Article Text

Abstract
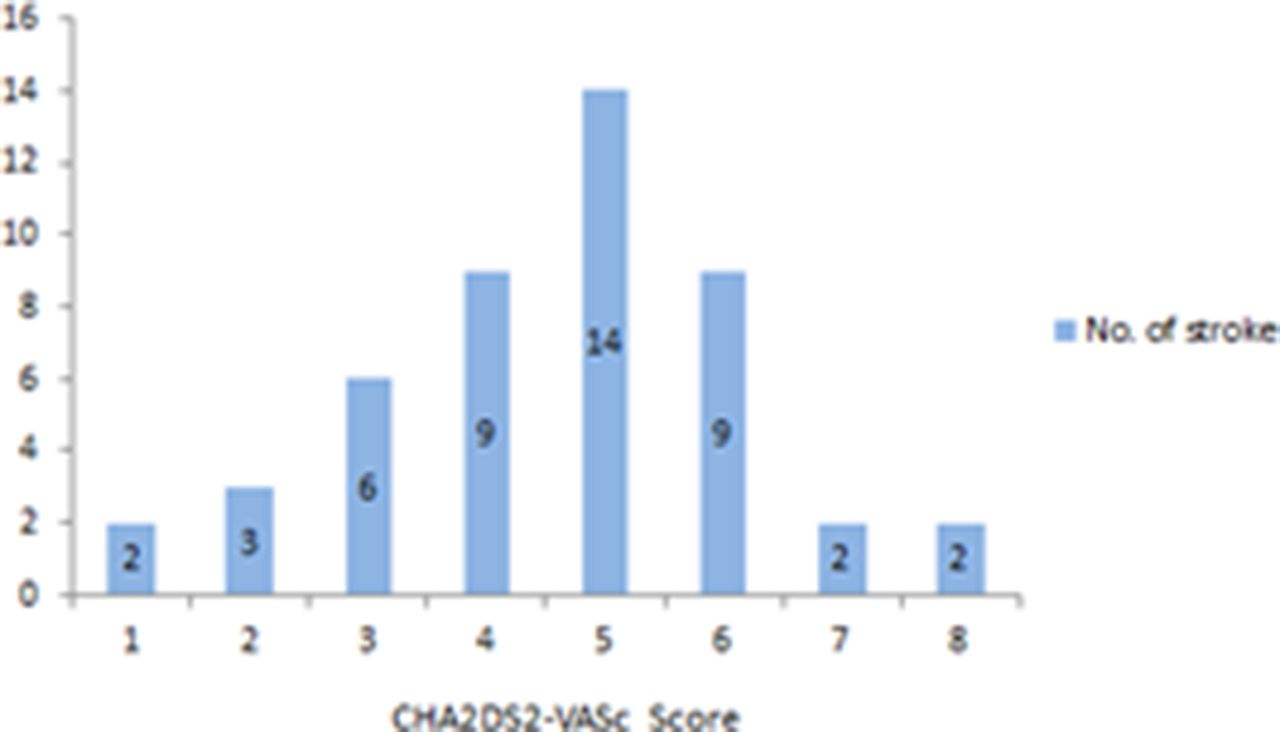
Aim To improve an appropriate use of antithrombotic therapy in atrial fibrillation (AF) on the basis of the presence (or absence) of stroke risk factors (based on CHA2DS2VASc score) as per ESC guideline.
Method This was a retrospective audit and data was obtained from the health record department on the total number of stroke admissions in 2012. A proforma based on the ECS guide was created and used to collect data from those that were coded as having a diagnosis of AF alongside the CVA.
Results There were a total of 389 admissions with stroke in 2012 and 108 of these had a diagnosis of AF.29.9% of which were a new diagnosis AF at the time of admission.
Of those who were known to have AF only 30.9% were anti-coagulated with Warfarin (W) despite all having a CHADS VASC score of 1 or more.46.8% of those had no documentation on the reason for the omission of anticoagulants.3 patients had a stroke while awaiting the initiation of W.
For those on W, 46.2% of those with an ischaemic stroke had a sub-therapeutic INR at the time of admission.
The time in therapeutic range for the patients on W was calculated using the Rosendaal method. This demonstrated that 64.7%of all the patients on W had a TTR below 60%.

{kind=link}
{kind=link}
There were no patients on Novel Oral Anticoagulants (NOAC) in our audit.
Conclusion The majority of patients with known AF were not on W despite > 95 % having a CHADS VASC score greater than 1. Those who were on W had poor INR control. 3 patients had a stroke while waiting for initiation of W. We believe that the risks of AF still needs to be highlighted and the use of NOACS in this cohort would have reduced stroke rate considerably.
- Atrial fibrillation
- antithrombotic
- stroke