Article Text

Statistics from Altmetric.com
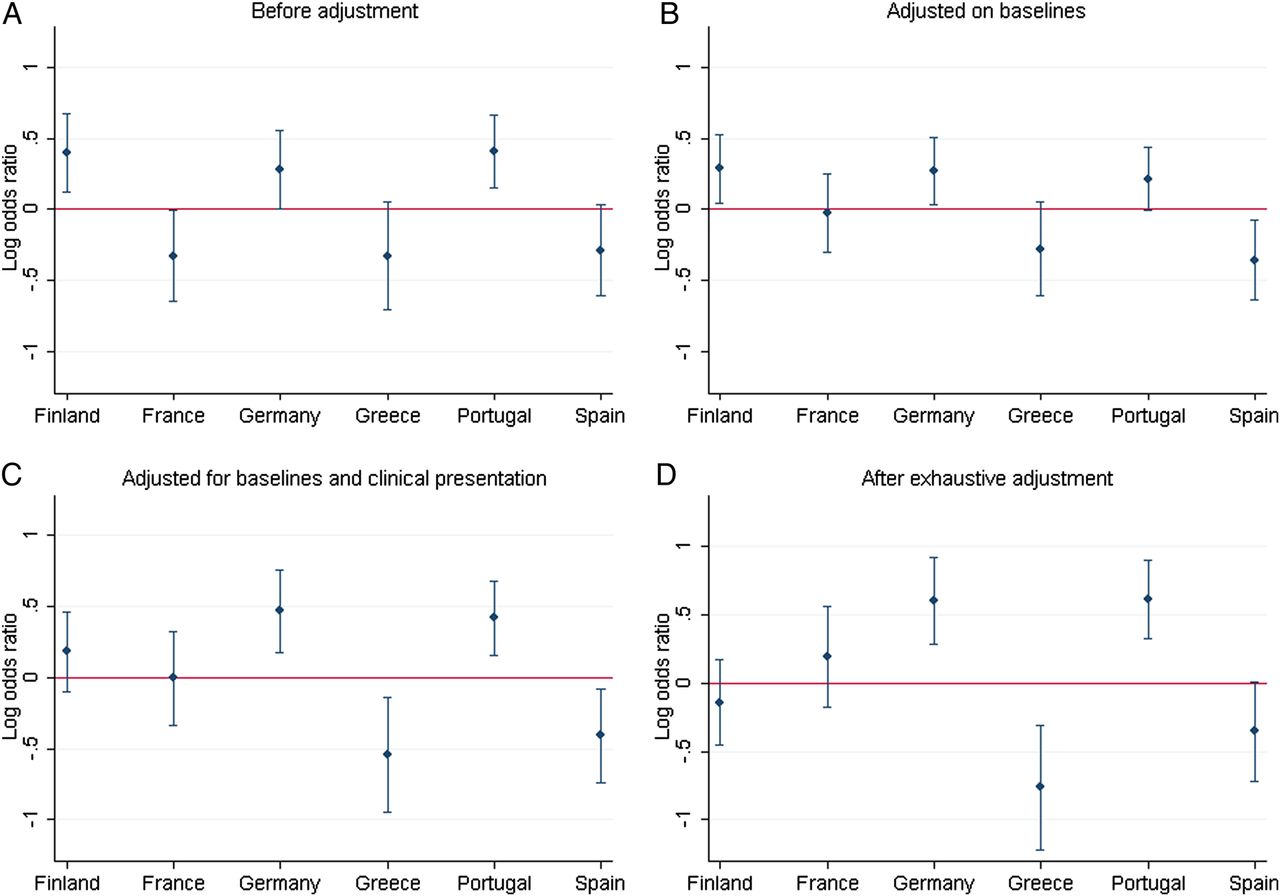
International guidelines for management of patients with an acute coronary syndrome (ACS) seek to improve the care of all patients, regardless of geographic location, and would be expected to reduce variation in outcomes between patients in different countries. However, national differences persist as detailed in the study by Dr. Andre and colleagues (see page 1201) who explored data from a population based cohort of over 12,000 consecutive patients with ACS in six European countries. As might be expected, differences in baseline characteristics explained some of the variation between countries for in-hospital mortality rates, which ranged from 15.1% in Germany to 4.9% in Spain for ST-elevation myocardial infarction (STEMI) patients. However, even after extensive adjustment for baseline factors, significant differences were still evident (Figure 1).
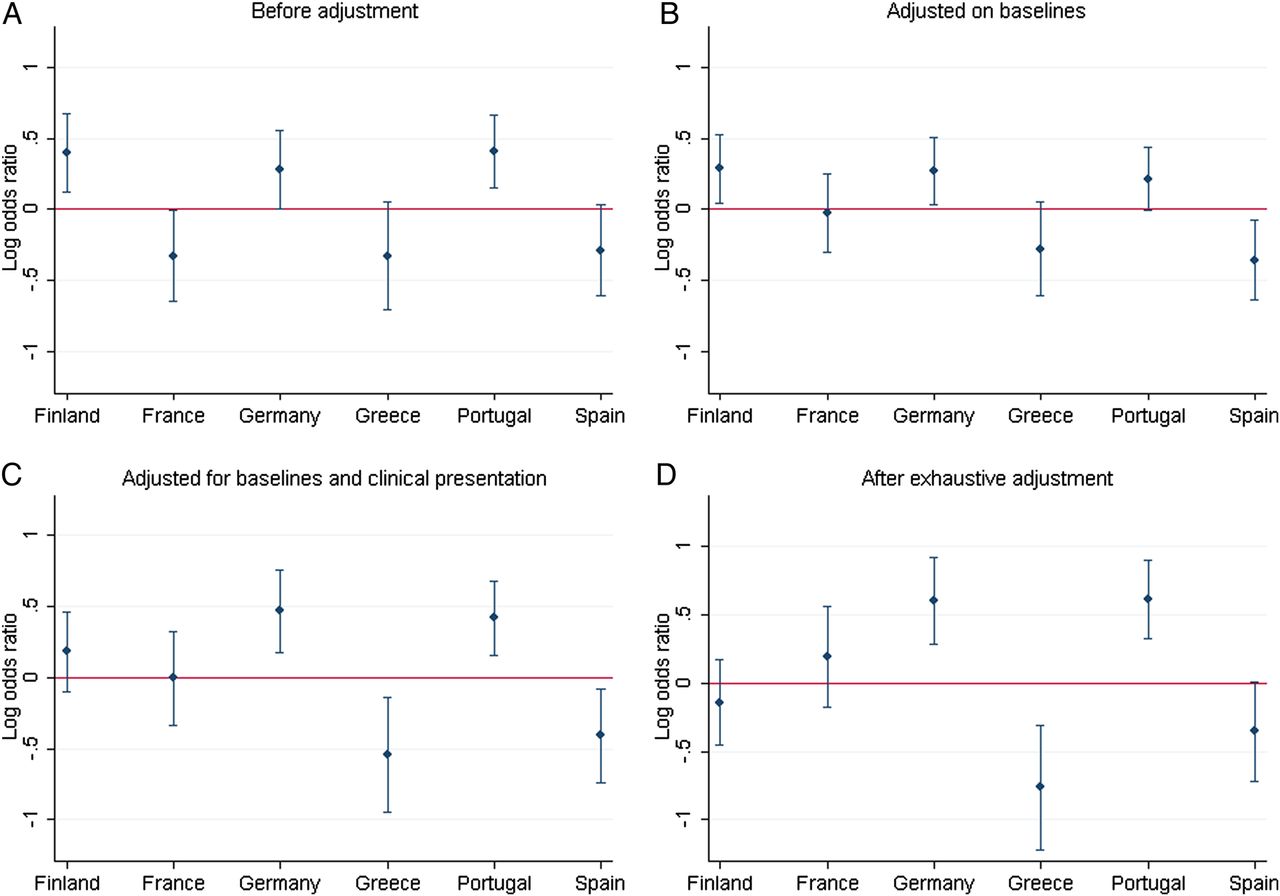
Logarithmic OR and 95% CIs for risk of inhospital death for each country according to multilevel analysis. (A) Without fixed-effect parameters. (B) After adjustment for baseline characteristics (age, gender, diabetes, hypertension, current smoking, obesity and history of coronary artery graft (CABG) surgery). (C) After adjustment for baseline and patients' clinical presentation (STEMI or non-ST-elevation myocardial infarction (NSTEMI), left ventricular EF, heart failure symptoms on admission). (D) After exhaustive adjustment for (C), management strategy (PCI-revascularisation, type of institution) and socioeconomic characteristics.
In the accompanying editorial, Drs. Ribeiro and Lemos (see page 1147) compare the findings from the current study with data from the Euro Heart Survey series which has shown a temporal decline in overall mortality from ACS across Europe but confirms persistent differences between countries. It remains unclear if these differences relate to differences in the timing and type of reperfusion therapy, adjunctive pharmacotherapy, or other aspects of healthcare delivery. Caution also is needed in equating in-hospital mortality rates with optimal patient outcomes. Further studies are needed to look at long-term survival, as well as post-ACS left ventricular function, quality of life, heart failure, recurrent ischemia and other adverse outcomes.
In patients with an implanted cardiac defibrillator (ICD) placed for primary prevention, should the ICD generator be replaced electively even if there have never been any appropriate ICD shocks? This vexing clinical questions is addressed in a study by Dr. Yap and colleagues. (see page 1189) In 275 patients with no prior appropriate shock at the time of first ICD generator replacement, the cumulative incidence of an appropriate ICD shock over the subsequent 3 years was almost 14% suggesting that ICD generator replacement is appropriate even in the absence of prior events. Specific factors predicting appropriate ICD shocks after replacement of the original generator could not be identified, with no difference between those with and without appropriate shocks with respect to a diagnosis of ischemic cardiomyopathy, left ventricular ejection fraction<25%, diabetes, severe heart failure symptoms, presence of biventricular pacing, or advanced age. In the accompanying editorial, Dr Roberts (see page 1149) concludes: “The study of Yap et al suggests that we should continue to replace ICDs in a primary prevention cohort even if they have not received therapy. However, perhaps it is time to more formally evaluate and establish a consensus as to how patients should be managed at the time of ICD generator change.”
The incidence of endocarditis (IE) is twice as high in men as women and previous studies suggest that the clinical presentation and outcomes in IE differ between men and women. Current guidelines list several indication for early surgery for IE: valve dysfunction causing heart failure, resistant organisms, heart block or paravalvular abscess, or other signs of persistent infection. Early surgery also might be considered in patients with large mobile vegetations or recurrent emboli. However, guidelines do not offer any sex-specific recommendations. In a pooled database of 466 (74%) men and 154 (25%) women from two population based IE cohorts, Dr. Curlier and colleagues (see page 1173) found that women with IE were older, had more comorbid conditions and underwent early valve surgery less often than men. However, even though women had a higher postoperative mortality, sex was not an independent predictor of one-year survival. Unfortunately, the database did not include enough information on post-operative events to determine the reasons for a higher postoperative mortality in women, which will be an important consideration for future studies.
This issue of Heart also includes the first in a series of “Straightforward Guide” articles. These reviews are the result of a partnership with the British Society of Cardiovascular Research with the goal of providing cardiovascular clinicians and researchers with, as stated by Professors Curtis, Jackson and Smart (see page 1150), “clear, unbiased, carefully researched review articles that set out what we actually know, rather than summarize what everybody thinks is true” about the basic principles of cardiovascular biology. The first article in this series on cardiovascular cell-based therapies by Professor Goumans and colleagues (see page 1153) provides useful insights into the potential value of transplanted stem cells in restoring myocardial function in the context of the stages of infarct healing (Figure 2).

{kind=link}
{kind=link}
Stages in infarct healing. Healing of myocardial infarction consists of 3 overlapping stages, each identified by different processes. Top row shows H&E staining of a murine left ventricular wall throughout the three phases after MI, at day 3, day 7 and day 14 respectively. Below is a magnification at the cellular level for each phase. Depicting from left to right: disruption of cardiac tissue and the influx of immune cells, thinning of the ventricular wall and proliferation of fibroblasts, infarct distention and the collagen scar. For each phase the processes and cells involved are listed, together with the potential cell therapy has and which cells could accomplish this.
The Image Challenge (see page 1192) in this issue includes multimodality imaging, as well as histologic images. This thought-provoking question is sure to increase your knowledge of the specific types of cardiac amyloidosis.
Linked Articles
- Review
- Image challenge
- Editorial
- Editorial
- Healthcare delivery, economics and global health
- Editorial
- Valvular heart disease
- Arrhythmias and sudden death