Article Text

Abstract
Objective Previous studies that evaluated cardiovascular risk factors considered age as a potential confounder. We aimed to investigate the impact of cardiovascular disease (CVD) and its risk factors on fatal outcomes according to age in patients with COVID-19.
Methods A systematic literature review and meta-analysis was performed on data collected from PubMed and Embase databases up to 11 June 2020. All observational studies (case series or cohort studies) that assessed in-hospital patients were included, except those involving the paediatric population. Prevalence rates of comorbid diseases and clinical outcomes were stratified by mean patient age in each study (ranges: <50 years, 50–60 years and ≥60 years). The primary outcome measure was a composite fatal outcome of severe COVID-19 or death.
Results We included 51 studies with a total of 48 317 patients with confirmed COVID-19 infection. Overall, the relative risk of developing severe COVID-19 or death was significantly higher in patients with risk factors for CVD (hypertension: OR 2.50, 95% CI 2.15 to 2.90; diabetes: 2.25, 95% CI 1.89 to 2.69) and CVD (3.11, 95% 2.55 to 3.79). Younger patients had a lower prevalence of hypertension, diabetes and CVD compared with older patients; however, the relative risk of fatal outcomes was higher among the former.
Conclusions The results of the meta-analysis suggest that CVD and its risk factors (hypertension and diabetes) were closely related to fatal outcomes in COVID-19 for patients across all ages. Although young patients had lower prevalence rates of cardiovascular comorbidities than elderly patients, relative risk of fatal outcome in young patients with hypertension, diabetes and CVD was higher than in elderly patients.
Prospero registration number CRD42020198152.
- meta-analysis
- cardiac risk factors and prevention
- quality and outcomes of care
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
COVID-19 is caused by a novel beta-coronavirus believed to have originated in Wuhan, China, in December 2019, before it spread worldwide. The virus was named SARS-CoV-2, and subsequently, the WHO declared the outbreak as a public emergency of international concern.1 Unfortunately, the number of deaths and confirmed cases of COVID-19 are rising steadily despite efforts by global healthcare providers to keep the disease under control. As of 21 June 2020, the total number of confirmed cases was approximately 8.7 million, with 463 281 deaths in 188 countries.2 Studies have reported that a considerable number of patients with COVID-19 have an underlying disease.3 4 Cardiovascular diseases (CVDs) are known to be triggered by acute respiratory infections caused by viruses (eg, influenza and respiratory syncytial virus) or bacteria.5 6 The presence of underlying CVD is often linked with other comorbidities that predispose patients to more frequent and severe forms of infection.7
During outbreaks of influenza, several infected patients have reportedly died due to complications of comorbid CVDs than due to secondary bacterial pneumonia.8 Furthermore, the presence of underlying CVD increases both the severity of the primary respiratory disease and the risk of developing further complications.9 It has been reported that the major risk factors for mortality in patients with COVID-19 include age greater than 60 years, male sex and the presence of comorbidities.3 However, previous studies that evaluated these risk factors considered age as a potential confounder. Although some studies have demonstrated that hypertension is a risk factor for developing severe COVID-19, the observation could be attributed to the higher prevalence of comorbidities in elderly patients.10 To the best of our knowledge, no study has investigated the association between the presence of risk factors for CVD and outcomes of patients with COVID-19 depending on age. Therefore, we conducted a systematic review and meta-analysis to estimate the prevalence and risk factors for CVD among patients with COVID-19 in different age groups.
The primary hypothesis of this review was that, in patients with both COVID-19 infection and risk factors for CVD, elderly individuals would have fatal outcomes, while younger patients would show better prognosis.
Methods
Research protocol
The present study was registered with PROSPERO (ID: CRD42020198152). This study was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analyses guidelines (figure 1). Literature search was performed using the PubMed and Embase search engines until 11 June 2020, using the following medical subject headings both alone and in different combinations: “COVID-19”, “SARS-CoV-2”, “comorbidity”, “prevalence”, “characteristic”, “observational”, “hypertension”, diabetes” and “cardiovascular disease” without any language restrictions. Major medical journals were also searched manually; we also searched for studies cited as references in relevant research articles in addition to systematic reviews of published, unpublished and ongoing studies (medRxiv, Research Square and Lancet preprint database). All observational studies (case series or cohort studies) conducted on in-hospital patients were included. The exclusion criteria comprised studies: (1) on paediatric populations (age 17 years or younger), (2) that did not include information on clinical outcomes, (3) that investigated the same cohort, (4) that only included mortality cases and (5) that did not have description on age of the patients.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart.
Each abstract or title based on results of the electronic search was screened by pairs of independent reviewers (SAB, S-MP, SRK and M-NK); full articles of potentially eligible studies were acquired and assessed by these reviewers, who then selected the studies to be included in our review. Discrepancies between the reviewers were resolved through discussion. If a consensus could not be reached, another reviewer (WJS) was consulted to resolve the disagreement.
Data extraction and assessment of study quality
Using a piloted form, we collected data on patient characteristics, study quality and clinical outcomes in patients with laboratory-confirmed COVID-19, indicated by a positive SARS-CoV-2-RT-PCR test. The definition of hypertension or diabetes used in this meta-analysis was history (comorbidity) of hypertension or diabetes. The definition of CVD used in this meta-analysis was history of CVD and its synonyms such as coronary artery disease or cardiac disease. The primary outcome measure was a composite fatal outcome of severe COVID-19 or death. Severe COVID-19 was defined as the presence of respiratory distress (respiratory distress (30 breaths or more per min), oxygen saturation of ≤93% at rest, PaO2/FiO2 ratio of 300 mm Hg) or the need for ICU care (respiratory failure requiring mechanical ventilation, shock and/or multiorgan failure).11
The overall quality of each study was assessed using the Newcastle-Ottawa Quality Assessment Scale (NOS).12 The NOS score for cohort studies ranges between 0 and 9, and a score greater than seven indicates high quality.
Statistical analysis
Wherever possible, prevalence rates and clinical outcomes were stratified by mean age for each study (range: <50 years, 50–60 years and ≥60 years). The mean age of the patients was calculated if the information was not presented directly in a study.13 Forest plots of point estimates, including their 95% CI range, were used for graphical analysis. For the meta-analysis, pooled logistic regression with inverse-variance weighting was used for each study, and summary estimates were exponentiated. Estimates are expressed as ORs with 95% CI. A random-effects model was used considering the heterogeneity of patient characteristics and differences in the number of patients between studies. Sensitivity analysis was conducted by omitting one study at a time and evaluating the effect on the pooled results to analyse the extent of heterogeneity among the selected studies. The I2 statistic was then used to evaluate heterogeneity among the studies; a value of 75% or greater indicated high heterogeneity.14 A meta-regression model was constructed considering the risk of clinical outcomes as the dependent variable to demonstrate our hypothesis regarding the effects of age. Small-study effect or publication bias was assessed using funnel plots, Egger’s test, Begg’s test and sensitivity analysis based on study size. In the event of significant publication bias, adjusted publication bias was performed by the trim-and-fill method (Duval and Tweedie non-parametric method).15 A p value <0.05 indicated evidence of bias. All data analyses were conducted using R software V.3.5.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study characteristics
The online literature search identified 6,560 studies. Three additional studies were identified by manual search (figure 1). Review of all studies until 11 June 2020 was performed, and 51 studies were considered eligible for analysis, with a total of 48,317 patients with COVID-19. All studies were observational (10 prospective and 41 retrospective). Thirty-seven studies were from China (patients, n=13,273), seven from the USA (n=14,925), six from Italy (n=2,927), and three each from the UK and Iran. The median age of the patients was 56 years, and 58.1% were men (online supplemental table 2).
Supplemental material
Hypertension
The overall prevalence of hypertension in all the studies was 26.19% (95% CI 21.76 to 31.16) and was found to increase with age, wherein 15.57%, 26.81% and 46.95% of the patients aged <50 years, 50–60 years and ≥60 years, respectively, were found to have the condition (figure 2A, online supplemental figure 1). Meta-analysis showed that comorbid hypertension conferred a high risk of developing severe COVID-19 (35.7% vs 20.3%, OR 2.42, 95% CI 1.98 to 2.96), death (26.1% vs 9.4%, OR 2.60, 95% CI 2.11 to 3.20) and overall fatal outcomes in patients across all age groups (31.0% vs 13.8%, OR 2.50, 95% CI 2.15 to 2.90) (figure 2B, online supplemental figures 2–5). However, patients younger than 50 years of age had a higher risk of developing fatal outcomes (22.9% vs 10.3%, OR 3.49, 95% CI 2.49 to 4.88) compared with those older than 60 years (34.7% vs 21.3%, OR 1.86, 95% CI 1.55 to 2.23).

Prevalence of hypertension and clinical outcomes by age.
Diabetes
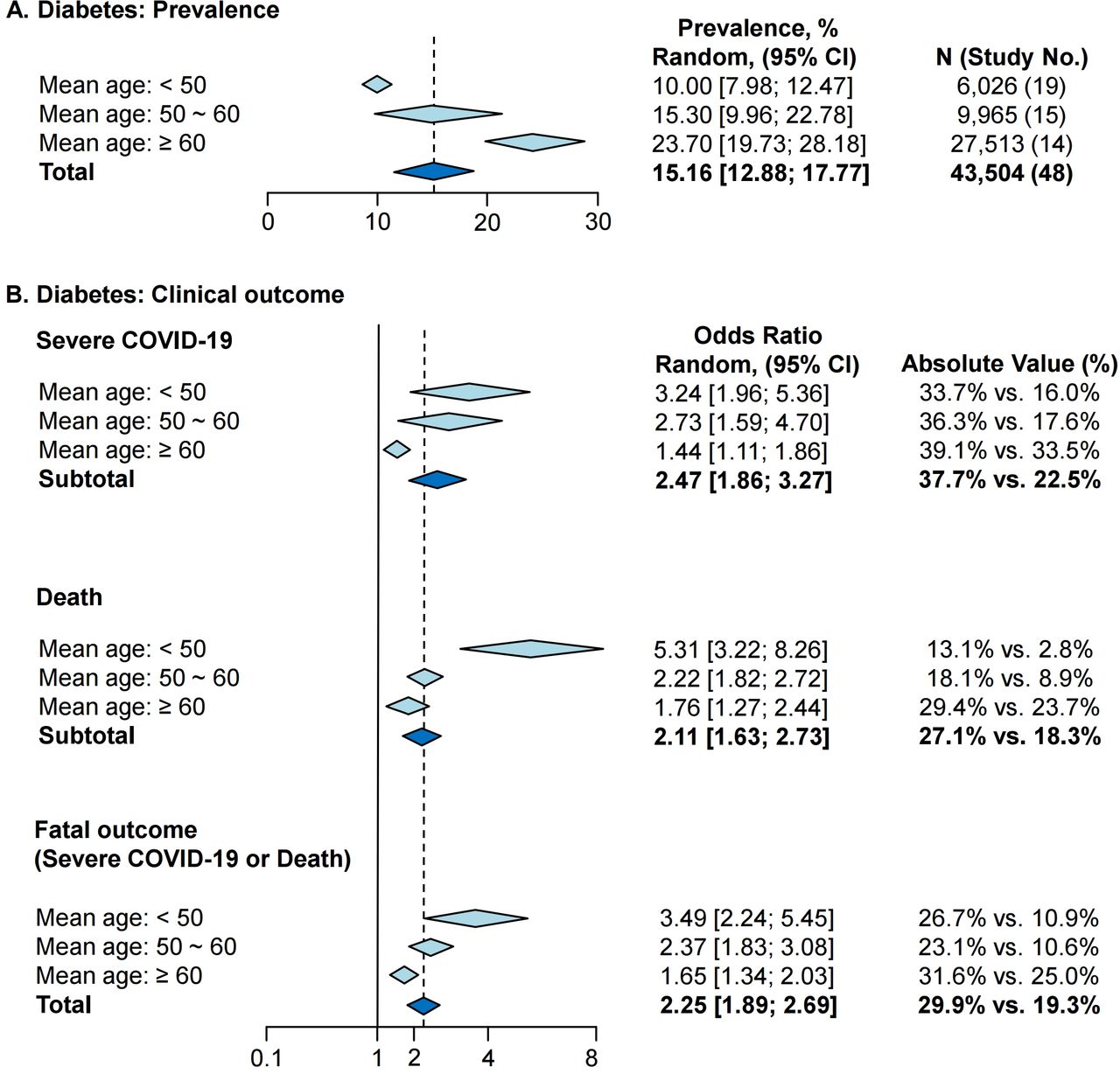
The overall prevalence of diabetes in 48 studies was 15.16% (95% CI 12.88 to 17.77) and was found to increase with age, wherein 10.0%, 15.3% and 23.7% of the patients aged <50 years, 50–60 years and ≥60 years, respectively, suffered from the condition (figure 3A, online supplemental figure 6). Meta-analysis showed that the presence of diabetes conferred a high risk of developing severe COVID-19 (37.7% vs 22.5%, OR 2.47, 95% CI 1.86 to 3.27), death (27.1% vs 18.3%, OR 2.11, 95% CI 1.63 to 2.73) and fatal outcomes in patients across all age groups (29.9% vs 19.3%, OR 2.25, 95% CI 1.89 to 2.69) (figure 3B, online supplemental figures 7–10). However, patients younger than 50 years of age had a higher risk of developing fatal outcomes (26.7% vs 10.9%, OR 3.49, 95% CI, 2.24 to 5.45) than those older than 60 years (31.6% vs 25.0%, OR 1.65, 95% CI 1.34 to 2.03).
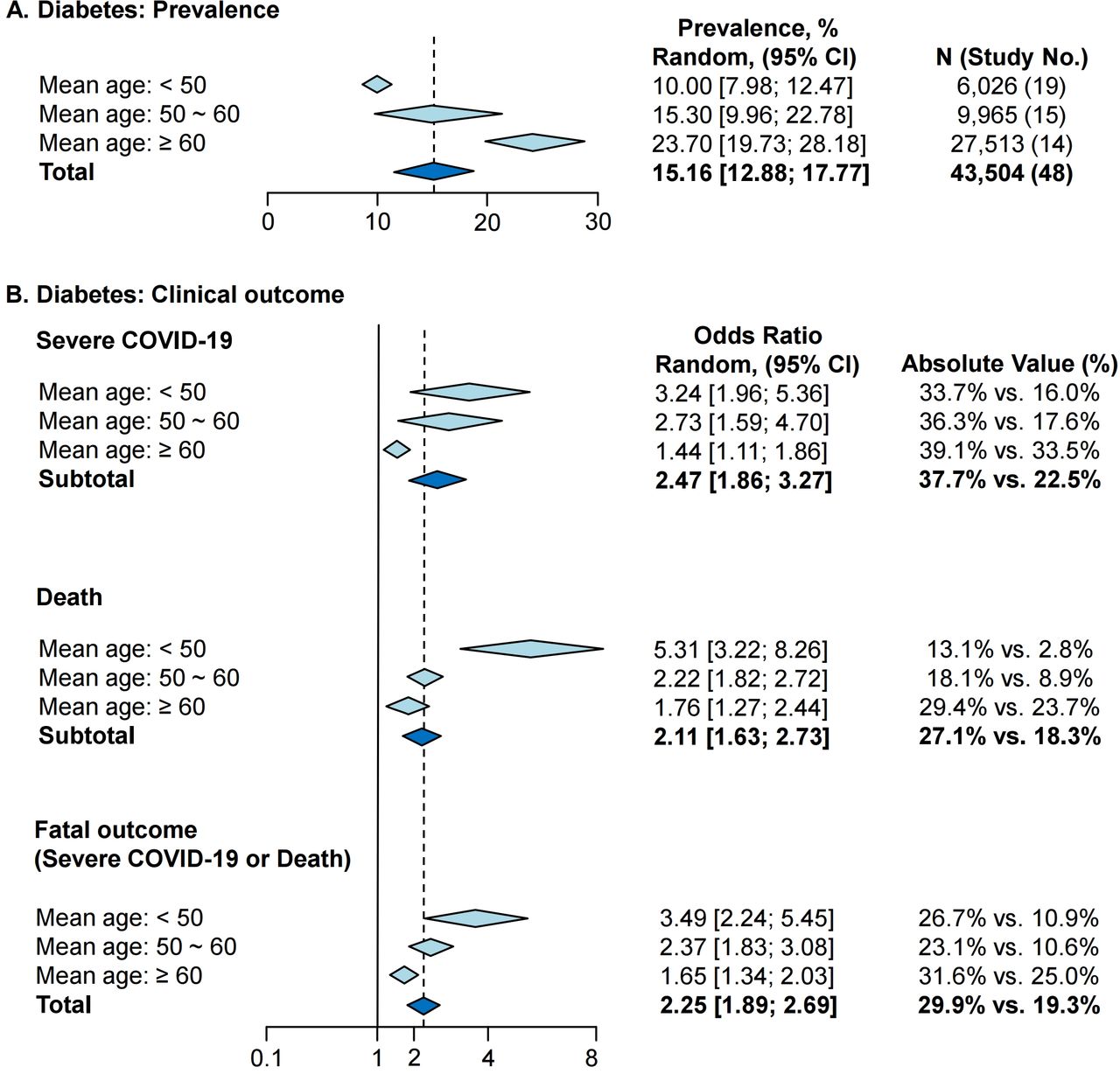
Prevalence of diabetes and clinical outcomes by age.
Cardiovascular disease
Overall prevalence of CVD in 44 studies was 8.33% (95% CI 6.32 to 10.91) and the prevalence was found to increase with age, wherein 4.51%, 9.26% and 15.02% of the patients aged <50 years, 50–60 years and ≥60 years, respectively, were found to have CVD (figure 4A, online supplemental figure 11). Results of the analysis showed that patients with COVID-19 and CVD had a high risk of developing severe disease (44.4% vs 23.3%, OR 3.15, 95% CI 2.34 to 4.25), death (35.7% vs 17.6%, OR 3.23, 95% CI 2.28 to 4.57) and fatal outcomes (37.1% vs 19.3%, OR 3.11, 95% CI 2.55 to 3.79) (figure 4B, online supplemental figures 12–15). Patients younger than 50 years of age had a higher risk of developing fatal outcomes (35.7% vs 10.9%, OR 5.66, 95% CI, 4.12 to 7.79) compared with those aged over 60 years (37.1% vs 23.8%, OR 2.10, 95% CI 1.68 to 2.61).

Prevalence of cardiovascular disease and clinical outcomes by age.
Meta-regression and sensitivity analyses
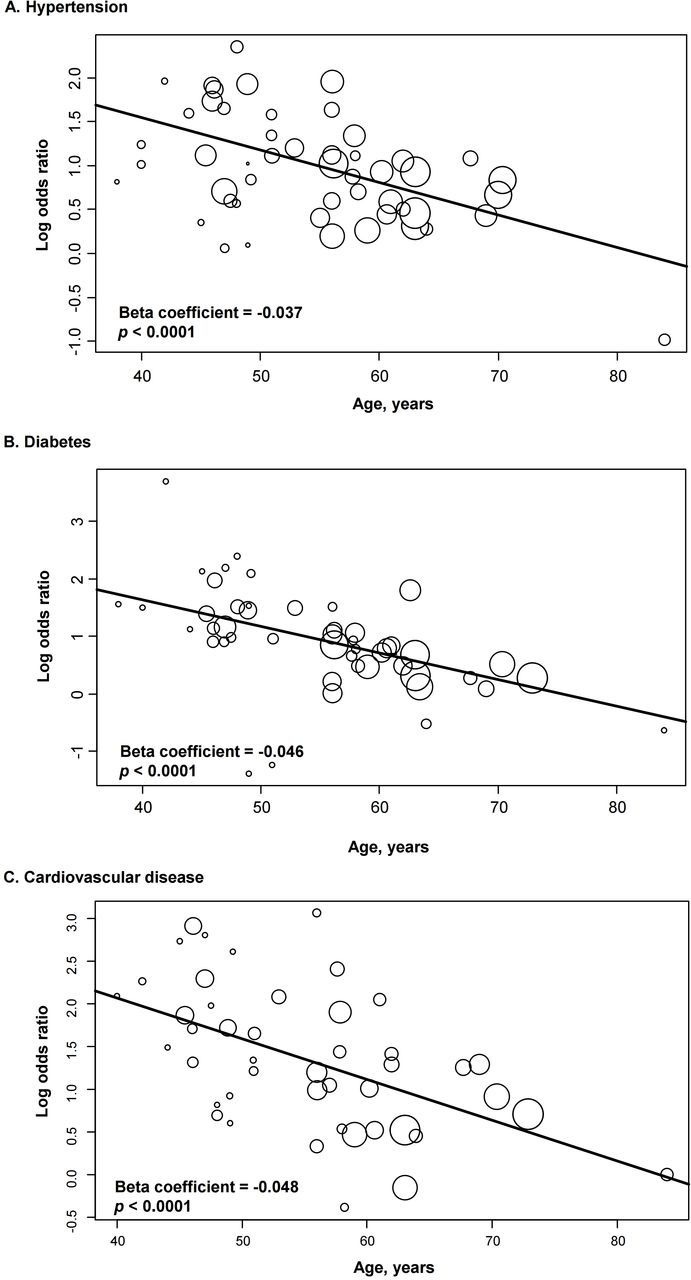
Random-effects meta-regression analysis demonstrated that the association between younger age and poor composite outcomes was affected by hypertension, diabetes and CVD (for all three parameters: p<0.0001) (figure 5). Sensitivity analysis based on study size and omission of individual studies yielded results that remained consistent with those of the primary analyses (online supplemental tables 4–7).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-regression analysis of risk of fatal outcomes.
Discussion
This systematic review and meta-analysis showed that risk factors for CVD (hypertension and diabetes) and CVD itself were significantly associated with fatal outcomes in patients with COVID-19 across all age groups. Although young patients (<50 years) had a lower prevalence of these comorbidities than elderly patients (≥60 years), their relative risk of developing a fatal outcome was higher than that of elderly patients.
Cardiovascular risk factors, CVD and COVID-19
Previous studies have demonstrated that patients with CVD or related risk factors were at significantly higher risk of developing poor clinical outcomes following COVID-19. The findings of the reviewed studies indicated that patients with underlying diseases were more vulnerable to COVID-19 as their comorbidities predispose them to infection and make them more likely to develop severe disease.16–18 Upon infection with SARS-CoV-2, an initial immune response is activated to protect the body from further viral invasion and growth, which occurs in the parenchyma of the lung and other epithelial sites. This immune response is associated with the appearance of mild symptoms and coincides with the activation of monocytes and macrophages. The ensuing inflammatory response causes blood vessel dilation, increased endothelial permeability and leucocytoplania. These events eventually lead to pulmonary distress with the development of parenchymal damage, fluid extravasation and hypoxaemia, ultimately causing increased stress on the cardiovascular system. Amplification of the host inflammatory response eventually leads to systemic inflammatory response syndrome.19
A study reported that the cardiovascular system was the main target of the virus, and it was also the most significant comorbid condition in all phases of COVID-19 infection.20 Evidence collected over time demonstrated that the heart may be the immediate target of SARS-CoV-221; and approximately 40% of the deaths in hospitalised, critically ill patients with COVID-19 in Wuhan, China, were associated with myocardial damage or heart failure.22 Cox regression analysis revealed that the mortality rate of patients with acute cardiac damage was higher than that of patients with chronic lung disease or a history of CVD.23 24 Pathologically, SARS-CoV-2 infection is known to induce endothelial inflammation in various organs due to both viral infection and the host’s own immune response.25 Thus, it is reasonable to conclude that patients with CVD or risk factors for CVD are more susceptible to COVID-19 infection. Furthermore, the cardiac injury caused by the comorbid condition and the infection itself significantly contributes to the development of adverse outcomes such as severe acute respiratory distress syndrome.
Impact of cardiovascular risk factors and CVD in young patients with COVID-19
To the best of our knowledge, the case fatality rate (CFR) of COVID-19 increases with age. Our review of literature indicates that the CFR of this infection is less than 1% among patients younger than 50 years of age, while the rates are 1.3%, 3.6%, 8% and up to 14.8% among patients in their 50 s, 60 s, 70 s and 80 s, respectively.26 Additionally, the CFRs of patients with CVD, diabetes, hypertension and cancer were 10.5%, 7.3%, 6% and 5.6%, respectively, while that of patients without any comorbid condition was only 0.9%.26
Based on the results of our age-stratified meta-analysis, young patients with CVD or risk factors for CVD (hypertension and diabetes) were at a higher risk of developing poor clinical outcomes than older patients. Several possible causes have been considered based on the results of previous studies; however, the exact cause remains to be established. A randomised study conducted in Denmark on 13,016 patients with hypertension reported that young patients (<50 years of age) had lesser awareness regarding hypertension and did not comply with compared with older patients.27 Another large prospective cohort study reported that young patients with hypertension had a higher prevalence of CVD and associated mortality rate than elderly patients.28 Furthermore, young patients with diabetes had higher prevalence of obesity and hypertriglyceridaemia as well as poorer glycaemic control, both initial and ongoing, than elderly patients (aged 50–70 years). Additionally, based on observations during follow-ups after initiation of treatment, achievement of glycaemic control was reported to be more difficult in younger patients than in the elderly.29 The prevalence of thrombophilia with high levels of coagulation factors was also significantly higher in young patients with CVD than among those in the healthy control group.30Andreotti and Becker, in a study that focused on young patients with arterial thrombosis, found that the prevalence of thrombophilic gene polymorphisms was significantly higher in these patients than among those in the control group.31 Autopsy results of patients infected with COVID-19 revealed widespread thrombosis with microangiopathy. Furthermore, the presence of microthrombi in capillaries was nine times higher in patients with COVID-19 than in those with influenza.32 It is plausible that patients with atherogenic and thrombophilic conditions have poorer prognosis due to increased metabolic demand and decreased cardiac reserves secondary to SARS-CoV-2 infection.
Association between cardiovascular comorbidities and cytokine storm in young patients with COVID-19
Characteristics of severe COVID-19 infection include hyperinflammatory syndrome, cytokine storm, acute respiratory distress syndrome and pulmonary, cardiac and/or renal damage. ‘Cytokine storm’ is a phenomenon wherein patients, usually those in advanced stages of COVID-19 infection, develop a rapid and uncontrollable inflammatory signalling cascade.33 It occurs in response to sustained hyperinflammation and can cause hypercoagulability in the microvasculature, which may lead to tissue injury, disseminated intravascular coagulation and multiorgan failure.34 35 Pre-existing organ damage due to comorbid CVD exacerbates the cytokine storm-induced organ damage.36–38 While these comorbidities are usually age related, the prevalence of hypertension and diabetes in young people continues to increase due to obesity, caused by sedentary lifestyle and a processed food diet, which in turn increases the risk of developing CVD.39 40 Furthermore, young patients tend to neglect fever or respiratory symptoms and do not seek medical help early in the course of COVID-19 infection.41 In summary, age itself or age-related diseases act as risk factors in elderly patients, while CVD and its risk factors are associated with a higher mortality rate in younger patients. This suggests that strict management of comorbid conditions can reduce mortality in both young and elderly patients.
This study has numerous strengths: a large sample of patients was assessed; all baseline characteristics of patients with COVID-19 were thoroughly evaluated; data from major biomedical literature were reviewed, which minimised the potential publication bias and other confounding factors. However, several limitations of this review should also be noted. First, this is a meta-analysis at the study level, and we could not properly assess the role of confounding factors. Since we stratified the data based on the mean age of patients in each study, various age groups were unavoidably combined. Nevertheless, we conducted a sensitivity analysis to overcome this limitation. Second, the criteria to determine whether a patient had severe or non-severe infection were not standardised. So, we defined severe COVID-19 based on the report of the WHO-China Joint Mission on Coronavirus Disease 2019. We categorised severe COVID-19 into presence of respiratory distress, need for ICU care and both. Third, results of contour-enhanced funnel plot and the Egger’s test performed to analyse the risk of small-study effect were found to be significant in the total group of hypertension, diabetes and CVD (online supplemental figure 16, table 3). However, results of the Begg’s test and trim-and-fill analysis did not reveal any evidence of small-study effect, and the results of sensitivity analysis based on study size remained consistent with those of the primary analyses.15 Fourth, there is a possibility that patients with multiple comorbidities were also included in the study. Fifth, the younger patients in death has a relatively extremely low I2 value compared with other groups. For this reason, we thought that the younger group had a lower comorbidity rate than elderly, and the event rate according to comorbidity was more pronounced. Therefore, it is important to show these results in a well-designed large cohort.
Conclusion
Based on the results of our meta-analysis, CVD and the associated risk factors (hypertension and diabetes) were closely related to fatal outcomes in patients with COVID-19 across all age groups. Although young patients had lower prevalence rates of cardiovascular comorbidities than elderly patients, relative risk of fatal outcome in young patients with hypertension, diabetes and CVD was higher than in elderly patients.
Key messages
What is already known on this subject?
Age greater than 60 years and the presence of comorbidities are established risk factors for mortality in patients with COVID-19.
Several patients die of comorbid cardiovascular disease (CVD) than of secondary bacterial pneumonia in event of influenza outbreaks. Furthermore, underlying CVD increases the severity and risk of developing complications from primary respiratory syndrome.
However, previous observational studies that evaluated these risk factors considered age as a potential confounding factor.
To the best of our knowledge, there are no comprehensive studies that have investigated the association between cardiovascular risk factors and critical outcomes of patients with COVID-19 based on age.
What might this study add?
CVD and its risk factors (hypertension and diabetes) were significantly associated with fatal outcomes in patients with COVID-19 across all ages.
Although young patients (<50 years) had a lower prevalence of cardiovascular comorbidities compared with elderly patients (≥60 years), their relative risk of developing fatal outcomes was higher than that of elderly patients.
How might this impact on clinical practice?
Among the patients with COVID-19, we need to pay special attention to young patients with cardiovascular comorbidities as well as the elderly.
Acknowledgments
The authors would like to thank Professor Juneyoung Lee for his statistical expertise.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SAB, SRK, M-NK and S-MP conceived the idea of the study. SAB and S-MP screened the studies and performed data extraction. SAB performed the statistical analysis, and S-MP supervised the analysis. SAB, S-MP, SRK, M-NK and WJS interpreted the findings. SAB drafted the manuscript; S-MP critically reviewed the manuscript, and SAB revised the manuscript for final submission. All authors have approved the final draft of the manuscript. S-MP and SAB are guarantors. S-MP accepts full responsibility for the work and conduct of the study, has access to the data and controls the decision to publish. The corresponding author attests that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. Additional data are available from the corresponding author on reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.