Article Text

Abstract
Objective To assess the efficacy and safety of subcutaneous treprostinil in adult patients with congenital heart disease (CHD)-associated pulmonary arterial hypertension (PAH) after 12 months of treatment.
Methods Consecutive adult patients with CHD–PAH received subcutaneous treprostinil to maximum tolerated doses in an observational study.
Results Advanced CHD–PAH patients with WHO class III or IV disease (n=32, age 40±10 years, 20 females) received treprostinil for suboptimal response to bosentan (n=12), WHO functional class IV disease (FC, n=7) or prior to bosentan approval (n=13). In the multivariate mixed model, mean increase in 6 min walk distance (6-MWD) from baseline to 12 months was 114 m (76; 152) (P<0.001). WHO FC improved significantly (P=0.001) and B-type brain natriuretic peptide decreased from 1259 (375; 2368) pg/mL to 380 (144; 1468) pg/mL (P=0.02). In those 14 patients who had haemodynamic data before and after initiation of treprostinil, pulmonary vascular resistance decreased significantly (from 18.4±11.1 to 12.6±7.9 Wood units, P=0.003). The most common adverse events were infusion-site erythema and pain. One patient stopped treatment because of intolerable infusion-site pain after 8 months of treatment. No other major treatment-related complications were observed. Five patients died during early follow-up, having experienced a decrease in their 6-MWD prior.
Conclusions Subcutaneous treprostinil therapy is generally safe and effective for at least 12 months and may be used in CHD-related PAH class III and IV.
- secondary pulmonary hypertension
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Congenital heart disease (CHD) is an increasingly recognised cause of pulmonary arterial hypertension (PAH), accounting for up to 42% of cases in national registries.1 The treatment of CHD-associated PAH is difficult because of a poor evidence base and because of the heterogeneity of the underlying CHD lesions.2 Furthermore, the prognosis in such patients with advanced disease (WHO class III or IV symptoms) is very adverse.3
In 2006, the relatively small BREATHE-5 study4 (54 patients with CHD–PAH, 37 treated with bosentan and 17 controls) showed an absolute increase in 6 min walk distance (6-MWD) of 53.1 m after 16 weeks of bosentan; this was the first randomised study of a PAH-specific therapy for patients with CHD. Since 2004, therefore, bosentan was increasingly used for such patients. In 2013, the Seraphin study5 reported the effects of macitentan in 62 patients with CHD–PAH (8.4%) of various aetiologies. In the overall study of 742 patients with PAH, 6-MWD increased by 7.4 m (treatment effect 3 mg macitentan vs placebo) and 12.5 m (10 mg macitentan vs placebo); the CHD patient benefit was not reported separately. Thus, outcomes in patients with CHD–PAH likely remain suboptimal6 and the evidence base for treatment options remains scant.
Prostacyclin is a highly effective treatment for PAH.7 Intravenous epoprostenol has a favourable effect on haemodynamics and exercise capacity in children with Eisenmenger syndrome (ES),8 without worsening oxygen saturation. A major drawback of intravenous prostacyclin therapy, however, is the need for permanent central venous access (such as a Hickman catheter); this leads to fear of systemic embolism in patients with obligatory right-to-left shunts and a high risk of infection, in particular.8 Regarding subcutaneous prostacyclin analogues, we have recently reported favourable outcomes and an acceptable safety profile with the administration of subcutaneous treprostinil in patients with PAH9 and CTEPH10. Based on this experience, we now report on the safety and efficacy of subcutaneous treprostinil in a consecutive series of patients with CHD–PAH, who had either failed bosentan therapy or in whom treprostinil was used as first-line treatment (mainly for WHO class IV symptoms or before bosentan approval in specific countries).
Our primary aims were therefore to assess 6-MWD response and safety after 12 months of subcutaneous treprostinil treatment. Furthermore, we analysed the effect of treprostinil therapy on WHO functional class (FC), B-type brain natriuretic peptide (BNP), haemodynamics and systemic oxygen saturation (SpO2) in CHD-related PAH.
Methods
Study population
We performed a three-centre observational cohort study (Budapest, Bratislava, Vienna). In addition to PAH associated with adult CHD, prospectively defined patient selection criteria included clinically symptomatic PAH (mean pulmonary arterial pressure (mPAP) >25 mm Hg in the presence of a mean pulmonary arterial wedge pressure <15 mm Hg) with no evidence of systemic ventricular dysfunction, and either (1) failure to improve clinically and haemodynamically on bosentan therapy or after discontinuation of bosentan due to adverse events,4 (2) need for medical treatment prior to bosentan approval or (3) WHO FC IV. All patients received optimal conventional therapy, at physician discretion. Conventional therapy included digitalis, diuretics, supplemental oxygen and surgical correction in operable patients. None had received any other PAH-specific agent.
The same exclusion criteria were used as previously described.9
Demographic and clinical data collected included age, gender, diagnosis, WHO FC, SpO2, 6-MWD and the measurement of BNP at baseline and after 1 year of treprostinil treatment. Right heart catheterisation (RHC) was performed using standard techniques before treprostinil initiation and after 1 year of treatment in a subset of the Austrian patients, at physician discretion. RHC was performed in Hungarian patients only in case of clinical deterioration. Cardiac output (CO) was calculated by the direct Fick method.
Patients provided written informed consent for the use of their medical records for the study.
Treprostinil therapy
Patients were instructed in the use of the positive pressure micro-infusion pump (CADD-MS3 Ambulatory infusion pump, Smith Medical, Minnesota, USA). Starting at 2 ng/kg/min, doses were increased over 16 weeks to a maximum dose, as tolerated. Dose increments were performed twice weekly with dose increases of 2.5 ng/kg/min on Tuesdays and Thursdays. Dose adjustments were performed every three months from then on and were based on signs and symptoms of PAH.
Local side effects, tolerability and pain management
The follow-up in the first three months was every 2–3 weeks to support the patients in dealing with infusion-site reaction and pain. The key strategy was to minimise infusion-site changes and maintain sites for a minimum of 4 weeks. Furthermore, the patients were instructed not to reduce the dose in the event of infusion-site pain.
The standard treatments of infusion-site pain were hot/cold compresses and topical application of three ointments containing various analgesic agents (formula D: ketoprofen 10%, lidocaine 5%, gabapentin 6%, ketamine 5%, amitriptyline 2%, clinidin 0.2%, pluronic lecithin organogel 35% ad 30.0), 5% lidocaine patches and 10% benzocaine.
Efficacy
Prespecified efficacy endpoints were 6-MWD, WHO FC, BNP plasma levels and (where available) haemodynamics, after 6 months and/or 12 months of treprostinil treatment, except in patients who were no longer alive at the relevant timepoints.
Statistics
Continuous parameters were summarised by means±SDs, or in the case of skewed distribution, by medians (25% percentile; 75% percentile). Discrete data were presented as counts.
Changes from baseline to follow-up (6 and 12 months) were assessed using linear mixed models. Differences between more complex (unstructured) and less complex (compound) models were assessed using the χ2 test. In case of significant differences between the two models, the more complex model was chosen. Additionally, linear mixed models were adjusted for confounders (gender, study centre and underlying defect of PAH–CHD) in multivariate analyses. Statistical significance was inferred at a two-tailed P value<0.05.
Data were analysed with IBM SPSS Statistics (V.21 for Mac, R (V.3.4.2 for Mac) and SAS (V.9.2 for Windows).
Results
Baseline clinical characteristics and haemodynamic variables
Thirty-two patients with PAH–CHD were treated with continuous subcutaneous treprostinil in three PAH centres (patients 1–24 in Vienna, patients 25–28 in Budapest, patients 29–32 in Bratislava). Clinical characteristics, exercise capacity (6-MWD), BNP and baseline haemodynamics according to subclassifications of PAH–CHD are shown in table 1. Mean age at initiation of treprostinil therapy was 40±10 years (20 females). There were 22 patients with ES (7 patients with pre-tricuspid defects, 15 patients with post-tricuspid defects). Of the 15 patients with ES with post-tricuspid defects, there were 5 patients with ventricular septal defect (VSD), 1 patient with persistent ductus arteriosus, 1 patient with aortopulmonary window and 8 patients with complex defects—unoperated or after a palliative surgery (two patients with a transposition of the great arteries, two patients with a double-outlet right ventricle, one patient with a double-inlet left ventricle, one patient with a complete atrioventricular septal defect, one patient with a pulmonary atresia (PA) with a VSD and aortopulmonary collaterals and one with a Pott’s shunt in a tetralogy of Fallot).
Baseline characteristics and haemodynamics of patients with PAH–CHD
One patient had PAH associated with non-correctable moderate to large systemic-to-pulmonary shunts without cyanosis at rest and two had PAH with small/coincidental defects with marked elevation in pulmonary vascular resistance (PVR) in the presence of small cardiac defects. Seven patients had PAH after repair.
In total, 13 patients were treated with subcutaneous treprostinil prior to bosentan approval, 12 patients received treprostinil because of a suboptimal response to bosentan (of these six were on combination therapy with bosentan and sildenafil before subcutaneous treprostinil was added due to inadequate treatment response, three patients experienced liver toxicity on bosentan and further three patients were on bosentan monotherapy when subcutaneous treprostinil was added) and 7 patients presented in WHO FC IV.
Prior to initiation of treprostinil therapy, mPAP was 73±21 mm Hg and PVR 19.1±10.1 WU. CO was 3.7±1.1 L/min, and cardiac index (CI) 2.1±0.6 L/min/m2. Mixed venous oxygen saturation was 68%±7%, and aortic oxygen saturation was 86%±8%. Baseline BNP levels were 1259 (375; 2368) pg/mL, and 6-MWD was 321±116 m. Prior to the initiation of treprostinil, 15 patients were classified as WHO FC III and 17 patients as WHO FC IV.
Baseline SpO2 was lower in patients with ES compared with other patients with PAH–CHD (P<0.001), while there was no difference in other baseline characteristics between the patients with ES and other patients with PAH–CHD.
Efficacy endpoints
6-MWD, WHO FC, BNP and SpO2
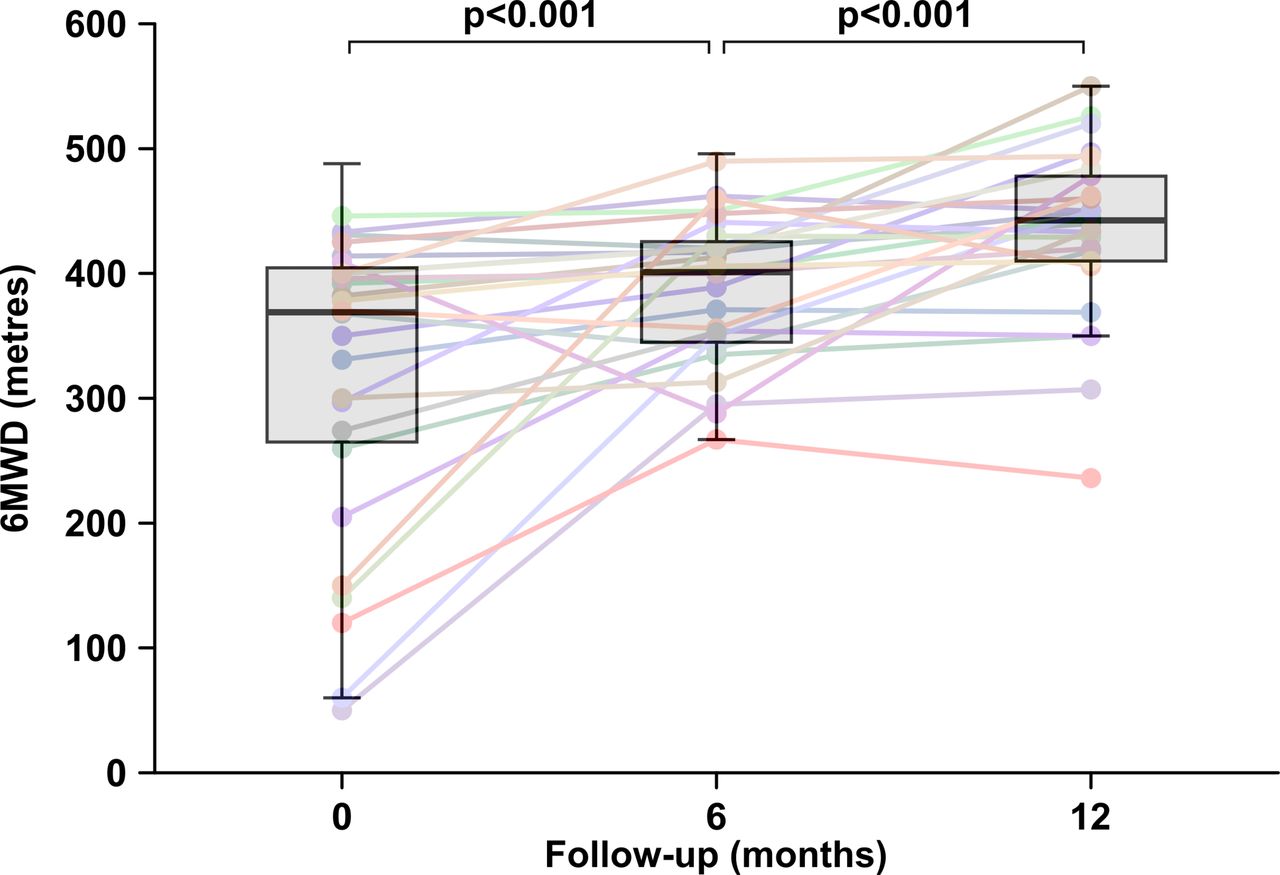
At 6 months follow-up, treprostinil dose was 17.3±7.7 ng/kg/min, and after 12 months 30.6±11.4 ng/kg/min. The mean increase in 6-MWD from baseline to 6 months was 58.7 m after 6 months (19.7; 97.7) (univariate and multivariate models: P<0.001) and 113.9 m (76.0; 151.8) after 12 months on treprostinil therapy (univariate and multivariate models: P<0.001; figure 1). Figure 2 depicts the improvement of FC from baseline to 6 and 12 months (at 6 months 18.8% of patients were in FC II, 75% in FC III and 6.3% in FC IV, univariate and multivariate models: P<0.001; at 12 months 56% of patients were in FC II and 44% in FC III, univariate and multivariate models: P=0.001; figure 2). BNP plasma levels significantly decreased from 1259 (375; 2368) pg/mL to 380 (144; 1468) pg/mL after 12 months (univariate model: P=0.026, multivariate model: P=0.020, figure 3). Treprostinil therapy led to an increase in SpO2 in patients with ES by 1.8% (0.5; 3.0), P=0.007, while SpO2 remained unchanged in other subgroups, after 12 months.

Effect of treprostinil treatment on 6 minute walking distance (6-MWD) at 6 and 12 months of treatment.

The change of WHO functional class (FC) at 6 and 12 months of treatment with subcutaneous treprostinil.

{kind=link}
{kind=link}
{kind=link}
Effect of treprostinil treatment on B-type brain natriuretic peptide (BNP) values at 6 and 12 months of treatment.
Haemodynamic effects of long-term continuous subcutaneous treprostinil
All patients underwent baseline RHC. Of 32 patients, 14 underwent follow-up RHC (table 2).
Change of haemodynamic variables from baseline to follow-up in patients with PAH–CHD
Treprostinil therapy was associated with significant improvements in mPAP (univariate model: P=0.015, multivariate model: 0.020), CO (univariate model: P=0.001, multivariate model: P=0.002) and PVR (univariate model: P<0.01, multivariate model: P=0.003).
Local side effects, tolerability and complications
No serious complications associated with treprostinil delivery occurred. The most common adverse events were infusion-site erythema in all, infusion-site pain (n=31, 97%) and local haematoma (n=6, 19%). There were two cases of infusion-site abscesses (n=2, 6%) requiring surgical incision and treatment with oral antibiotics, with no serious adverse consequences. Diarrhoea (n=7), jaw pain (n=6) and flushing (n=2) were mild and transient. One patient stopped treatment because of intolerable infusion-site pain after 8 months of treatment. There were no bleeding or thrombotic events reported or observed.
Deaths
Five patients (38±11 years) died between 6 and 12 months follow-up. Three patients were in WHO FC IV at baseline and four were males. Prior death they experienced no improvement in 6-MWD (mean change −22.3 m) at a treprostinil dose of 13.1±3.8 ng/kg/min. None of the deceased patients improved their WHO FC class after 6 months. All patients died due to right heart failure.
Discussion
Our study reports the efficacy and safety data of subcutaneous treprostinil therapy in adult patients with advanced CHD-related PAH. Although this comprises a heterogeneous group of patients, treprostinil-treated patients demonstrated marked and significant improvements in 6-MWD, WHO FC and BNP plasma levels after 12 months of treatment, and only a low rate of discontinuation for adverse effects (<5%). Unsurprisingly, five patients in this very unwell group of adults died from PAH rather than from any treatment-related complications. Otherwise, the most common adverse events were infusion-site erythema and infusion-site pain. Practical and psychological support was used to help the patients to manage pain and to cope with the infusion pump system. The key strategy was to minimise infusion-site changes and maintain sites for a minimum of 4 weeks because initial pain usually subsides after ~4–6 days.10
The medical treatment strategy for patients with PAH associated with CHD is mainly based on the clinical experience of experts rather than being formally evidence-based.2 Only one CHD-PAH-specific randomised controlled trial (RCT) is available, with bosentan therapy in patients with ES in WHO FC III, confirming a significant but relatively modest improvement in exercise capacity. Furthermore, the results of the recently presented second RCT (Maestro study)11 did not confirm the superiority of macitentan over placebo in the primary endpoint of change from baseline to week 16 in exercise capacity in 226 patients with ES (treatment effect (95% CL): −4.7 m (−22.8 to 13.5), P=0.612). Exercise capacity in patients with PAH may reflect disease severity and assist with prognostic evaluation. Physiologically, for patients with CHD-related PAH, exercise testing also provides information on change in arterial oxygen saturations during exercise. This is why we chose 6-MWD as a primary study endpoint of interest. The mean 6-MWD distance improvement in this study was 58.7 m after 6 months and 113.9 m after 12 months.
However, five patients did not respond sufficiently well to the treatment and died after 6 months follow up. Prior to death, these patients had had a decrease in 6-MWD by an average of 22 m; therefore, deterioration in 6-MWD on treprostinil could identify patients with a poorer prognosis. These data confirm that serial changes in standard clinical parameters (WHO FC, 6-MWD) have even more prognostic value compared with baseline parameters.12 However, whether these patients might eventually benefit from double or triple PAH-specific combination therapy needs to be assessed in future.
Our results are consistent with the few studies previously reporting benefits with PAH-targeted treatments have previously been assessed in CHD-related PAH. In 1999, Berman-Rosenzweig and colleagues presented a heterogeneous group of 20 young patients with PAH–CHD on long-term intravenous PGI2 therapy. Sixteen patients had RHC after an average of 15 months of continuous PGI2 therapy, showing significant improvement in haemodynamic and functional parameters.8 Of these, however, seven patients had had central venous line dislodgement, four had had central line infections and two reported pump malfunctions. In a study by Thomas and colleagues,13 eight adult patients with PAH–CHD were treated with continuous PGI2 treatment for more than a year. Of these, two were on subcutaneous treprostinil, four on intravenous epoprostenol and two on intravenous treprostinil. Long-term continuous PGI2 therapy resulted in haemodynamic and clinical improvements in this small study. Findings of our larger study with subcutaneous treprostinil in all treated patients were similar, with significant improvements in haemodynamics, 6-MWD and in resting oxygen saturation in patients with ES.
In our group of patients with the most severe haemodynamic compromise at baseline (mPAP=73±21 mm Hg), long-term PGI2 produced similar results on PA pressures without causing a reduction in systemic oxygen saturations. The avoidance of continuous intravenous therapy, however, reduces the substantial and important risks of embolism and infection, commonly experienced by patients treated in this way.14
Our study is limited by a relatively small sample size, although substantially larger than any other study yet reported of parenteral prostacyclin therapy in patients with CHD. Ours was not a randomised study. Another limitation of the study is the extended timeframe of patient recruitment because of the orphan disease status and variable drug approval status across European countries, including drug labelling. Furthermore, haemodynamic assessments in follow-up were done for clinical indications and thus were only available on a subset of patients. Long-term observations (beyond 12 months) are not yet available; however, most published studies on this subject have reported follow-up periods of only several weeks or months. Long-term clinical follow-up of this group will provide important further insights. Finally, treprostinil doses were uptitrated according to a study protocol over 16 weeks, but beyond this period the dose titration schedule was based on patients’ symptoms rather than prespecified dosing schemes. This is also why a full dose–response analysis was not possible, which is of course a limitation of our study.
In conclusion, subcutaneous treprostinil resulted in substantial improvements in exercise capacity, WHO FC class and BNP values in most of our patients with CHD-related PAH. Improvements in 6-MWD are substantially greater than those reported for oral PAH treatments. However, larger observational studies or RCTs are needed to confirm our findings. Subcutaneous treprostinil is generally safe for at least the first 12 months and may be considered for the treatment for CHD-related PAH.
Key messages
What is already known on this subject?
The treatment of congenital heart disease (CHD)-related pulmonary arterial hypertension (PAH) is difficult because of a poor evidence base and the heterogeneity and generally poor prognosis of this patient group.
What might this study add?
Subcutaneous treprostinil therapy avoids complications related to the use of continuous intravenous epoprostenol, including embolism and line infections. Subcutaneous treprostinil significantly improved exercise capacity, WHO functional class and B-type brain natriuretic peptide in the majority of 32 patients with CHD–PAH. Subcutaneous treprostinil is generally safe and may be considered for the treatment of CHD-related PAH.
How might this impact on clinical practice?
Subcutaneous treprostinil can thus be used as an alternative parenteral prostanoid in the treatment of CHD-related PAH, in patients with advanced disease. Improvement in 6 minute walk distance is substantially greater after 12 months of treatment compared with historical findings with oral PAH treatments.
References
Footnotes
Contributors NS-S and IML designed, wrote the protocol, submitted ethics application, included patients and treated patients. HG, RS-K and HB have included and treated the patients. OHB, DK, MK and IS submitted ethics applications, included patients and treated patients. CG, MG and JJ have prepared statistical analyses and the figures. NS-S, DC and IML have drafted the work.
Competing interests NS-S reports personal fees from GlaxoSmithKline, grants and personal fees from AOPOrphan Pharmaceuticals, grants and personal fees from Actelion, personal fees from Bayer AG, personal fees from Pfizer, personal fees from United Therapeutics, outside the submitted work.
Patient consent Obtained.
Ethics approval The databases used in this study were approved by the Ethics Committee of the Medical University of Vienna (# 972/2009), the Ethics Committee of the Gottsegen György Hungarian Institute of Cardiology and the Ethics Committee of the Slovak Medical University.
Provenance and peer review Not commissioned; externally peer reviewed.