Article Text

Abstract
Introduction Acute heart failure is an increasingly common cause for hospital admissions. It is largely presumed that these patients have breathlessness at rest, but National Audit data suggest otherwise. In clinical practice, treatment for acutely breathless patients is usually given within minutes of presentation but novel therapies studied in trials are not usually implemented until 6–12 h after initial presentation and treatment.
Methods We collected detailed information retrospectively from the case-notes of a representative sample of patients admitted with a primary death/discharge diagnosis of heart failure to determine what proportions of patients were Short Of Breath At Rest (SOBAR) and Comfortable At Rest but Breathless On Slight Exertion (CARBOSE). We measured blood pressure (BP), heart rate and respiratory rate (RR) at initial presentation at 1, 2, 3, 4–6, 6–12 and 12–24 h. Results are described in median and Interquartile (IQR) ranges and the proportion with a systolic BP (SBP) >125 mmHg (RELAX-HF entry criterion). We assessed mortality in different groups at discharge, and 30 days, 90 days and 180 days after presentation.
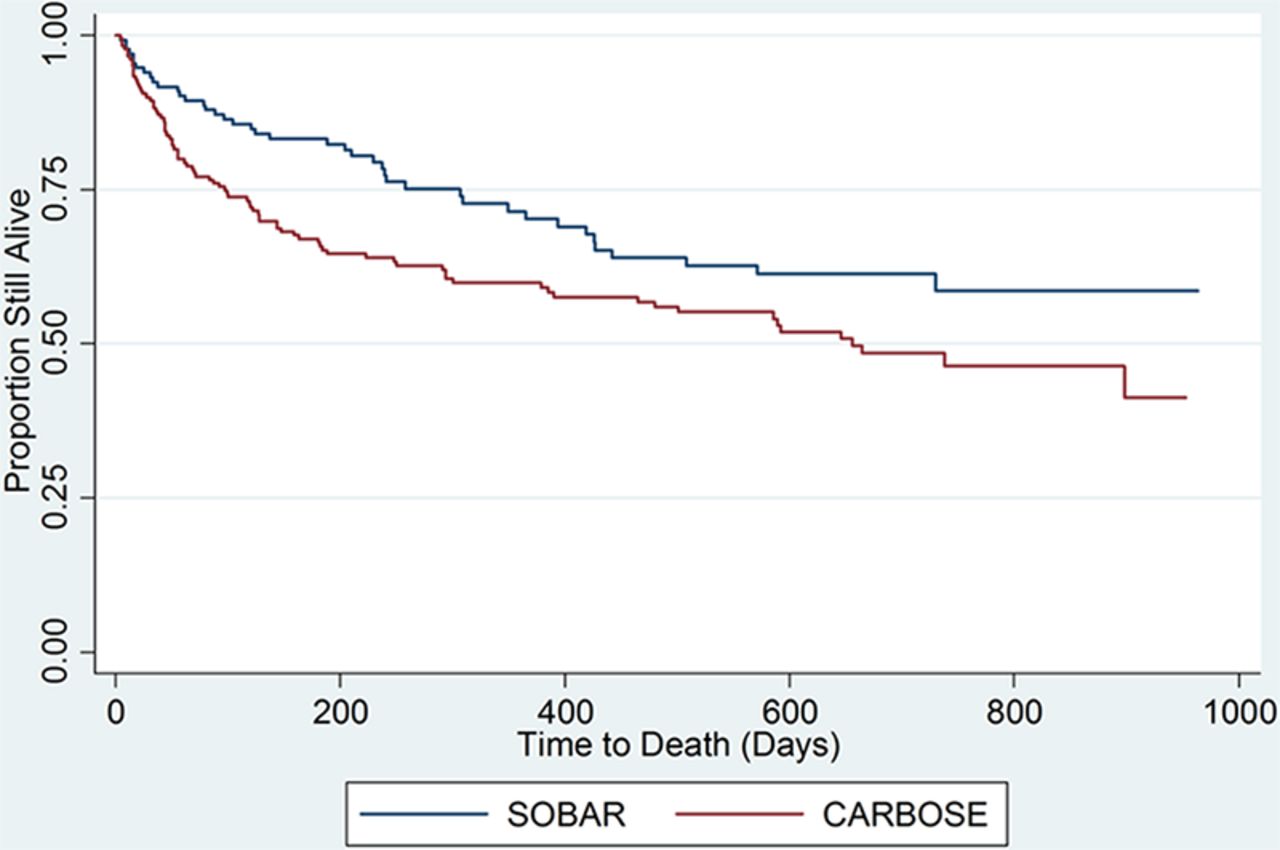
Results Of the 307 patients enrolled, 43% had SOBAR and 57% CARBOSE; 34% were women, the median age was 77 (IQR 71–84) years and median amino-terminal probrain natriuretic peptide (NT-proBNP) was 4082 (IQR: 1895–10,279 ng/L). Compared to patients with CARBOSE, patients with SOBAR were younger (76 vs 78 years), had higher HR (100 vs 85 bpm), SBP (141 vs 122 mmHg) and RR (24 vs 18 rpm) and were more often in atrial fibrillation (54% vs 49%). SBP was >125 mmHg in 73% patients with SOBAR and 46% with CARBOSE. SBP (122–116 mmHg), HR (85–82 bpm), and RR (18–18 rpm) changed little amongst patients with CARBOSE in the first 4–6 h but all declined steeply in patients with SOBAR (141–128 mmHg, 100–90 bpm, and 24–20 rpm, respectively). Overall 47% patients died in CARBOSE and 31% in SOBAR (HR 1.58, p-value = 0.02). After adjusting for age and sex, patients with CARBOSE had significantly higher all-cause mortality than SOBAR (HR = 1.70, p = 0.004). Further adjustment with Systolic Blood pressure, Heart Rate, Respiratory Rate, Creatinine levels and LVSD provided more evidence that CARBOSE was independently predictive of all-cause mortality (HR = 2.26, p = 0.003).
Conclusion Most patients admitted with a primary diagnosis of heart failure present with CARBOSE rather than SOBAR. Patients presenting with SOBAR had, as expected, higher BP, heart and respiratory rates. CARBOSE showed little variation in these clinical characteristics in first 24 h but suffered higher mortality during hospital admission and at 30, 90, 180 days of presentation. Despite a higher risk of mortality, due to low BP, relatively fewer numbers of patients were suitable for serelaxin in CARBOSE.
{kind=link}
- acute heart failure
- breathlessness
- congestion