Article Text

Abstract
A 64-year-old man presented with several weeks of intermittent irregular palpitations. He had no prior history of cardiac disease, hypertension or syncope. A 12-lead ECG revealed sinus rhythm with premature atrial and ventricular contractions and high QRS voltages consistent with LV-hypertrophy. Cardiac MR revealed asymmetrical septal hypertrophy and marked mid-myocardial hyperenhancement of the interventricular septum.
Statistics from Altmetric.com
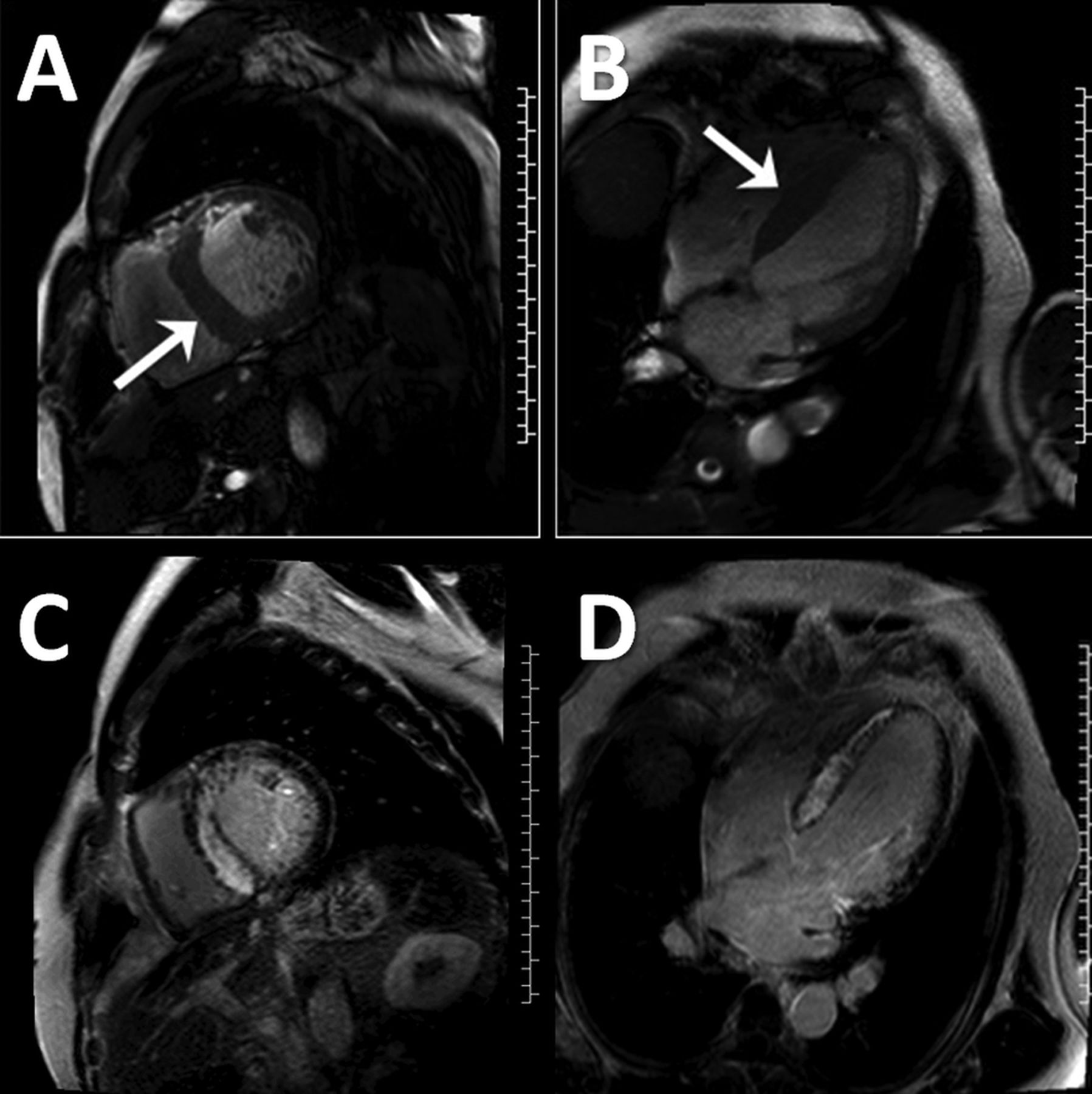
A 64-year-old man presented with several weeks of intermittent irregular palpitations. He had no prior history of cardiac disease, hypertension or syncope. A 12-lead ECG revealed sinus rhythm with premature atrial and ventricular contractions and high QRS voltages consistent with LV-hypertrophy (figure 1). Echocardiography showed asymmetrical septal hypertrophy but image quality was very limited due to poor acoustic windows. Cardiac MR was performed to better visualise myocardial morphology. This revealed asymmetrical septal hypertrophy (2.3 cm septum vs 1.0 cm inferolateral wall) (white arrow figure 2A,B) with a mildly enlarged LV cavity and an EF of 42% (see online supplementary videos 1 and 2). Late gadolinium enhancement imaging showed marked mid-myocardial hyperenhancement of the interventricular septum (figure 2C,D).

12-lead ECG showing sinus rhythm with premature atrial and ventricular contractions and high QRS voltages consistent with LV-hypertrophy.

(A) Short-axis cine image showing asymmetrical septal hypertrophy (2.3 cm septum (white arrow) vs 1.0 cm inferolateral wall) with a mildly enlarged LV cavity. (B) Four-chamber cine image showing asymmetrical septal hypertrophy (2.3 cm septum (white arrows) vs 1.0 cm inferolateral wall) with a mildly enlarged LV cavity. (C) Short-axis image showing marked mid-myocardial hyperenhancement of the interventricular septum. (D) Four-chamber image showing marked mid-myocardial hyperenhancement of the interventricular septum.

{kind=link}
{kind=link}
{kind=link}
(A) Endomyocardial biopsy showing amyloid deposition on H&E staining. (B) Endomyocardial biopsy showing amyloid deposition on Congo red staining.
Question
The most appropriate next step is:
-
Coronary angiography
-
Implantable defibrillator placement
-
Endomyocardial biopsy
-
Invasive electrophysiology study
For answers see page 177
Answer
From question on page 167
C: In myocardial infarction, hyperenhancement invariably involves the subendocardium, which is spared in this case. The mid-wall hyperenhancement seen here is highly suggestive of a non-coronary artery disease aetiology. Mid-myocardial septal hyperenhancement in association with asymmetrical septal hypertrophy is common in hypertrophic cardiomyopathy.1 ,2 However, the hyperenhancement characteristically appears in a diffuse, patchy mid-wall distribution with predilection for the anterior and posterior RV insertion sites. In this case, the extent and intensity of the hyperenhancement as well as the presence of LV enlargement and dysfunction were not typical for hypertrophic cardiomyopathy. There is no indication for implantable defibrillator placement or invasive electrophysiology study at this stage. Endomyocardial biopsy was therefore performed to try to obtain a diagnosis. This showed amyloid deposition on H&E (figure 3A) as well as Congo red (figure 3B) staining confirming the diagnosis of cardiac amyloid. Light-chain amyloidosis was confirmed on further workup including bone marrow biopsy.
This case demonstrates that cardiac amyloid can occasionally present with electrocardiographic LV-hypertrophy, asymmetrical septal hypertrophy and a focal mid-myocardial (as opposed to diffuse subendocardial) hyperenhancement pattern on cardiac MR, which may mimic hypertrophic cardiomyopathy.1–4 Distinguishing between these entities may require endomyocardial biopsy and has significant prognostic and therapeutic implications.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video 1
- Data supplement 2 - Online video 2
Footnotes
-
Contributors AF-F cared for the patient, supervised all imaging studies and drafted the manuscript. MAB helped draft the manuscript. All authors contributed to writing and editing of manuscript. All authors read and approved the final manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Institutional IRB.
-
Provenance and peer review Not commissioned; internally peer reviewed.