Article Text

Abstract
Objective We studied in European adolescents (i) the association between cardiorespiratory fitness and ideal cardiovascular health as defined by the American Heart Association and (ii) whether there is a cardiorespiratory fitness threshold associated with a more favourable cardiovascular health profile.
Methods Participants included 510 (n=259 girls) adolescents from 9 European countries. The 20 m shuttle run test was used to estimate cardiorespiratory fitness. Ideal cardiovascular health was defined as meeting ideal levels of the following components: four behaviours (smoking, body mass index, physical activity and diet) and three factors (total cholesterol, blood pressure and glucose).
Results Higher levels of cardiorespiratory fitness were associated with a higher number of ideal cardiovascular health components in both boys and girls (both p for trend ≤0.001). Levels of cardiorespiratory fitness were significantly higher in adolescents meeting at least four ideal components (13% higher in boys, p<0.001; 6% higher in girls, p=0.008). Receiver operating characteristic curve analyses showed a significant discriminating accuracy of cardiorespiratory fitness in identifying the presence of at least four ideal cardiovascular health components (43.8 mL/kg/min in boys and 34.6 mL/kg/min in girls, both p<0.001).
Conclusions The results suggest a hypothetical cardiorespiratory fitness level associated with a healthier cardiovascular profile in adolescents. The fitness standards could be used in schools as part of surveillance and/or screening systems to identify youth with poor health behaviours who might benefit from intervention programmes.
Statistics from Altmetric.com
Introduction
Cardiorespiratory fitness is an important marker of cardiovascular health already in children and adolescents.1 Longitudinal studies indicate that higher levels of cardiorespiratory fitness in childhood and adolescence are associated with a healthier cardiovascular profile2 and with a reduced risk of myocardial infarction later in life.3 Despite cardiovascular disease (CVD) events occurring most frequently during or after the fifth decade of life, the precursors of CVD seem to have their origin in childhood and adolescence.4 Therefore, establishing health-related cardiorespiratory fitness standards for adolescents can be useful to identify the target population for primary CVD prevention as well as for health promotion policies.
Several attempts have been made in order to determine the cardiorespiratory fitness level associated with a healthier cardiovascular profile in children and adolescents.5–14 However, it is rare for paediatricians, physical education teachers or other health agents to measure cardiorespiratory fitness when evaluating present and future cardiovascular health in youth.
The American Heart Association (AHA) released in 2010 a set of seven cardiovascular health components for youth and adults to describe ideal cardiovascular health.15 Data from the Cardiovascular Risk in Young Finns Study showed that children with a higher number of ideal cardiovascular health components had a reduced risk for hypertension, metabolic syndrome, high levels of low-density lipoprotein cholesterol and high-risk carotid intima-media thickness 21 years later in adulthood.16 The concept of ideal cardiovascular health has also been inversely associated with aortic intima-media thickness and the incidence of CVD,17 and directly associated with aortic elasticity in adolescents.18
The Healthy Lifestyle in Europe by Nutrition in Adolescence (HELENA) study is a multicentre, cross-sectional study performed in nine European countries primarily designed to obtain reliable and comparable data on nutrition and health-related parameters of a relatively large sample of European adolescents aged 12.5–17.5 years.19 The HELENA study collected data on the components included in the ideal cardiovascular health concept,15 thus providing a great opportunity to (i) study the association between cardiorespiratory fitness and ideal cardiovascular health in European adolescents, and to (ii) examine whether there is a cardiorespiratory fitness threshold associated with a more favourable cardiovascular health profile.
Methods
Study participants
The HELENA study was conducted from 2006 to 2007 in 10 European cities (hereafter called centres) from 9 countries.19 The HELENA study sample comprised 3528 boys and girls aged 12.5–17.5 years with valid data for gender and body mass index (BMI). Blood sampling was randomly performed in one-third of the recruited adolescents (n=1089).
This study comprised adolescents who had complete data on (i) cardiorespiratory fitness and (ii) the components included in the ideal cardiovascular health concept.15 A total of 510 (n=251 and 259, boys and girls, respectively) participants were finally included into the present study. There were no differences in the study key characteristics (ie, age, sex distribution, weight and height, and cardiorespiratory fitness) between the current study sample and the original HELENA sample (n=3528, all p>0.1).
Cardiorespiratory fitness
Cardiorespiratory fitness was assessed by the 20 m shuttle run test.20 Participants were required to run between two lines 20 m apart, while keeping the pace with audio signals emitted from a pre-recorded CD. The initial speed was 8.5 km/h, which was increased by 0.5 km/h per minute (1 min equal one stage). Participants were instructed to run in a straight line, to pivot on completing a shuttle and to pace themselves in accordance with the audio signals. The test was finished when the participant failed to reach the end lines concurrent with the audio signals on two consecutive occasions. Otherwise, the test ended when the subject stopped because of fatigue. We estimated the maximum oxygen consumption (VO2max, mL/kg/min) from the 20 m shuttle run test scores using the equation reported by Leger et al.21
Ideal cardiovascular health
The ideal cardiovascular health index and its different components were calculated as outlined by AHA15 using the cut-off values for adolescents.
Health behaviours
Data on smoking were collected via self-reported questionnaires. Adolescents who reported that they had never smoked were categorised as having an ideal smoking status and those who reported having smoked one or more cigarettes were categorised as presenting a non-ideal smoking status.
Height and weight were measured, and BMI calculated as weight (in kg) divided by height (in m2). BMI z-score and BMI categories were derived using British 1990 Growth Reference Data from the Child Growth Foundation.22 ,23
Physical activity was assessed by a self-report questionnaire.24 Adolescents who did not reach 60 min of moderate to vigorous intensity physical activity every day were classified as having a non-ideal physical activity level.
Diet: The HELENA-Dietary Assessment Tool (HELENA-DIAT) was used to assess dietary intake and food consumption.25 It is a self-reported 24 h dietary recall assessment tool based on six meal occasions. Participants completed the HELENA-DIAT in two non-consecutive days according to a standardised protocol. The German Nutrient Database was used to analyse the dietary data. The Multiple Source Method provided by the German Institute of Human Nutrition Potsdam-Rehbrücke as web-based programme package was used to account for within-person variation in the 24 h dietary recalls (https://nugo.dife.de/msm/). All dietary indicators described below have been scaled on a total daily energy intake of 2000 kcal as indicated in the ideal cardiovascular health calculations protocol.15
We classified adolescents as having an ideal fruit and vegetable consumption if they consumed at least 400 g of fruits and vegetables (sum of both) per day.26 Adolescents who consumed at least 28 g of fish or fish products per day were classified as having ideal fish consumption. Adolescents who consumed at least 1.1 g of fibre per 10 g of carbohydrates were classified as having ideal fibre consumption. Those who consumed <1500 mg of sodium per day were classified as having ideal sodium intakes. Adolescents who consumed 145 mL or less of soft drinks per day were classified as having ideal soft drink consumption. The calculation of the 145 mL sugar-sweetened beverages was obtained via the ‘oz’ unit that was included in the original recommendation: 450 kcal (36 oz) per week=28.350* 36/7 g per day. Intake goals are expressed for a 2000 kcal diet and have been scaled accordingly for other levels of calorie intake. Adolescents who had at least four of these five ideal diet components were categorised as having an ideal healthy diet, and adolescents with 0–3 ideal diet components were classified as having a non-ideal healthy diet.
Health factors
Blood analysis: For the determination of total cholesterol and glucose levels, venous blood samples were drawn after an overnight fast. In adolescence, levels of total cholesterol have been defined as ideal <4.40 mmol/L (<170 mg/dL) or non-ideal ≥4.40 mmol/L (≥170 mg/dL).15 Fasting serum glucose concentrations were analysed enzymatically and classified as ideal <5.6 mmol/L (<100 mg/dL) or non-ideal ≥5.6 mmol/L (≥100 mg/dL).15
Blood pressure: It was measured twice after being seated in a quiet room for 10 min with their back supported and feet on the ground. Two blood pressure readings were taken with a 10 min interval of quiet rest. The lower value of the two measurements was used in the analysis to classify blood pressure status in adolescence as ideal (systolic blood pressure <90th centile and diastolic blood pressure <90th centile) or non-ideal (systolic blood pressure ≥90th centile or diastolic blood pressure ≥90th centile).15 All centile-based threshold limits are sex-specific and age-specific from the entire HELENA study sample.
Indices of the ideal cardiovascular health
From the individual health behaviours and factors described above, we generated the corresponding AHA indices (ie, ideal health behaviours index, ideal health factors index and the ideal cardiovascular health index). The ideal cardiovascular health index corresponds to the number of ideal health behaviours (0–4) and factors (0–3) achieved by the participant. In analyses, we used the ideal cardiovascular health index as a continuous variable (from 0 to 7) as done elsewhere,16 ,18 as well as categorised as presence of at least four ideal components (ideal cardiovascular health vs non-ideal cardiovascular health).18
Statistical analysis
The data are presented as means (SD) unless otherwise stated. Differences on cardiorespiratory fitness levels between ideal and non-ideal cardiovascular health components were assessed by analysis of covariance (ANCOVA) with cardiorespiratory fitness as a dependent variable, cardiovascular health component (ideal vs non-ideal) entered as a fixed factor, age as a covariate and centre as a random factor. The association of cardiorespiratory fitness with ideal cardiovascular health index, as well as with ideal health behaviours and factors separately, was assessed by ANCOVA as explained above.
We determined the cardiorespiratory fitness level associated with having at least four ideal components by receiver operating characteristic (ROC) curve.27 The area under ROC curve (AUC) and 95% CI were calculated. Finally, binary logistic regression was used to study the relationship between cardiorespiratory fitness and ideal cardiovascular health score, adjusting for age and centre. Analyses were conducted for boys and girls separately. All analyses were performed using the Statistical Package for Social Sciences (SPSS, V.20.0 for Windows; SPSS, Chicago), and the level of significance was set at α=0.05.
Results
Table 1 shows the characteristics of the study participants. None of the adolescents had all seven ideal cardiovascular health components, except one girl. Simultaneous presence of at least four ideal components was found in 87% of boys and 84% of girls.
Characteristics of the study participants
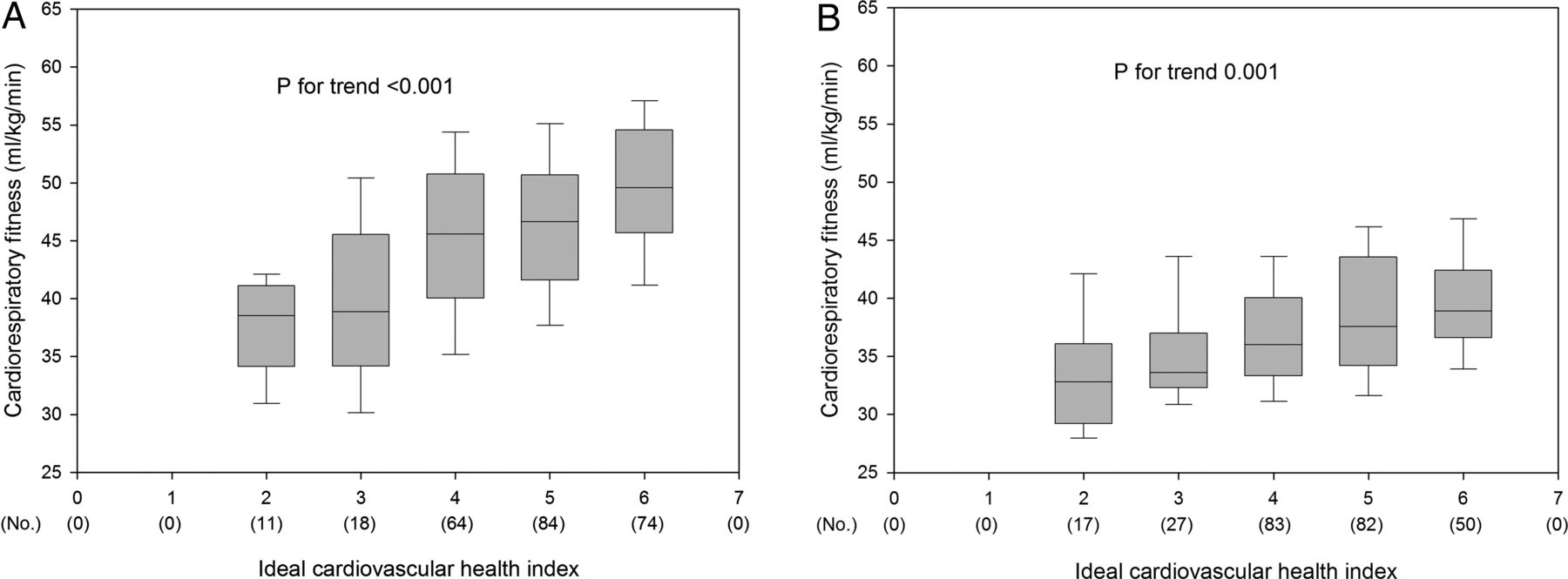
Higher levels of cardiorespiratory fitness were associated with a higher number of ideal cardiovascular health components in both boys (p for trend <0.001) and girls (p for trend 0.001) (figure 1). Levels of cardiorespiratory fitness were significantly higher in adolescents meeting at least four ideal components (13% higher in boys, p<0.001; 6% higher in girls, p=0.008) compared with those meeting less than four ideal components (table 2). Higher levels of cardiorespiratory fitness were associated with a higher number of ideal health behaviours (p for trend <0.001 in both boys and girls), and with a higher number of ideal health factors in boys (p for trend 0.001) but not in girls (p for trend 0.291) (figure 2). Levels of cardiorespiratory fitness were similar between ideal versus non-ideal glucose or smoking groups in both boys and girls (table 2).
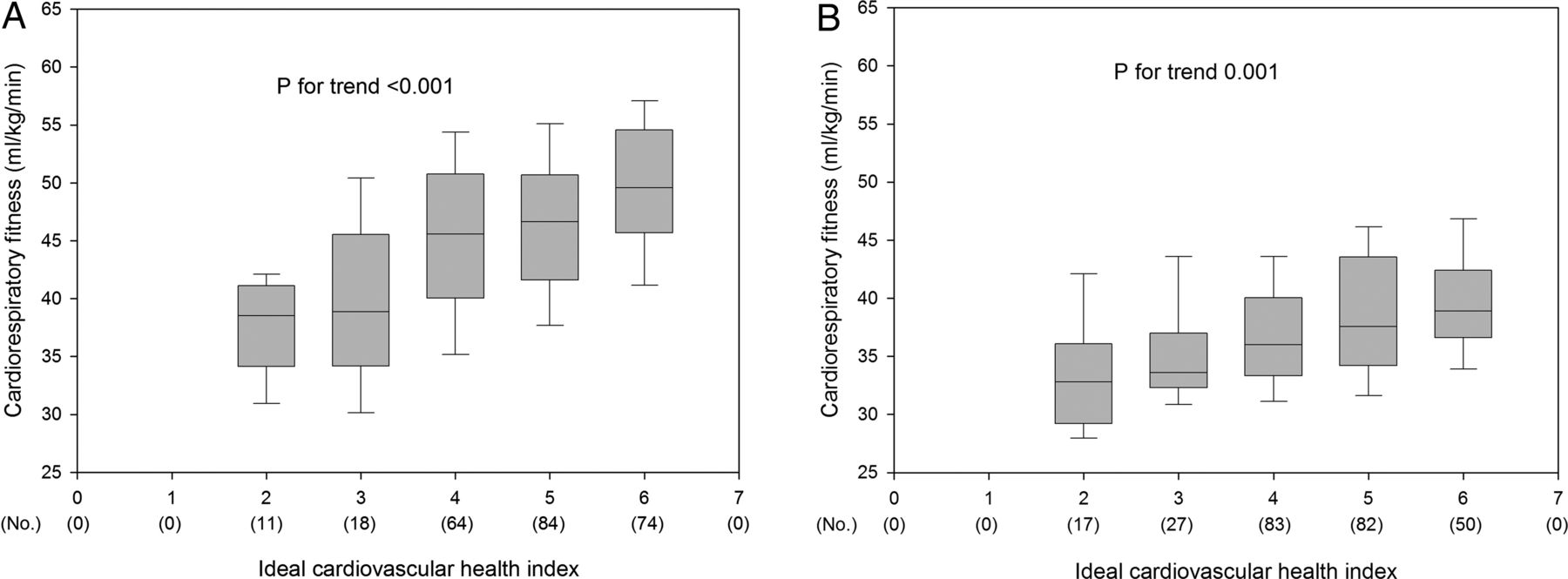
Association between cardiorespiratory fitness and ideal cardiovascular health index in European adolescents from the Healthy Lifestyle in Europe by Nutrition in Adolescence study. (A) Boys; (B) girls. No., frequency.
Cardiorespiratory fitness (mL/kg/min) mean and SE estimates by ideal cardiovascular health components in European adolescents (both boys and girls) from the HELENA study

Levels of cardiorespiratory fitness across ideal health behaviours (smoking, body mass index, physical activity and diet) and factors (total cholesterol, blood pressure and plasma cholesterol) score in European adolescents from the Healthy Lifestyle in Europe by Nutrition in Adolescence study. (A and C) Boys; (B and D) girls. No., frequency.
ROC analysis showed a significant discriminating accuracy of cardiorespiratory fitness in identifying a favourable (presence of at least four ideal metrics) ideal cardiovascular health in boys (AUC 0.805, 95% CI 0.726 to 0.883, p<0.001) and in girls (AUC 0.694, 95% CI 0.605 to 0.784, p<0.001) (figure 3). The cardiorespiratory fitness cut-off levels associated with having at least four ideal components were 43.8 mL/kg/min (optimal pair of sensitivity and specificity 68.9 and 82.8, respectively) in boys and 34.6 mL/kg/min (optimal pair of sensitivity and specificity 74.9 and 59.1, respectively) in girls. Logistic regression analysis showed that boys with levels of cardiorespiratory fitness above 43.8 mL/kg/min had higher OR of having at least four ideal components compared with those with cardiorespiratory fitness levels below this value (OR, 6.437; 95% CI 2.580 to 16.057; p<0.001). Girls with cardiorespiratory fitness levels above 34.6 mL/kg/min had higher OR of having at least four ideal components than those with cardiorespiratory fitness levels below this value (OR, 2.756; 95% CI 1.316 to 5.775; p=0.007). The results did not change when a different equation to estimate cardiorespiratory fitness was used.21

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curve summarising the potential of cardiorespiratory fitness to identify ideal cardiovascular health status (simultaneous presence of at least four ideal components) in European adolescents from the Healthy Lifestyle in Europe by Nutrition in Adolescence study. (A) Boys; (B) girls. AUC, area under the curve.
Discussion
The findings of the present study indicate that cardiorespiratory fitness is positively associated with the ideal cardiovascular health index as determined by AHA in European adolescents. Furthermore, the current study identified a hypothetical cardiorespiratory fitness threshold associated with a more favourable cardiovascular health profile, which seems to be more discriminative for boys than for girls.
Interestingly, the observed cut-off levels for cardiorespiratory fitness obtained in adolescents participating in the HELENA study are similar to those published previously by other studies conducted in past generations of children and adolescents from the USA9 and different European countries8 ,10 ,11 ,12 ,13 with diverse environmental, cultural and social factors. Of note is that previous studies used less comprehensive health indices than the one used in the present study and did not use behaviour-related components. Moreover, the test protocols as well as the prediction equations to estimate cardiorespiratory fitness also differed across studies. Similarities among the study results however reinforce the existence of a cardiorespiratory fitness threshold associated with cardiovascular health in youth. Taken together present and previous findings (see table 3), the estimated cardiorespiratory fitness levels for optimum cardiovascular health in children and adolescents seem to fall between 40 and 47 mL/kg/min for boys and between 35 and 42 mL/kg/min for girls.
Health criterion-reference standards for cardiorespiratory fitness in children and adolescents
Schools are a convenient setting to promote a healthy lifestyle among young populations and could collect this information to encourage children to be more physically active to achieve and go beyond the health-related cardiorespiratory fitness thresholds. Moreover, whereas the information given by the assessment of cardiorespiratory fitness in the schools is not diagnostic, it could be used as part of surveillance and/or screening systems to identify youth with poor health behaviours who might benefit from intervention programmes. As such, this has potentially clinical and public health implications. Unfortunately, despite the relevant information provided by a relatively simple assessment of cardiorespiratory fitness, such data rarely become available or are not used by public health and clinical practitioners for purposes of health promotion or disease prevention.9 Physicians have access to measures of CVD risk factors such as fasting blood samples and blood pressure; however, some of these procedures are invasive, expensive and not suitable for CVD risk screening among large populations of children and adolescents. The origins of CVD are found in childhood,4 and cardiorespiratory fitness levels at childhood and adolescence are associated with cardiovascular health during these years and later in life;1 ,2 thus lifestyle modification focused on enhancing physical activity and increasing fitness might help improve their cardiovascular health.
Meeting all seven ideal cardiovascular components is the ultimate target, yet we observed that cardiorespiratory fitness levels were already higher (13% and 6% in boys and girls, respectively) when at least four ideal cardiovascular health components were met. In the present study, we observed that the likelihood of having four or more ideal cardiovascular health components was 6.4 and 2.7 times higher in boys and girls, respectively, meeting the health-related cardiorespiratory fitness levels (43.8 mL/kg/min in boys and 34.6 mL/kg/min in girls) than in those not meeting these levels. We previously showed similar results in Spanish adolescents12 as well as in Swedish and Estonian children aged 9–10 years.8 Children who did not meet the health-related levels (42.1 and 37.0 mL/kg/min in boys and girls, respectively) were three times more likely to have a lower CVD risk score compared with those who did not meet the standards.8 These findings are also similar to those observed in the National Health and Nutrition Examination Survey (NHANES).9 Lobelo et al9 showed that higher levels of cardiorespiratory fitness were associated with a healthier cardiovascular profile in adolescents. Moreover, they showed that boys who met the fitness levels were between four and five times more likely to have a low CVD risk compared with those who did not meet the standards. Comparable results were found (i) in 4500 children and adolescents from Denmark, Estonia, Norway and Portugal, who were tested as part of the European Youth Heart Study (EYHS);10 (ii) in 16 619 English children from the SportsLinx Project11 and (iii) in 450 Portuguese adolescents.13 All the aforementioned studies calculated mathematically the cardiorespiratory fitness levels associated with a more favourable cardiovascular profile, which turned out to be similar to the health-related cardiorespiratory fitness thresholds suggested by worldwide recognised organisations such as the European Group of Pediatric Work Physiology5 or the Cooper Institute for Aerobics Research6 ,7 (table 3).
Cardiorespiratory fitness is influenced by several factors, including genetics. It might be argued that there may be some shared inherent qualities for both better fitness and improved cardiovascular health; however, recent reports suggest that this assumption should be revisited.28 Other facts such as sex, age, body composition and health status are known to influence cardiorespiratory fitness level, yet its principal modifiable determinant is habitual physical activity.29 Findings from exercise-based intervention studies indicate that cardiorespiratory fitness levels can be improved in youth through aerobic training.29 Moreover, aerobic exercise interventions have shown to improve blood lipid profile, body fatness and other cardiometabolic risk factors in youth.30 School-based interventions to improve physical activity participation among youths who fail to meet the health-related cardiorespiratory fitness levels are warranted as part of programmes aiming to improve youth's cardiovascular health.
Limitations of this study include its cross-sectional design, which precludes definitive causal attributions. Another limitation is the use of a questionnaire to assess physical activity, which was previously pilot-tested and validated.24 The HELENA study assessed physical activity by both questionnaire and accelerometry. Nevertheless, results were materially the same when using data from accelerometry (data not shown). In addition, the difficulty of accurate assessment of dietary intake must also be considered as a potential limitation, especially among adolescents, where misreporting is a common problem.19 We only had two non-consecutive days 24 h dietary recalls. When considering the daily fish intake, this might lead to false non-consumers, that is, adolescents consuming fish but not on these two 24 h recall days. It should also be noted that the formation of the ideal cardiovascular health score relies on the use of binary variables and on the assumption that all health behaviours and factors contained in this index contribute the same to the final score.
In conclusion, the present study provides health-related cardiorespiratory fitness thresholds associated with a more favourable cardiovascular health profile in youth.
Key messages
-
What is known on this subject?
-
Cardiorespiratory fitness is a marker of cardiovascular health during childhood and adolescence, and a predictor of the cardiovascular profile later in life.
-
What might this study add?
-
The present study identifies a cardiorespiratory fitness threshold associated with a favourable cardiovascular health profile in adolescents.
-
How might this impact on clinical practice?
-
The fitness thresholds could be used by paediatricians, physical education teachers or other health agents to measure as part of surveillance and/or screening systems to identify youth with poor health behaviours who could benefit from intervention programmes.
Acknowledgments
We thank the children and adolescents who participated in the study and their parents and teachers for their collaboration. We also acknowledge the members involved in fieldwork for their efforts, particularly Anke Carstensen and Petra Pickert for their work in the blood sample laboratory.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Collaborators HELENA Project Group: list included in online supplementary appendix.
-
Contributors JRR wrote the manuscript and performed the statistical analysis. IH, MC-G, EGA, IL, AM, GV-R, AP, YM, MG-G, AM, KW, DM, AK, MS, LAM, MJC and FBO contributed to the interpretation and discussion of the results. All authors contributed to the interpretation and discussion of the results, and critically revised the drafted manuscript.
-
Funding The HELENA project was supported by the European Community Sixth RTD Framework Programme (contract FOOD-CT-2005-007034). The data for this study were gathered under the aegis of the HELENA project, and further analysis was additionally supported by the Spanish Ministry of Economy and Competitiveness (grants RYC-2010-05957 and RYC-2011-09011), the Spanish Ministry of Health: Maternal, Child Health and Development Network (grant RD08/0072) and the Fondo Europeo de Desarrollo Regional (MICINN-FEDER).
-
Disclaimer The content of this paper reflects the author’s views alone, and the European Community is not liable for any use that may be made of the information contained herein.
-
Competing interests None.
-
Patient consent: All adolescents and their parents or guardians signed an informed written consent before being enrolled in the study.
-
Ethics approval The corresponding local Human Research Review Committees of the centres involved approved the study protocol.
-
Provenance and peer review Not commissioned; externally peer reviewed.