Article Text

Abstract
Introduction Coronary stent thrombosis (ST) is a rare but potentially lethal complication of percutaneous coronary intervention (PCI). Previous studies have identified various patient, lesion and procedure-related risk factors, but there are currently no risk scoring tools in clinical use. In this study, we aimed to develop a scoring system to predict the risk of ST at different time points following PCI, to help guide the potency and duration of antiplatelet treatment.
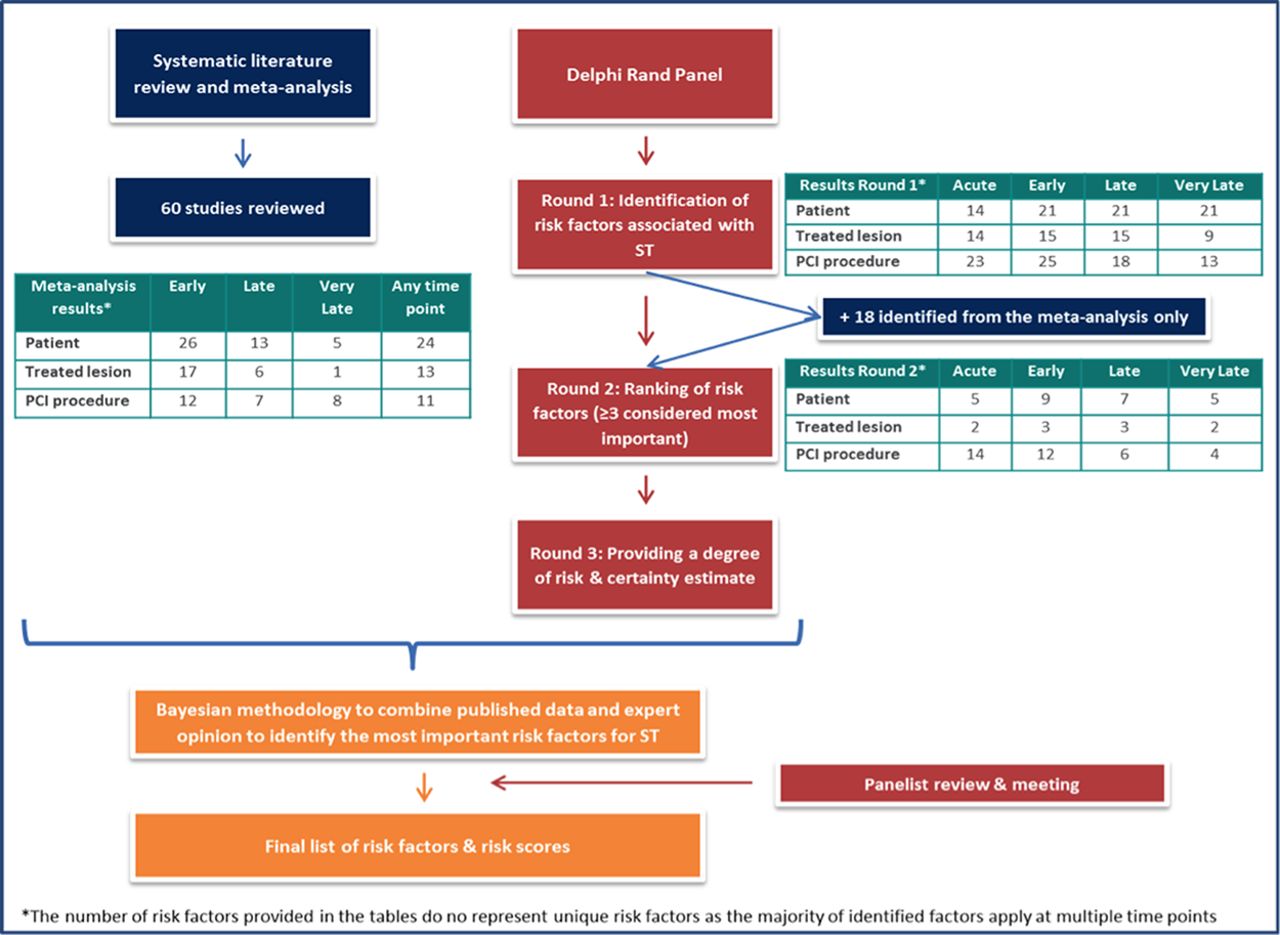
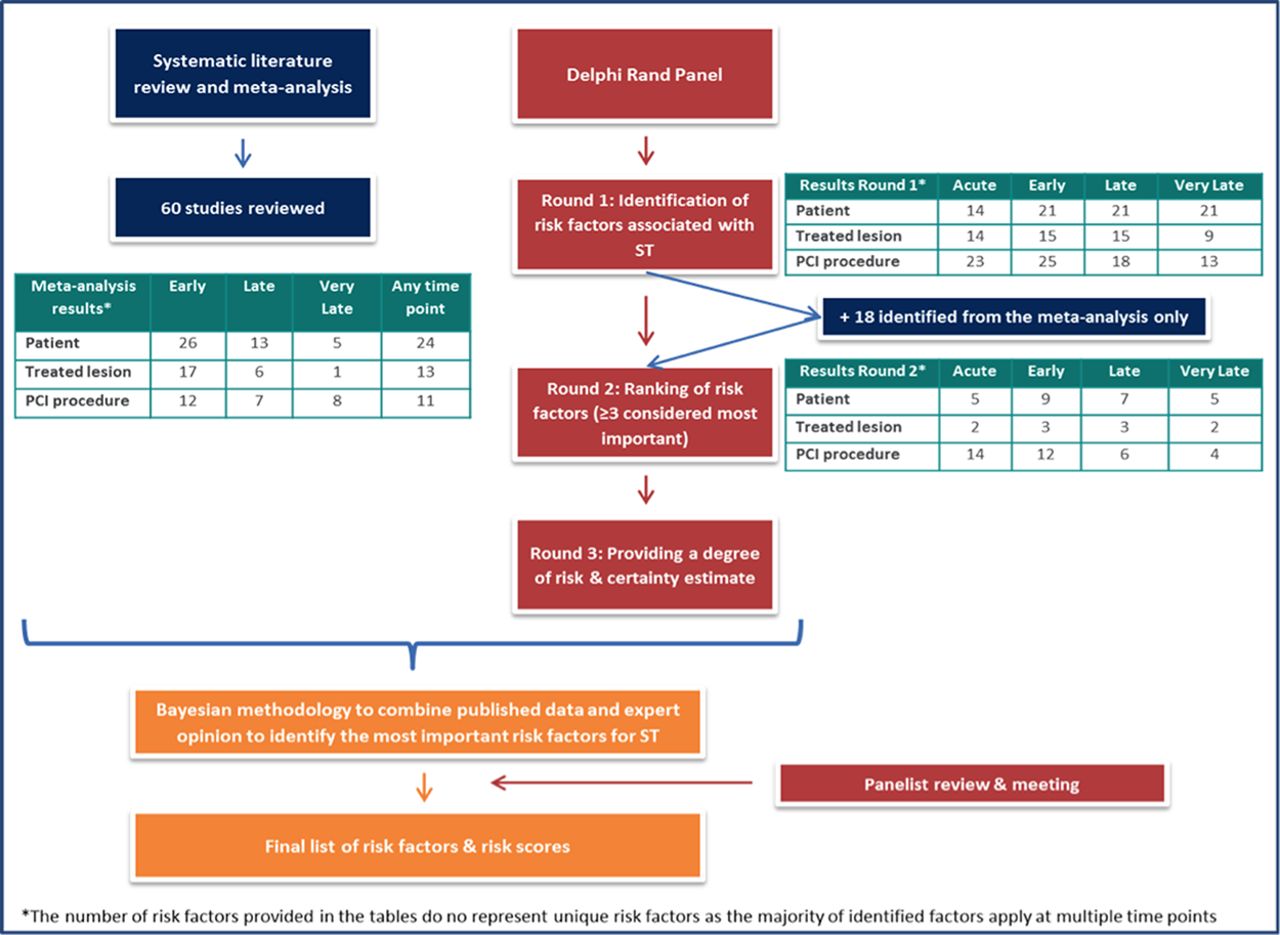
Methods Two research methods were used to identify risk factors for acute (within 24 h), early (within 30 days), late (30 days to 1 year) and very late (more than 1 year after PCI) ST and their associated odds ratios (ORs). This included a systematic literature review and meta-analysis of studies that met certain pre-defined criteria, and a modified Delphi RAND panel to gain expert opinion from eight experienced interventional cardiologists (Figure 1).
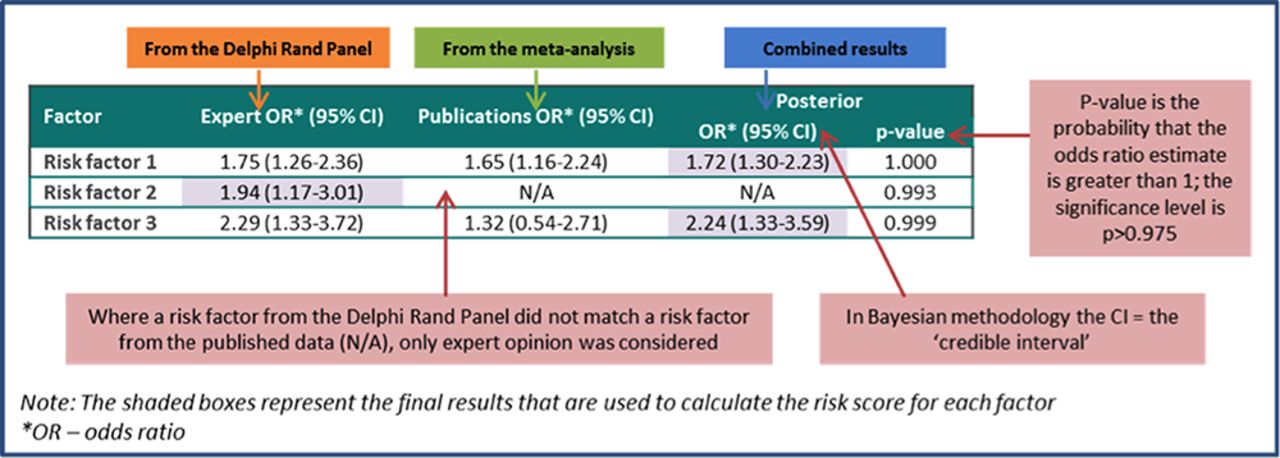
A Bayesian model was used to combine the results of both methods to produce a list of risk factors for each time point with associated ORs and confidence intervals (CIs) (Figure 2).
{kind=link}
{kind=link}
The risk scores were validated by applying them to patient level data from the TRITON-TIMI 38 study and the discriminatory power was tested by developing receiver operator characteristic (ROC) curves for each time point. The ability of the risk scores to predict ST was tested using the Hosmer-Lemeshow goodness-of-fit test.
Results In total, 20 risk factors (9 patient-, 3 lesion- and 8 PCI procedure-related) were found to significantly influence the risk of developing ST. The combined ORs with CIs for some of the risk factors common to all time points are shown in Table 1 below.
The final weighted risk scores, divided into patient-, treated lesion- and PCI procedure-related factors ranged from 0 to 22, 0 to 22 and 0 to 20 for acute, early and late ST respectively. When applied to the patient cohort within the TRITON-TIMI 38 study, the related risk of ST was 0–1.53%, 0–3.85% and 0–0.96% for acute, early and late ST respectively. Model discrimination, measured by area under the ROC curve, was 0.60 (95% CI 0.54–0.67, p = 0.0028) for acute ST, 0.67 (0.61–0.73, p < 0.0001) for early ST and 0.66 (0.58–0.73, p < 0.0001) for late ST, indicating good discriminatory power for all 3 risk scores.
Conclusions In conclusion, published data were combined with expert opinion to produce a weighted scoring system to predict the risk of acute, early, late and very late ST following PCI. This will be assessed prospectively in clinical practice. Use of such a tool will be invaluable in combination with established bleeding risk scores to tailor the potency and duration of antiplatelet therapy in patients undergoing PCI.
- Stent thrombosis
- Risk score
- Delphi RAND