Article Text

Statistics from Altmetric.com
In patients with cardiovascular disease, both clinicians and patients struggle with the issue of obesity as related to cardiometabolic syndrome and recurrent cardiovascular events. In a prospective study of 5231 patients with cardiovascular disease but no history of diabetes, Dr. van der Leeuw and colleagues defined cardiometabolic dysfunction as 3 or more of the following: elevated blood pressure, high serum triglycerides, low high density lipoprotein, elevated fasting glucose or an elevated C-reactive protein level. Adiposity was defined by body mass index (BMI) as normal weight, overweight or obese. The risk of recurrent cardiovascular events was higher in patients with cardiometabolic syndrome in all three BMI categories whereas BMI alone was not a predictor of adverse cardiovascular outcomes (figure 1).
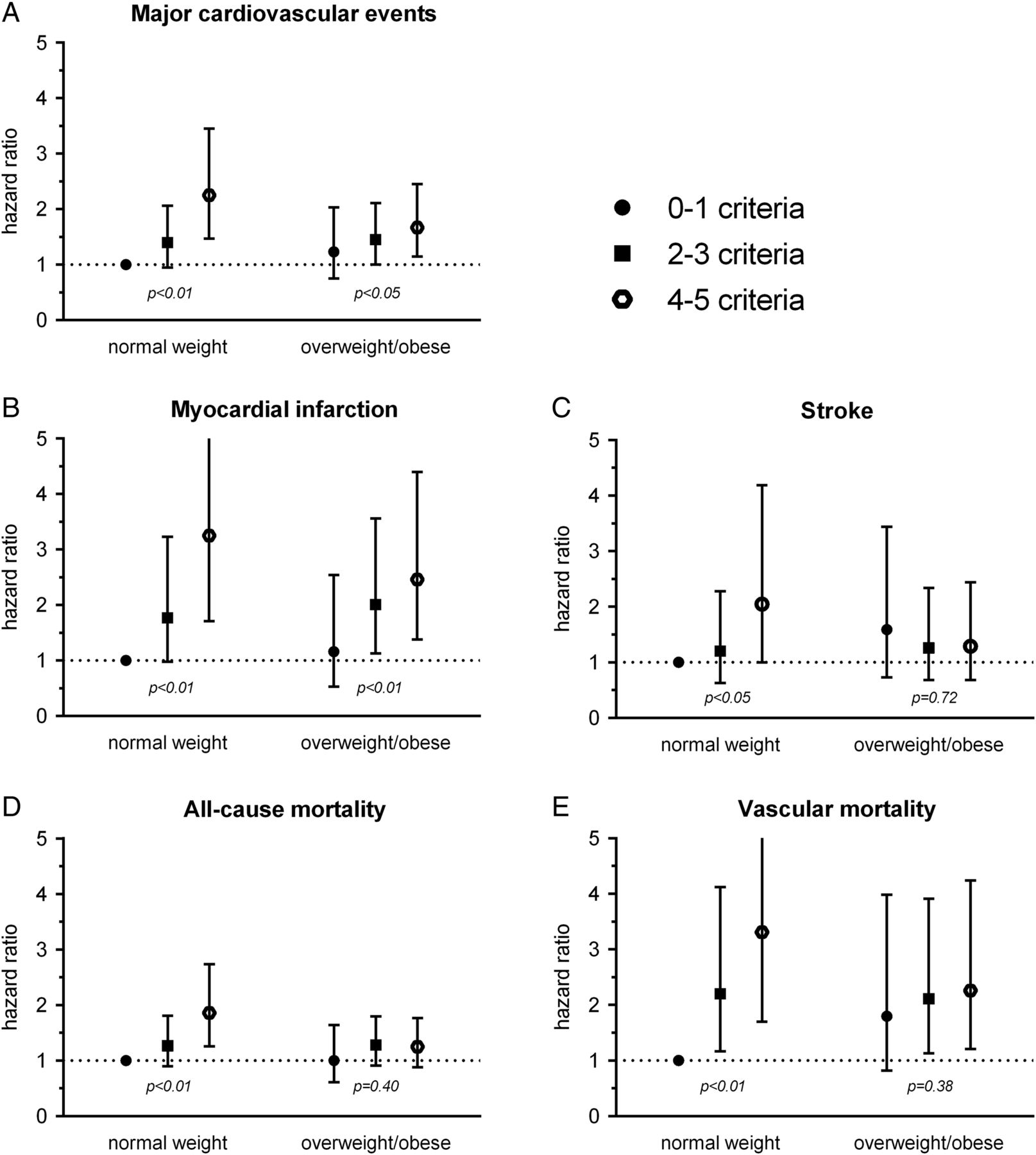
The risk of adiposity and level of cardiometabolic dysfunction on recurrent cardiovascular events and mortality. HRs adjusted for age, sex, current smoking, alcohol consumption, physical activity, use of lipid lowering agents, use of antiplatelet agents, years since first vascular event and number of affected vascular territories. Categorised by normal weight (20–25 kg/m2) and overweight or obesity (>25 kg/m2); p=p for trend.
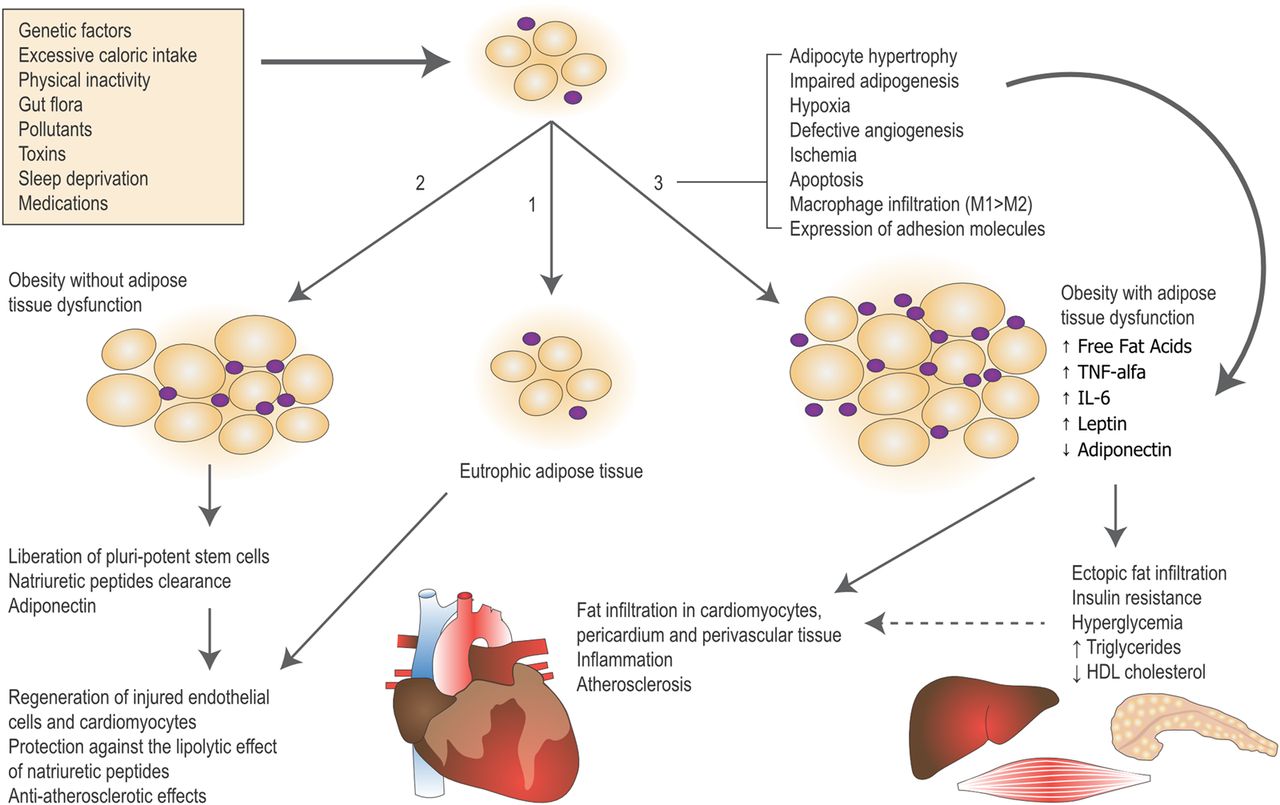
The controversy surrounding the relative role of obesity versus physiologic changes associated with obesity as a cardiovascular risk factor is concisely summarized in an editorial by Professors Beleigoli and Diniz (figure 2) (see page 1399). Cardiometabolic syndrome occurred in 70% of obese patients in this study, but also was present in 40% of normal weight patients. However, other factors that may be important in metabolic health, such as fitness levels are not included in the current definition of cardiometabolic syndrome. In addition, there is scant data on the long-term effects of weight control on cardiovascular outcomes in patients who are already overweight or obese. The authors suggest “Evaluating the cardiometabolic profile, and also the patient functional status and the presence of other conditions … helps physicians understand the patient's personal experience of illness, and balance between the benefits and risks of weight loss.”⇓
{kind=link}
{kind=link}
Overview of possible responses of the adipose tissue to genetic and environmental factors and its cross-talk with the cardiovascular system. Three possible responses of adipose tissue (AT) to genetic and environmental factors, according to individual susceptibility, are depicted: 1–AT remains eutrophic. The normal function of AT is associated with the following protective effects to the cardiovascular system (CVS)- secretion of adiponectin, which has antiatherosclerotic effects; clearance of natriuretic peptides, which reduces the lipolytic effects of the natriuretic peptides reducing the risk of cardiac cachexia; release of pluripotent stem cells promoting regeneration of injured cells; 2–Enlargement of the AT occurs mainly in the subcutaneous compartment with preservation of its storage capacity. AT function and the cross-talk with CVS remain normal; 3–The storage capacity of the subcutaneous AT is exceeded. Histological (hypertrophy, ischemia, inflammation, macrophage infiltration with predominance of M1 over M2 macrophages, apoptosis and cellular death) and functional (adipogenesis, defective angiogenesis, lipotoxiciy, hypersecretion of proinflammatory–TNF-α, IL-6 and leptin–and a decrease of anti-inflammatory cytokines, eg, adiponectin) alterations ensue in the subcutaneous and visceral AT. Deleterious cross-talk with the CV system occurs directly (ectopic deposition of fat and low-grade inflammation) and indirectly (insulin resistance) leading to atherosclerosis and metabolic abnormalities.
Optimal management of patients presenting to the Emergency Department with chest pain is challenging. On the one hand, we want to quickly identify high-risk patients who will benefit from early intervention for impending myocardial infarction. On the other hand, we want to avoid unnecessary testing and hospitalization in patients who are not having an acute coronary event. To address this issue, Dr. Body and colleagues (see page 1462) developed a clinical decision rule based on data from two large prospective observational cohorts. The Manchester Acute Coronary Syndromes (MACS) algorithm uses 8 simple clinical or laboratory variables to accurately identify those at very low risk (about 27% of the study group) who can be safely sent home versus those with a very high likelihood of an acute coronary syndrome (about 10% of patients). In the accompanying editorial, Drs. Brace-McDonnel and Laing note that the MACS clinical decision rule has the advantages of simpler clinical measures and a more clinically relevant 30 day time frame, compared to other approaches, such as the Thrombolysis in Myocardial Infarction (TIMI) and Global Registry for Acute Coronary Events (GRACE) scores which predict longer term outcomes. However, one of the biomarkers in the MACS score is not currently widely available, limiting immediate implementation of this approach, and further validation is needed. Finally, they conclude “perhaps now is also the time to seriously evaluate the false positives picked up by current practice and weigh it against the hidden risk that we add, the risk of over investigation and treatment.”
In a study from St Michael's Hospital in Toronto, Canada, Dr Zhang and colleagues (see page 1456) found that patients presenting with an acute coronary syndrome with an initial ECG showing a left anterior hemiblock (LAHB) are a high-risk subgroup but are less likely to undergo cardiac catheterization or revascularization. Unadjusted in-hospital and 6 month mortality rates were higher in patients with a LAHB compared to other acute coronary syndrome patients; although this difference disappeared when adjusted for comorbidities and other risk factors. It seems paradoxical that these high-risk patients showed no difference in adjusted mortality rates despite receiving interventional therapy less often. I agree with Drs Gale and Camm (see page 1406) who suggest in their editorial that “whether LAFB is directly implicated in missed ACS treatment opportunities or is simply a surrogate marker of comorbidity status is theoretical. Either way, closer attention to the provision and interpretation of the ECG for all patients with suspected ACS can only improve ACS quality of care and outcomes.”
The Education in Heart article in this issue reviews molecular imaging of atherosclerosis – an approach that have provided valuable insights into mechanism of disease over the past few decades and is now becoming clinically relevant in patient management as we move towards earlier detection and treatment of cardiovascular disease (see page 1469).
The Image Challenge case shows a distinctive echocardiographic image that all clinicians should recognize; see if you know the cause and clinical implications of these imaging findings (see page 1455).
Linked Articles
- Editorial
- Coronary artery disease
- Image challenge
- Editorial
- Education in Heart
- Coronary artery disease