Article Text

Statistics from Altmetric.com
In this issue of Heart Dr. Bhattacharyya and colleagues (see page 370) looked at indications for exercise and dobutamine stress echocardiography in a series of 250 consecutive patients. Their findings support Appropriate Use Criteria (AUC) which help separate patients at high versus low risk of subsequent coronary disease events. Inducible ischemia was seen in 45.5% of those with versus only 12.7% in those without an appropriate indication for stress testing (p<0.0001). The authors suggest that AUC can reduce unnecessary stress testing in lower risk patients.⇓

Kaplan–Meier survival curves comparing survival in patients whose indication for stress echocardiography was classified as appropriate, uncertain or inappropriate (p=0.01 for appropriate vs inappropriate; p=0.05 for appropriate vs. uncertain).
In an accompanying editorial, Professors Fonseca and Marwick (see page 357) have a different point of view, reminding us that AUC were developed in the USA using a consensus approach, not based on clinical outcomes. While it is encouraging that AUC help identify higher risk patients, there are many clinical settings in which a normal stress test result has value; for example, confirming that a conservative medical therapy approach is reasonable or reassuring an anxious patient. In addition, there is little evidence that AUC have improved medical practice with no change in the relative number of “appropriate” and “inappropriate” stress tests over the last decade. Reducing unnecessary diagnostic studies is an essential element in reducing health care costs and, so far, publication of AUC has not achieved this goal. We hope to see future research studies on more effective approaches to utilization of diagnostic testing based on both cost analysis and clinical outcomes.
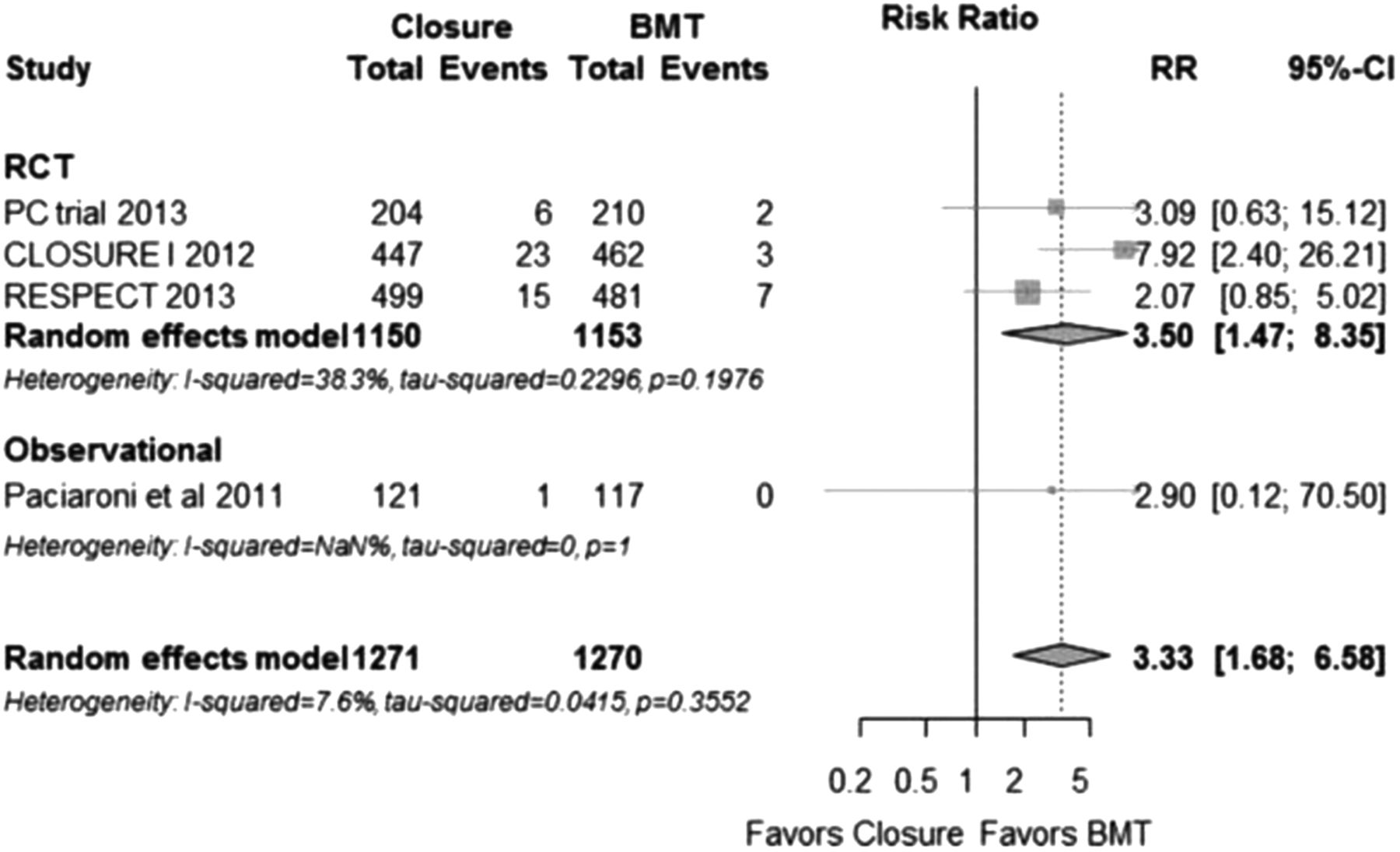
Patients with cryptogenic stroke have a high prevalence of patent foramen ovale (PFO) but the value of transcatheter PFO closure compared to medical therapy has been controversial. In a meta-analysis of 4335 patients included in 3 randomized controlled clinical trials and 11 non randomized observational studies, Dr. Meier and colleagues (see page 389) did not find convincing evidence that PFO closure is superior to medical therapy for preventing recurrent stroke, although there was a slight trend in the data when a time to event analysis, with strict multivariate analysis, was used (HR 0.58, 95% CI 0.33 to 0.99, p=0.047). There was no difference in bleeding or mortality between groups, but there was a higher incidence of atrial fibrillation with PFO closure (RR 3.50, 95% CI 1.47 to 8.35, p=0.005).⇓

Forest plot of risk ratios (RR) for atrial fibrillation. BMT, best medical therapy; RCT, randomised controlled trials.
Future clinical trials are needed to resolve the question of whether PFO closure is superior to medical therapy for preventing recurrent cryptogenic stroke. Given the findings from this meta-analysis, these studies should include robust methods for detection of atrial fibrillation, as well as recurrent stroke, to ensure that our therapy for one disease does not create another.
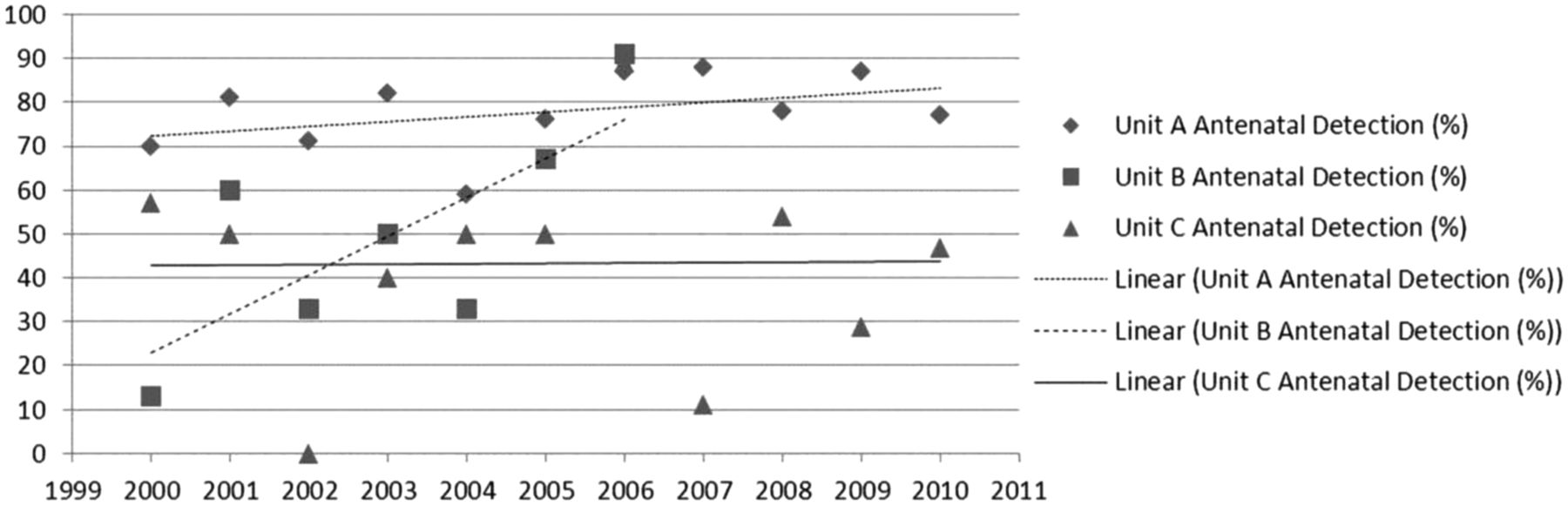
Prenatal screening with ultrasound for major congenital heart disease (mCHD) now is routine at most medical centers. However, in a detailed analysis by Dr. Gardiner and colleagues (see page 375) only 31% of infants with transposition of the great arteries and 37% of infants with aortic coarctation are diagnosed before birth. In addition, prenatal detection rates vary widely depending on whether the hospital has an onsite fetal medicine unit, telemedicine access to a perinatal cardiologists or only sonographers supported by local obstetricians.⇓

{kind=link}
{kind=link}
{kind=link}
Linear trends for prenatal detection of major congenital heart disease in three screening hospitals over 11 years showing a steady and high detection rate in Hospital A, improvement in Hospital B (data only between 2000–2006), and a steady but poorer detection rate in hospital C. ♦: Hospital A; ▪: Hospital B; ▴: Hospital C, and linear trends for Hospital A: …………; Hospital B: ……… and Hospital C __________
The authors suggest that creation of a database that links maternal screening with post-natal diagnosis of mCHD would allow hospital-specific interventions to improve prenatal detection rates.
The Eduction in Heart article by Professor Harvey White and colleagues (see page 424) in this issue focuses on myocardial infarction with a review of the underlying pathophysiology, diagnostic modalities and the universal definition of myocardial infarction. Summary boxes highlight other causes of elevated troponin values, the classification of types of myocardial infarction, and the clinical implications of the Third Universal Definition of Myocardial Infarction. Remember that Education in Heart articles offer CPD/CME credits if you answer the accompanying multiple choice questions.
The Image Challenge by Dr. Muthumala and colleagues (see page 434) reminds us that we need to pay close attention to simple diagnostic tests, such as the chest radiograph and electrocardiogram.
Linked Articles
- Coronary artery disease
- Editorial
- Aortic and vascular disease
- Congenital heart disease
- Education in Heart
- Image challenge