had the major responsibility of reviewing the study and input on revisions. All authors read and approved the final manuscript.
Funding This work was supported by the South-Eastern Norway Regional Health Authority, Oslo, Norway, Throne Holst Foundation for Nutrition Research, University of Oslo and Aktieselskabet Freia Chocolade Fabriks Medisinske Fond.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was performed in accordance with the Declaration of Helsinki and approved by the Regional Committee for Medical and Health Research Ethics, South-East Norway (case no. 2011/1343) and the Data Protection Official at Oslo University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The corresponding author has the right to grant on behalf of all authors, and does grant on behalf of all authors, an exclusive licence (or non-exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd and its Licensees to permit this article (if accepted) to be published in Heart editions and any other BMJPGL products to exploit all subsidiary rights.
Author note All participants signed an informed consent for genetic testing for diagnostic purpose. All participants received a letter with information that they could refuse their data to be linked to other registries. Those who refused were not included. The letter with information about the register linkage and the study as well as this procedure was approved by the local ethical committee prior to study start. This letter is uploaded as a supplementary file. The original language is Norwegian and it is uploaded in its original form; however, we will translate it if needed.