Article Text

Abstract
Introduction The clinical effectiveness of a ‘rule-out’ acute coronary syndrome (ACS) strategy for emergency department patients with chest pain, incorporating a single undetectable high-sensitivity cardiac troponin (hs-cTn) taken at presentation, together with a non-ischaemic ECG, remains unknown.
Methods A randomised controlled trial, across eight hospitals in the UK, aimed to establish the clinical effectiveness of an undetectable hs-cTn and ECG (limit of detection and ECG discharge (LoDED)) discharge strategy. Eligible adult patients presented with chest pain; the treating clinician intended to perform investigations to rule out an ACS; the initial ECG was non-ischaemic; and peak symptoms occurred <6 hours previously. Participants were randomised 1:1 to either the LoDED strategy or the usual rule-out strategy. The primary outcome was discharge from the hospital within 4 hours of arrival, without a major adverse cardiac event (MACE) within 30 days.
Results Between June 2018 and March 2019, 632 patients were randomised; 3 were later withdrawn. Of 629 patients (age 53.8 (SD 16.1) years, 41% women), 7% had a MACE within 30 days. For the LoDED strategy, 141 of 309 (46%) patients were discharged within 4 hours, without MACE within 30 days, and for usual care, 114 of 311 (37%); pooled adjusted OR 1.58 (95% CI 0.84 to 2.98). No patient with an initial undetectable hs-cTn had a MACE within 30 days.
Conclusion The LoDED strategy facilitates safe early discharge in >40% of patients with chest pain. Clinical effectiveness is variable when compared with existing rule-out strategies and influenced by wider system factors.
Trial registration number ISRCTN86184521.
- acute coronary syndromes
- acute myocardial infarction
- health care delivery
- health care economics
- quality and outcomes of care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- acute coronary syndromes
- acute myocardial infarction
- health care delivery
- health care economics
- quality and outcomes of care
Introduction
The number of patients attending emergency departments (EDs) worldwide continues to rise. Across England and Wales, there were over 23 million attendances in 2017–2018, a rise of over 20% in a decade.1 Chest pain makes up 6% of ED attendances in the UK and is the most common reason for emergency hospital admission.2 Many patients with chest pain have prolonged hospital stays during which they undergo testing to rule out acute myocardial infarction (AMI), yet 90% of patients are found to have a non-cardiac cause of chest pain.2 Prolonged assessment leads to increased costs and ED crowding.3
For patients with suspected cardiac chest pain, the diagnostic biomarker of choice is cardiac troponin, a marker of myocardial necrosis.4 High-sensitivity cardiac troponin (hs-cTn) assays have been developed, and very low concentrations can be measured.5 This has led to improved diagnostic accuracy earlier after chest pain onset and development of rapid ‘rule-out’ strategies for low-risk patients.6–15 These strategies have predominantly been evaluated within observational cohorts, and a lack of high-quality interventional trial data means that the potential of hs-cTn assays to improve clinical effectiveness in the rapid discharge of low-risk patients with chest pain admitted to the ED remains poorly understood.14
A rapid rule-out strategy incorporating a single undetectable (below the limit of detection (LoD)) hs-cTn taken at ED presentation, together with a normal ECG, has been extensively evaluated in observational studies.8–15 While this limit of detection and ECG discharge (LoDED) strategy maintains a high diagnostic accuracy for both AMI and major adverse cardiac events (MACEs), across populations, the proportion of patients actually discharged after a single blood test, and consequently its clinical and cost effectiveness, remains unknown.3 14 Due to concerns about reporting imprecision, the undetectable cut-off has not been approved for use by the US Food and Drug Administration,16 while in Europe, consensus guidelines include caveats to its clinical use. European Society of Cardiology (ESC) guidelines recommend that the undetectable cut-off is only used if blood sampling occurs more than 3 hours after chest pain onset, and UK National Institute of Health and Care Excellence guidelines suggests it should be confined to low-risk patients identified using a validated risk score.17 18 This may explain why around only 3% of hospitals within the UK use the undetectable cut-off in clinical practice.19
We aimed to determine whether the LoDED strategy, when used irrespective of chest pain onset time, without risk scores and across different hs-cTn assays, would increase the rate of safe early discharge from hospital in patients with suspected cardiac chest pain, when embedded within routine ED practice, and without an increase in healthcare costs.
Methods
Study design and participants
The LoDED strategy versus usual care in adult patients with chest pain attending the ED trial was a prospective randomised open label blinded endpoint parallel group trial that aimed to assess the clinical effectiveness of the LoDED strategy in adult patients presenting to the ED with suspected cardiac chest pain in eight secondary and tertiary hospitals across England and Wales. Patients were eligible for recruitment if they were aged ≥18 years; presented to the ED with chest pain and triggered a suspected cardiac chest pain investigation pathway (ie, the treating clinician intended to perform investigations to rule out an acute coronary syndrome); had a non-ischaemic ECG (no new T-wave inversion of >3 mm or ST depression of >1 mm as judged by the treating clinician); and peak symptoms occurred <6 hours prior to ED presentation. Exclusion criteria are described in the published trial protocol and included in the Consolidated Standards of Reporting Trials (CONSORT) diagram (figure 1).20

ConsolidatedStandards of Reporting Trials diagram. ACS, acute coronary syndrome; LoD, limit of detection; LoDED, limit of detection and ECG discharge.
Randomisation and blinding
Patients were randomised to evaluation with either the LoDED strategy (intervention) or the usual rule-out strategy in that site (control) in a 1:1 ratio, before initial hs-cTn results were known to the treating clinician. Randomisation was undertaken through a web-based portal, stratified by site and minimised by age and sex.
Procedures
Cardiac troponin testing and measurement
All participants had a blood sample taken for hs-cTn measurement at, or shortly after, ED arrival as part of their standard clinical assessment. Where repeat hs-cTn sampling was required, this was undertaken according to local guidelines (table 1) and not controlled for trial purposes.
Summary of usual rule-out strategies (control) by site
Clinical blood samples were analysed, in real-time, locally in central hospital laboratories for either the Roche Elecsys high-sensitivity cardiac troponin T (hs-cTnT) assay, Abbott Architect high-sensitivity cardiac troponin I (hs-cTnI) or Beckman Coulter Access hs-cTnI (further assay details in table 1).
Trial interventions
LoDED Strategy (intervention)
Participants randomised to the LoDED strategy were eligible for discharge if their ECG was non-ischaemic; a single hs-cTn test taken at presentation (and irrespective of the symptom onset time) was undetectable for the assay used at that study site; and there was no ongoing clinical concern. Any participant not fulfilling these discharge criteria reverted to the usual rule-out strategy at that study site.
Usual rule-out strategies (control)
Table 1 summarises the usual rule-out strategies in use across the eight sites. No sites used identical strategies; this heterogeneity accords with the findings of a cross-sectional survey of English hospitals and therefore reflects current practice.19
Clinical management, data collection and follow-up processes are detailed in the supplementary material and in the published protocol.20
Outcomes
The primary outcome was successful early discharge, defined as discharge from hospital within 4 hours of ED arrival, without a MACE occurring within 30 days. A time point was chosen for the primary outcome, rather than admission/discharge rate, because hospital admission is defined differently in different hospitals. This approach has been used in previous randomised trials evaluating the clinical effectiveness of rule-out strategies.7 21 The time point of 4 hours was selected to reflect the NHS 4-hour ED standard. Such targets have been used internationally to provide an impetus to manage patients in a timely manner in an emergency setting.1 The safety endpoint of MACE occurring within 30 days was defined as cardiac death, type I AMI or emergency revascularisation occurring within 30 days of ED attendance (including the index presentation). Type I AMI was defined according to the Fourth Universal definition (a rise and/or fall of troponin above the 99th percentile).4 A significant rise and/or fall was defined as an absolute change in troponin over time of at least half the 99th percentile value of the assay in use.22 Primary outcomes were adjudicated by an independent expert panel comprising a senior emergency physician and cardiologist blinded to both participants’ allocated groups and initial hs-cTn results. Secondary outcomes are listed in the supplement.
Statistical analysis
The statistical and health economic analysis are described in detail in the supplementary material. Briefly, for the statistical analysis of the primary outcome, an intention-to-diagnose logistic regression analysis, adjusting for age and sex using all those randomised with complete data, was conducted by centre. As expected, usual care pathways differed between sites, and the proportion of patients discharged within 4 hours varied, which influenced observed treatment effects at each centre. Meta-analysis methodology was used to produce an overall OR and between-centre heterogeneity examined using the Q and I2 statistic. Potential reasons for heterogeneity were investigated further for sites with and without the undetectable cut-off in usual care and by hs-cTn assay type. Kaplan-Meier-type graphs illustrate the relationship between length of hospital stay.
Sample size
The target sample size was based on both observational and interventional data.7 13–15 For the overall population, we anticipated 8% of participants would be discharged within 4 hours using usual care and at least 17% using the LoDED strategy. Therefore, the trial was powered to detect a 9% difference between early discharge rates with 90% power and two-sided alpha of 0.05. This required 282 patients in each group with primary outcome data. Allowing for a 95% follow-up rate, a total recruitment target of 594 participants was set.
Patient and public involvement
Patient and public involvement occurred at all stages of trial design and conduct. A patient advisory group (PAG) oversaw development and approval of patient-facing materials. The PAG supported the interpretation of results and approved the final manuscript submission.
Results
In total, 632 patients were randomised between 4 June 2018 and 4 March 2019. Three patients were later withdrawn; one had no record of consent and two were randomised in error. All remaining 629 patients were successfully monitored for 30 days. A total of 316 patients were allocated to the LoDED strategy and 313 to usual care (figure 1). The baseline characteristics were well balanced between groups (table 2). The cohort was predominantly men (59%), of white British ethnicity (88%), with a mean age of 53.8 years, and were at low risk of cardiac disease. Patients presented at a median of 2.3 hours (IQR 1.5–3.6 hours) after chest pain onset and the first hs-cTn sample was drawn at a median of 3.3 hours (IQR 2.3–4.5) after chest pain onset. Of the 629 patients, 42 (7%) had a MACE within 30 days (table 3).
Patient demographics and risk characteristics
Clinical outcomes and comparative costs
Supplemental material
Primary outcome
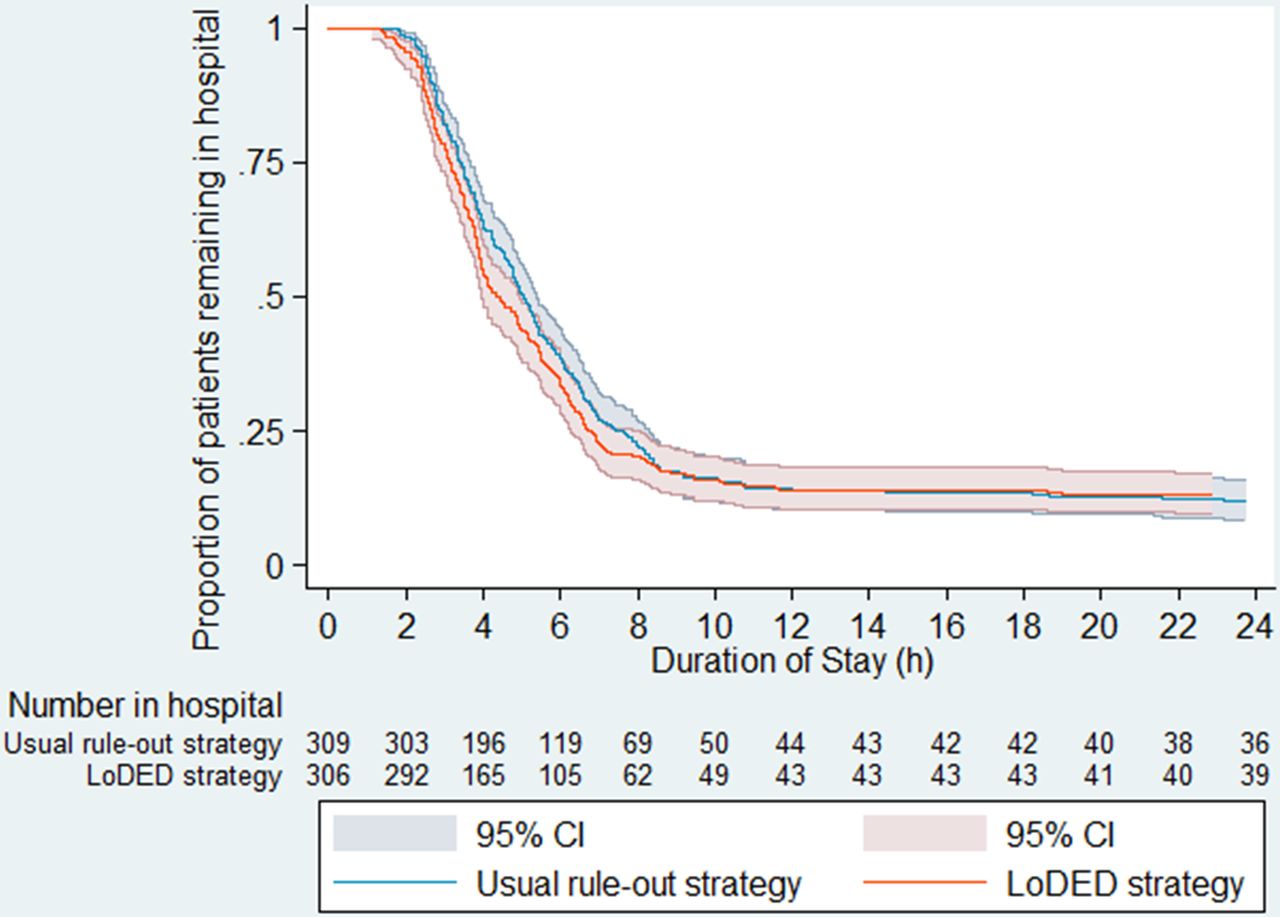
Data were available for the primary outcome in 620/629 patients. Discharge time was not recorded for 14 patients, but for five of these, their length of stay was over 4 hours. When allocated to the LoDED strategy, 141 of 309 (46%) were discharged within 4 hours of arrival, without subsequent 30-day MACE, and for usual rule-out strategies, 114 of 311 (37%) (table 3); pooled OR 1.58 (95% CI 0.84 to 2.98). The Kaplan-Meier-type length of stay curve illustrates improved discharge rates using the LoDED strategy, which persisted until 8 hours after patient arrival (figure 2).

Kaplan-Meier-type length of stay curve by group allocation (intention to treat). LoDED, limit of detection and ECG discharge.
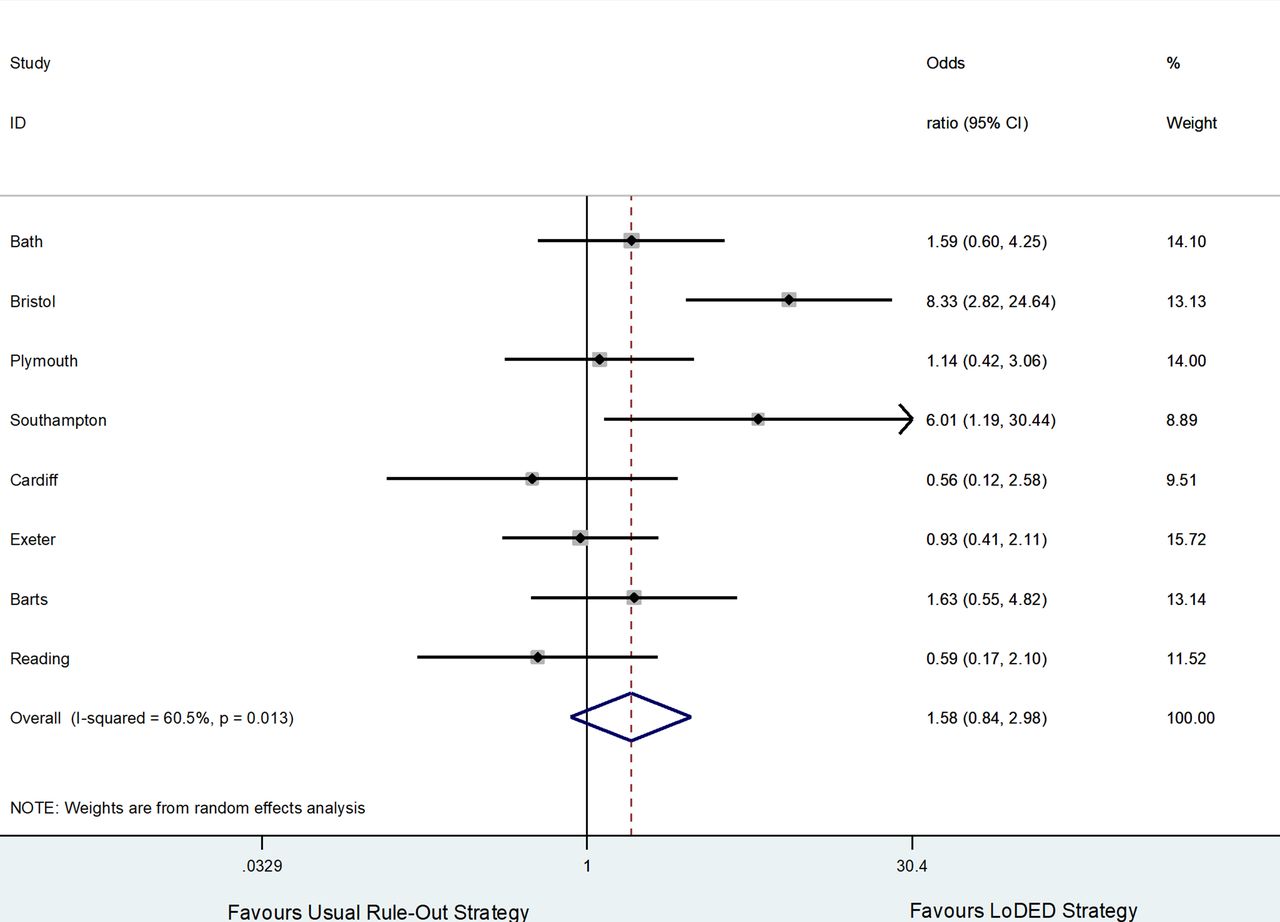
Figure 3 demonstrates significant heterogeneity between sites for the primary outcome (I2=61%, p=0.01 for Q test of heterogeneity), which was only partially explained by the control rule-out strategies in use. For sites using the undetectable cut-off within usual care, the pooled OR was 0.93 (95% CI 0.54 to 1.59, I2=0.0%, p=0.58 for Q test). For sites not using the undetectable cut-off within usual care, the pooled OR for the primary outcome was 2.87 (95% CI 1.07 to 7.69, I2=67%, p=0.03 for Q test). This positive treatment effect was driven by only two sites, Bristol (OR 8.33, 95% CI 2.82 to 24.64) and Southampton (OR 6.01, 95% CI 1.19 to 30.44), with no effect seen in the remaining two sites not using the LoD within usual care, Bath (OR 1.59, 95% CI 0.60 to 4.25) and Plymouth (OR 1.14, 95% CI 0.42 to 3.06). Kaplan-Meier-type length of stay curves for each site are included in online supplementary figures 1–8. Clinical outcomes by group allocation and site are shown in table 3. A subgroup analysis of patients with an initial undetectable hs-cTn is detailed in figure 4 and in the online supplementary material. Resource use data are described in table 4, together with mean per-patient costs by category. Comparative costs are described in detail in the online supplementary material.
Total resource use and mean per-patient costs by category
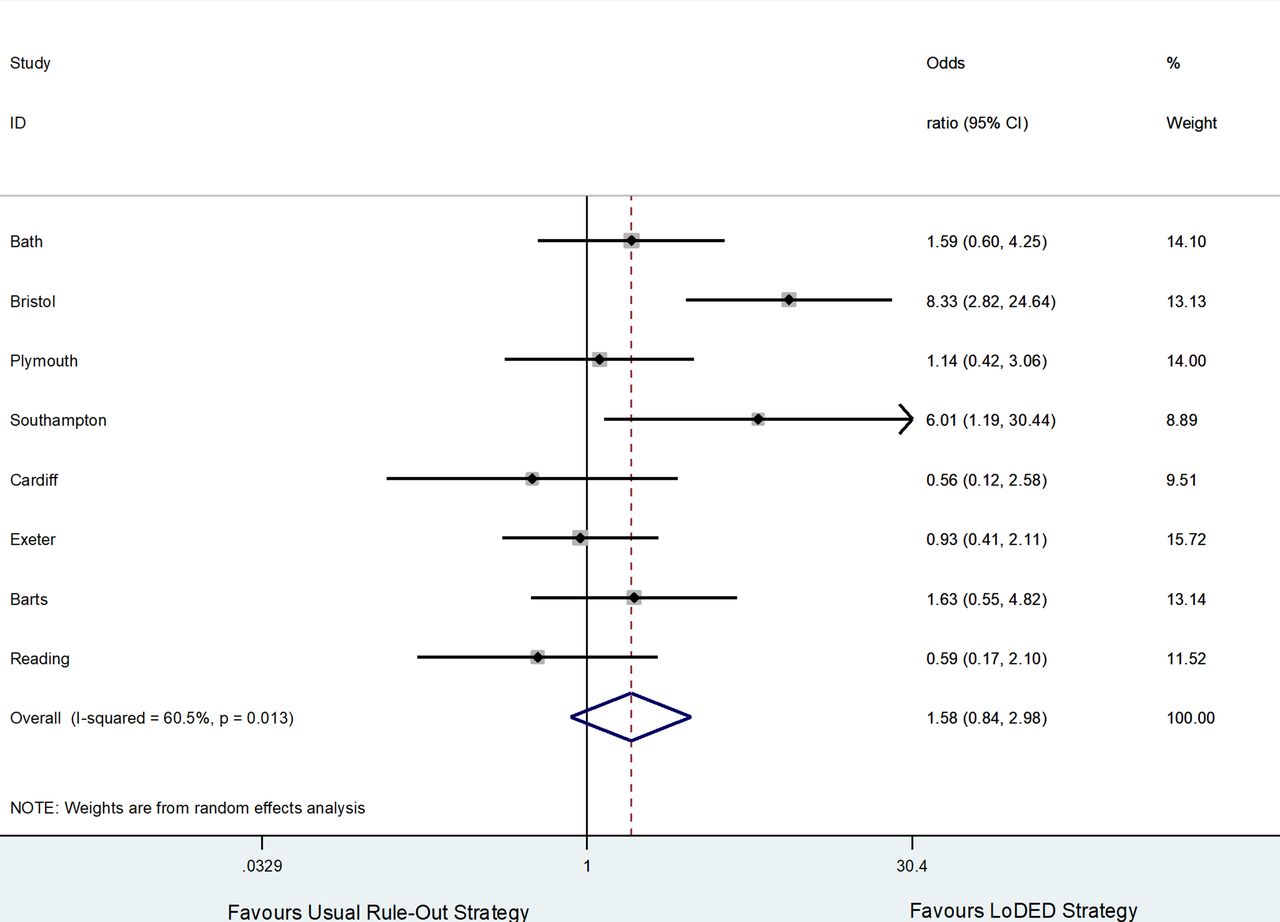
Forest plot for the primary outcome of successful early discharge. LoDED, limit of detection and ECG discharge.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier-type length of stay curve for patients with an initial high-sensitivity cardiac troponin below the limit of detection. LoDED, limit of detection and ECG discharge.
Acceptability and adherence to the LoDED strategy
Interviews with 11 patients from four sites and two focus groups with 20 ED professionals and general practitioners were conducted. From the qualitative interviews, patients were not anxious about the new strategy, trusted the clinicians’ judgement and welcomed the opportunity to be discharged sooner. Clinicians were more sceptical about discharging patients early in case they missed something and awaited the trial results to reassure them that there were no adverse consequences of discharging patients sooner (a full qualitative report has been submitted for publication and is available on request to the authors). Despite this finding, 88% (95%CI 81% to 93%) of patients allocated to the LoDED strategy who had an initial hs-cTn below the LoD were discharged from hospital in accordance with the strategy.
Discussion
We evaluated whether the use of a rapid rule-out strategy based on a single undetectable hs-cTn test taken on arrival at the ED (irrespective of chest pain onset time), together with a normal ECG (the LoDED strategy), increased the rate of safe, early discharge. When embedded within existing rule-out strategies in use across eight sites, the LoDED strategy facilitated discharge within 4 hours in over 40% of all patients and, importantly, no patient discharged with an initial undetectable hs-cTn had a MACE before 30 days. This accords with findings from multiple observational studies that the LoDED strategy is safe and provides clinicians with an opportunity to discharge low-risk patients based on a single undetectable hs-cTn result.8–15 However, when compared with existing rule-out strategies which use hs-cTn assays as recommended by consensus guidelines,19 20 the LoDED strategy did not show a difference in the rate of safe early discharge, even in those patients with an initial undetectable hs-cTn. There was also no difference in healthcare costs between the two strategies.
There are a number of potential explanations for these findings. First, the proportion of patients discharged within 4 hours across control strategies (37%) was much greater than the 8% estimated in our power calculation, which was based on an interventional study of a testing strategy of 0 and 2 hours undertaken 5 years prior to designing this trial (the primary outcome for that trial was successful discharge within 6-hour of arrival; data on 4-hour discharge rates were provided through personal communication with the trial statistician).7 This may reflect an improved clinical understanding of the use of rapid rule-out strategies to facilitate early discharge and subsequent guideline recommendations that the undetectable cut-off can be used in clinical practice, although with caveats.17 18 Contamination, whereby clinicians simply applied the LoDED strategy to those patients allocated to usual care, is also possible. Second, we observed considerable heterogeneity between sites, with some sites demonstrating a potential for reduced effectiveness of the intervention strategy compared with usual care. We demonstrated improvements in the primary outcome at some sites where the undetectable cut-off was not already in use, as per guideline recommendations. However, even when accounting for these control strategy differences, significant heterogeneity remained. This is an important finding and may reflect local culture, in terms of which patients are selected for rule-out testing, and the high clinical intensity of the ED, which are beyond the rule-out strategy itself. Third, we undertook this study, in which discharge within 4 hours was a component of the primary outcome, during a time period when performance against the 4-hour standard for all ED patients has been at its worst for a decade.1 Given that we observed separation on the Kaplan-Meier-type length of stay curves between usual care and the LoDED strategy up to 8 hours after ED attendance, our findings may reflect poor performance against this standard, rather than performance of the rule-out strategy itself.
Despite being available for nearly a decade, there are very few interventional trials evaluating the clinical effectiveness or cost-effectiveness of hs-cTn assays in the rapid discharge of patients with chest pain admitted to the ED. One randomised controlled trial of over 3000 participants evaluating the ESC-recommended Roche hs-cTnT assay of 0 and 1 hour, rule-out strategy demonstrated improved clinical effectiveness in terms of rapid discharge from the ED, but compared this strategy to a control group where contemporary cut-offs were used, which may have inflated the results.23
Our trial has several strengths that distinguish it from prior studies and extend the generalisability of the findings. First, we tested a strategy that does not rely on a risk score. Numerous risk scores such as thrombolysis in myocardial infarction, history, ECG, age, risk factors, troponin and troponin-only Manchester acute coronary syndromes have been evaluated and shown promise in observational studies.24 25 However, when tested within interventional trials, poor adherence by clinicians has limited their clinical effectiveness when applied to practice.7 26 Our results demonstrate good adherence to the LoDED strategy, suggesting clinicians would be willing to follow its recommendations when used in routine care. Second, one of the remaining controversies in the use of the undetectable cut-off is in patients who present early after chest pain onset.14 By excluding patients who presented over 6 hours from chest pain onset, we have tested the LoDED strategy in a population where around 45% of patients had their first sample drawn within 3 hours of chest pain onset. Given there were no 30-day MACEs in patients with an initial undetectable troponin in either arm of the trial, this provides reassurance to clinicians that the LoDED strategy can be used irrespective of chest pain onset time. However, clinical judgement should be used to ascertain the need for serial testing in very early presenters. Third, previous trials have tested hs-cTn assays provided by a single manufacturer.23 This approach can have significant limitations in terms of generalisability because hospitals may have limited opportunity to change assays. By applying the LoDED strategy across the three different troponin assays in which the undetectable cut-off has been evaluated in observational studies, we have enhanced the generalisability of our findings.8–15
Other study limitations include a trial design that assessed the clinical effectiveness of the LoDED strategy, rather than comparing safety between the intervention and control arms. It is possible that some patients discharged according to the LoDED strategy may have developed a subsequent subclinical rise in troponin after discharge. It is known that hs-cTn elevations above the undetectable cut-off may have prognostic implications when follow-up periods are extended beyond a year.27 Prognostic implications have not been addressed in our trial. Finally, despite randomising participants prior to hs-cTn results being known, the population demographics suggest this is a low-risk chest pain population. We excluded patients with ischaemic ECG findings, which may explain the low-risk demographics. However, the trial sample had lower-risk demographics than an unselected observational study, which applied the same ECG exclusion criteria.8 Therefore, it is possible that a degree of patient selection occurred, and the study findings can only be applied to patients with chest pain deemed low risk by treating clinicians.
We have shown that a rule-out strategy based on an initial undetectable hs-cTn test, normal ECG and no ongoing clinical concern (LoDED), facilitates the safe early discharge of over 40% of patients with chest pain, without an increase in healthcare costs. However, the clinical effectiveness of such a strategy is limited when compared with existing rule-out strategies, especially those that already incorporate the undetectable cut-off. In addition, the clinical effectiveness of early rule-out strategies is likely to be undermined by a range of system factors such as prolonged ED waiting times and crowding.
Key messages
What is already known on this subject?
Numerous cohort studies, systematic reviews and meta-analyses suggest that patients with an undetectable high-sensitivity cardiac troponin (hs-cTn) concentration at presentation to the emergency department (ED) are at low-risk of 30-day major adverse cardiac events. This finding has been repeated across different troponin assays. However, a lack of interventional trial data means that the clinical effectiveness of embedding this rule-out strategy within routine practice is unknown.
What might this study add?
Although the limit of detection (LoD) strategy facilitated the safe early discharge of over 40% of low-risk patients with chest pain, clinical effectiveness was not statistically different from usual care strategies that already incorporate high-sensitivity troponin tests. This finding brings into question existing observational evidence and may, in part, be due to factors beyond the strategy itself, such as the high clinical intensity of the ED, which has an important effect on the ability of clinicians to facilitate early discharge.
How might this impact on clinical practice?
The LoD strategy is safe and provides clinicians with an opportunity to discharge low-risk patients based on a single undetectable hs-cTn result taken at presentation to the ED. However, clinicians should be mindful of the importance of clinical judgement in patients presenting early after chest pain onset, and in some centres the strategy may not lead to improved clinical effectiveness. Long-term prognostic implications of this strategy have not been addressed in this trial.
Supplemental material
Supplemental material
Acknowledgments
The British Heart Foundation assisted in providing an independent patient and public representative for the Trial Steering Committee. The Peninsula Clinical Trials Unit at the University of Plymouth provided support with the design, management and logistics of the trial. We thank the following individuals for their support during the conduct of the trial: Gareth Williams (Swansea), patient and public involvement lead; Jamie Milton, Gay and Adrian Sawyer (Bristol), members of the patients advisory group; Saif Al-Nahas, local principal investigator, Royal Unit Hospital, Bath, UK; Tim Rainer and Nick Manville, local principal investigators, University Hospital of Wales, Cardiff, UK; Manish Thakker, local principal investigator, Royal Berkshire Hospital, Reading, UK; Sanjay Ramamoorthy, local principal investigator, University Hospital Southampton, UK; Ben Bloom, Royal London Hospital, Barts Health NHS Trust, London; Research nursing staff at all sites, who ensured recruitment to time and target; Richard Body, independent emergency physician and chair of the Trial Steering Committee (TSC); James Gamble, independent cardiologist on the TSC; Sean Ewings, independent statistician on the TSC; Sarah Miles, patient representative on the TSC; Eva Sammut, cardiologist, Outcome Adjudication Committee; Anne Frampton, emergency physician, Outcome Adjudication Committee.
References
Footnotes
Twitter @eddcarlton
Correction notice Since the online publication of this article, the provenance and peer review statement has been updated to show that this article was externally peer reviewed.
Contributors EWC conceived the idea for the study. EWC, JK, AR, JES and JRB were responsible for the initial study design, which was refined with the help of RK, JI and HT and support from our regional National Institute for Health Research Research Design Service. Expert advice on cardiological and biochemical elements of the study design was provided by SA and PB, respectively. HT provided the statistical plan and undertook data analysis. RK led the economic study and provided oversight to JG, who undertook the resource and cost analyses. JI developed the integrated qualitative study, with support from LB, and supported the public and patient views in the study development. SCa and RC coordinated the study set-up and finalisation of the study protocol as senior trial manager and assistant trial manager, with oversight from SCr, director of the Peninsula Clinical Trials Unit. All authors contributed to the final study design and protocol development, critically revised successive drafts of the manuscript and approved the final version. The trial management group was responsible for the conduct of the study, overseen by the Trial Steering Committee.
Funding This trial was funded by the National Institute for Health Research (NIHR) through its Research for Patient Benefit programme (grant reference number PB-PG-0416-20012). JRB is an NIHR senior investigator.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Competing interests EC has received funding from Abbott Diagnostics for related research and honoraria for education from Roche.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval The study was approved by the South West Frenchay Research Ethics Committee (REC reference 18/SW/0038) and each of the participating NHS Trust’s Research and Development department. All patients provided written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Summary data collected from the study, including de-identified patient level data, can be made available upon request to the corresponding author.