Article Text

Statistics from Altmetric.com
IMAGE CHALLENGE
A 74-year-old man who had been diagnosed with LV hypertrophy (LVH) at the age of 60 years in another hospital was referred for evaluation of repeated hospitalisation for heart failure. He complained shortness of breath, but no chest pain or syncope. Significant information was not obtained in spite of a carefully taken past and family history. There was no history of hypertension. His blood pressure was 118/60 mm Hg and the third heart sound was audible. With the patient sitting, the right internal jugular vein was visibly distended. Brain natriuretic peptide level was 498 pg/mL. Transthoracic echocardiography at first evaluation in our hospital is presented (figure 1; see online supplementary video). We also reviewed his echocardiographic data at his initial diagnosis of LVH at the age of 60 years (figure 2; see online supplementary video). Coronary angiography showed no significant lesions.
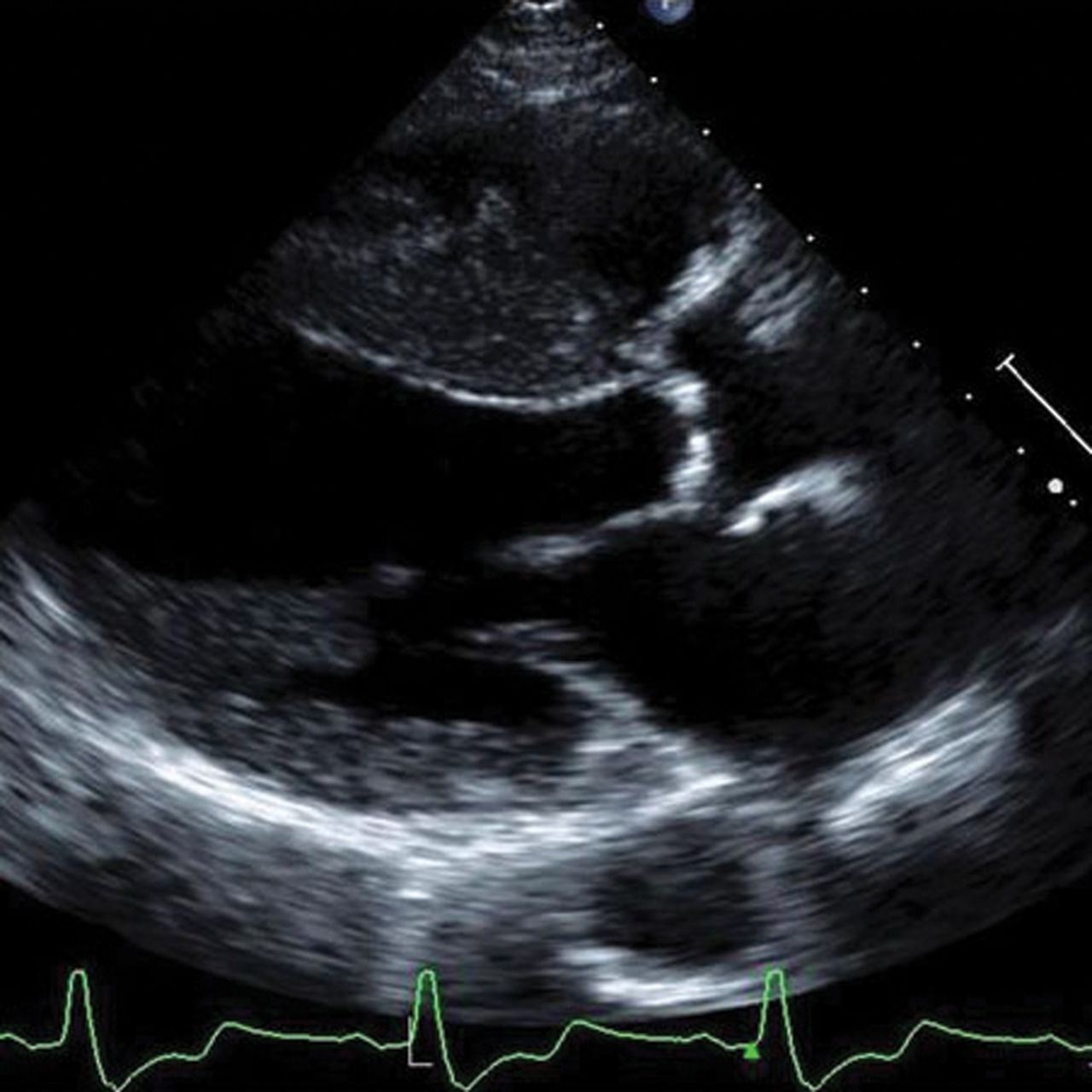
Parasternal long-axis view of the left ventricle at the age of 74 years.
{kind=link}
{kind=link}
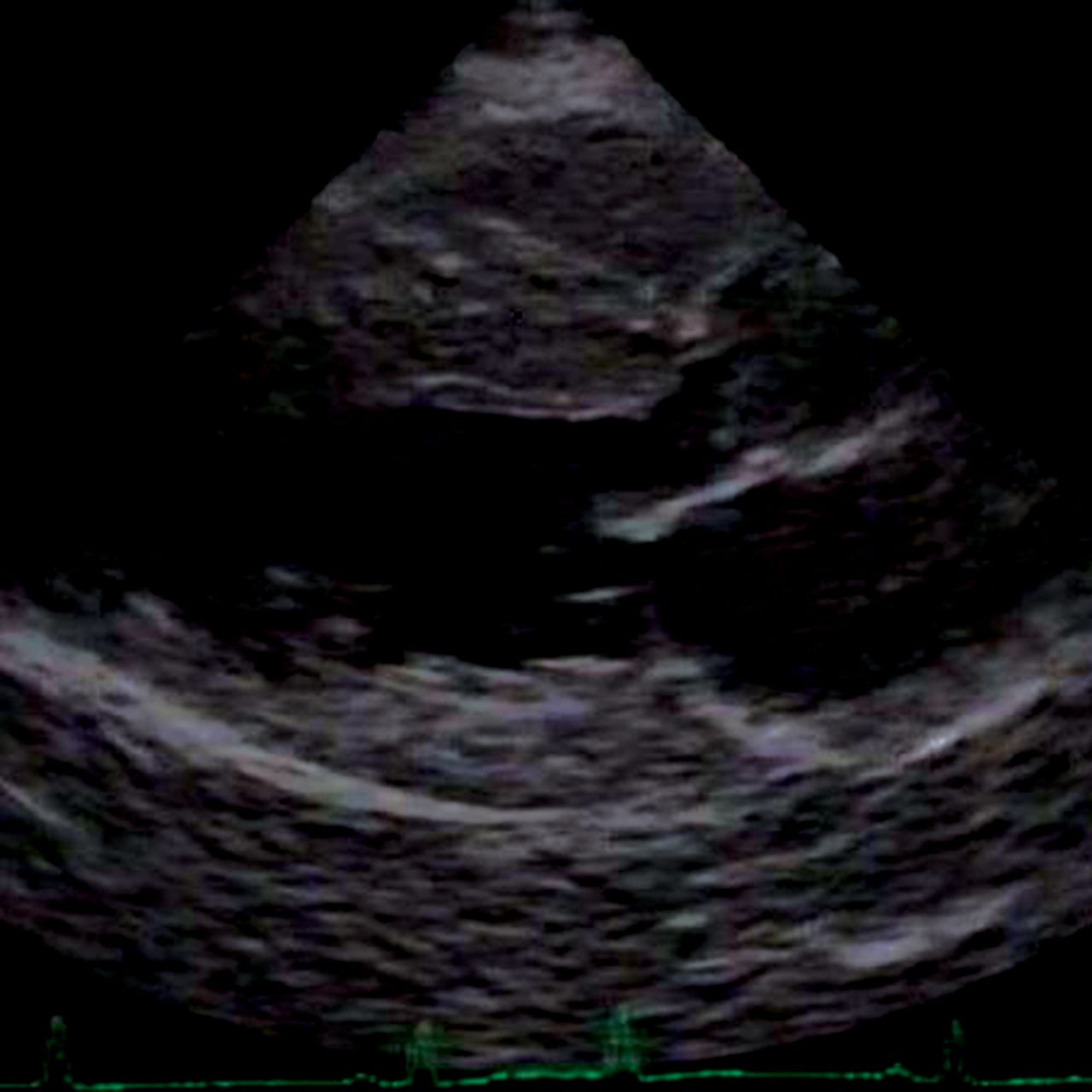
Parasternal long-axis view of the left ventricle at the age of 60 years.
QUESTION
The next best step for diagnosis of cause of LVH is:
-
to evaluate presence of an M-protein in serum
-
to measure transferrin saturation
-
to screen sarcomere protein gene mutations
-
to measure alfa-galactosidase A activity
For answers see page 742
ANSWER: D
From the question on page 710
Transthoracic echocardiography (figure 1) showed asymmetric septal hypertrophy (ASH) with interventricular septal wall thickness of 16 mm and posterior wall thickness of 11 mm and reduced LV EF with predominantly hypokinetic wall motion of the posterior region. But, at the age of 60 years he had not ASH but concentric LVH with interventricular septal wall thickness and posterior wall thickness of 16 mm and normal LV systolic function (figure 2). Biochemical analysis revealed low alfa-galactosidase A activity in his plasma (0.3 nmol/h/mL (normal: 3.6–17.6)).
Based on his low alfa-galactosidase A activity, a diagnosis of cardiac Anderson–Fabry disease was finally made. Anderson–Fabry disease is an X-linked storage disorder, and the disease is a relatively prevalent cause of LVH, mainly concentric hypertrophy.1–3 In terminal-stage patients with Anderson–Fabry disease, LV dysfunction with localised thinning of the base of the LV posterior wall is seen. Disease-specific enzyme replacement therapy is available and has been shown to be beneficial in patients with Anderson–Fabry disease.4 Cardiac amyloidosis shows concentric LVH and evolves into diffuse hypokinesis of LV wall in the advanced stage. Hemochromatosis can lead to a dilated cardiomyopathy. In hypertrophic cardiomyopathy (HCM), LVH is usually asymmetric and predominantly septal, but akinesis and thinning of septal wall develop as LV remodelling progresses. Although ‘ASH’ is often used as a synonym of HCM, it is important to recognise that LV wall thinning limited to the LV basal posterior wall seen in the advanced stage of Anderson–Fabry disease may lead to this morphology.5
Footnotes
-
Contributors We have contributed to this study, and have read and approved the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Approved by Kochi Medical School.
-
Provenance and peer review Not commissioned; internally peer reviewed.