Article Text

Statistics from Altmetric.com
Cardiac resynchronization therapy (CRT) is recommended in patients with heart failure, a reduced left ventricular ejection fraction (≤35%) and a wide QRS complex on electrocardiography (ECG). Evidence is strongest for improved clinical outcomes with CRT therapy in patients with a left bundle branch block (LBBB) on ECG leading to a Class I recommendation for CRT in these patients. However, current guidelines also recommend CRT in heart failure patients with a low ejection fraction and a QRS duration greater than 150 milliseconds (Class IIa) or between 120 and 150 milliseconds (Class IIb), regardless of QRS morphology, depending on severity of heart failure symptoms.
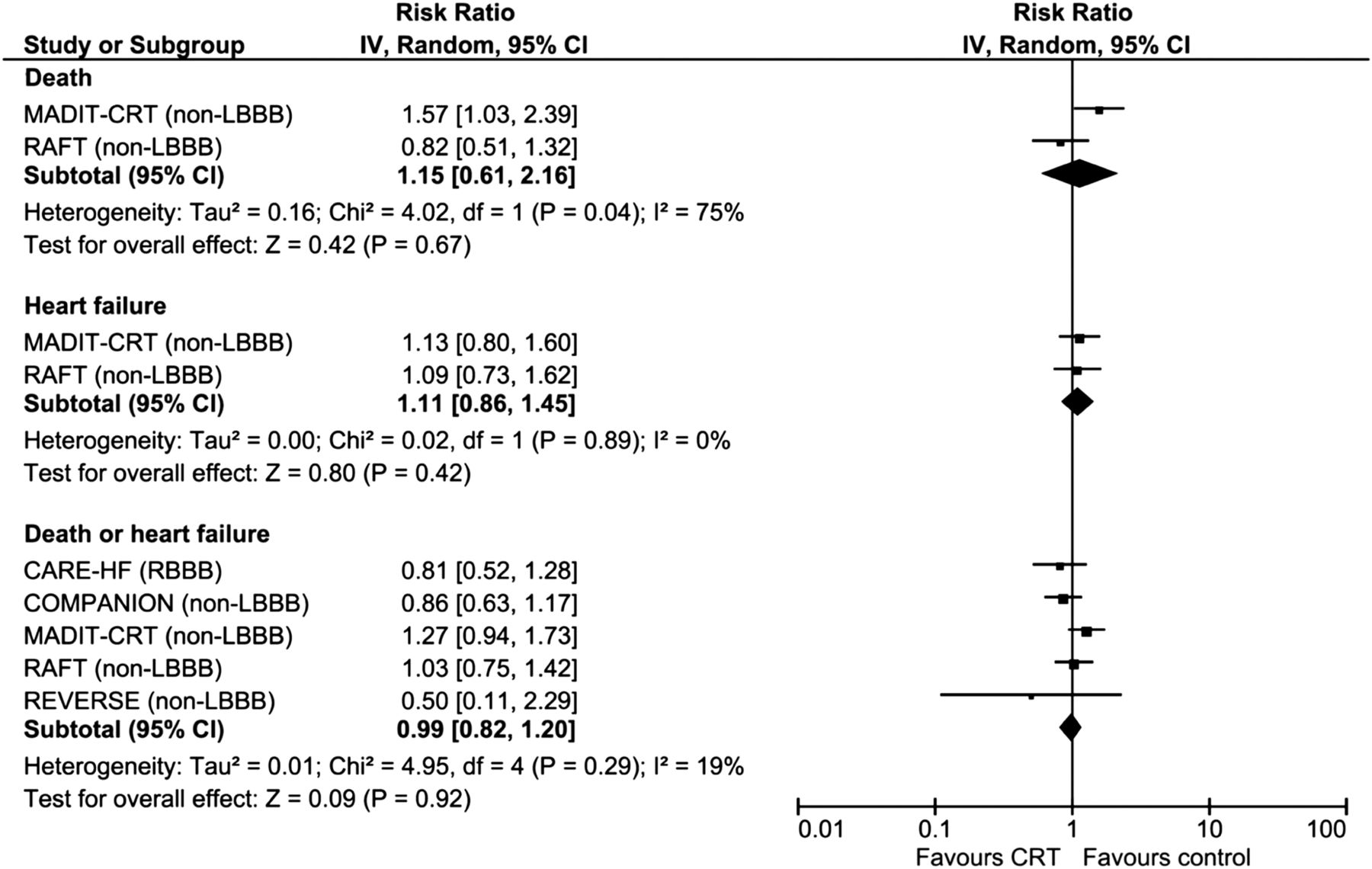
In order to further define the potential benefit of CRT in heart failure patients with a non-LBBB pattern on ECG, Cunnnington and colleagues (see page 1456) performed a meta-analysis of randomized controlled trials. Based on 1766 subjects (27% of the total) with a non-LBBB QRS pattern in the 5 studies included in this meta-analysis, CRT was not associated with a reduction in death or heart failure hospitalization in this subgroup of patients (figure 1).

Risk of adverse outcomes among patients with non-left bundle branch block (non-LBBB) QRS morphology who did or did not receive cardiac resynchronisation therapy (CRT).
In a provocative accompanying editorial, Cleland and Freemantle (see page 1441) argue that this meta-analysis “does not exclude a 39% reduction in mortality with CRT in such patients and does not provide statistical evidence of heterogeneity of the effect of CRT amongst patients with different QRS morphologies. This analysis should not be used to deny patients a potentially highly beneficial treatment.” This editorial also discusses the possible mechanisms by which CRT improves ventricular function and clinical outcomes, suggesting that different mechanisms may be operative in different patients or at different points in the disease course. They conclude: “Patients and the scientific community should welcome more information on the effects of CRT but the balance of clinical evidence does not favour withholding CRT when QRS duration is >140 msec regardless of QRS morphology. Trials in patients with QRS duration between 120–140 msec have been proposed. There are many other more important questions that need to be addressed, including whether CRT-D is superior to CRT or whether CRT is effective in the large proportion of patients with heart failure who have atrial fibrillation.”
In adults with severe aortic stenosis (AS), transcatheter valve implantation (TAVI) is an attractive alternative to surgical valve replacement, particular in patients with a high or prohibitive surgical risk. There also has been hope that the transcatheter approach might eventually result in lower total costs and shorter hospital stays; an elusive goal to date. In a comparison of 107 patients discharged early (within 72 hours) after TAVI compared to a propensity matched cohort of patients discharged later, Barbanti and colleagues (see page 1485) found that early discharge was more likely in patients with a prior permanent pacer, no bleeding events, and less severe baseline symptoms. The likelihood of early discharge also increased with each year of TAVI experience at this medical center. However, outcomes after discharge were similar with no significant differences in death or rehospitalization with early versus later discharge after TAVI (table 1). This data suggests the possibility of reducing TAVI costs with early discharge of patients at low risk of post-TAVI complications.
Thirty-day outcomes post-discharge
Exposure to ambient air pollution is estimated to account for 20, 000 to 30,000 excess deaths annually in the USA and Western Europe. The effects of even short term exposure to particulate matter and other air pollution components has led to the concern that the adverse effects of air pollution might be associated with an increased risk of cardiovascular events in pregnant women. Männistö and colleagues (see page 1491) examined the association between air pollution exposure and maternal events near the time of delivery in 223,502 pregnancies in an observational USA cohort. Adverse cardiovascular events occurred in 0.3% of deliveries with a higher odds of cardiovascular events with increasing levels of exposure to nitric oxides and other toxic air pollution species in the 5 to 6 days before delivery (figure 2). These novel findings show that even short-term exposure to low ambient levels of air pollutants is associated with an increase in cardiovascular events during and immediately after labor and delivery. For readers interested in understanding the potential mechanism of the adverse effects of air pollution, the review article by Chin published in Heart earlier this year provides a detailed discussion.1

The odds (99% CIs) of cardiovascular events after exposure to criteria pollutants at delivery day and 1–7 days prior to delivery, single-pollutant models. All results are adjusted for site, maternal age, race/ethnicity, insurance status, smoking during pregnancy and pre-pregnancy body mass index (kg/height in m2). CO, carbon monoxide; NOx, nitrogen oxides; PM10, particulate matter <10 µm in aerodynamic diameter, PM2.5, particulate matter <2.5 µm in aerodynamic diameter, SO2, sulfur dioxide.
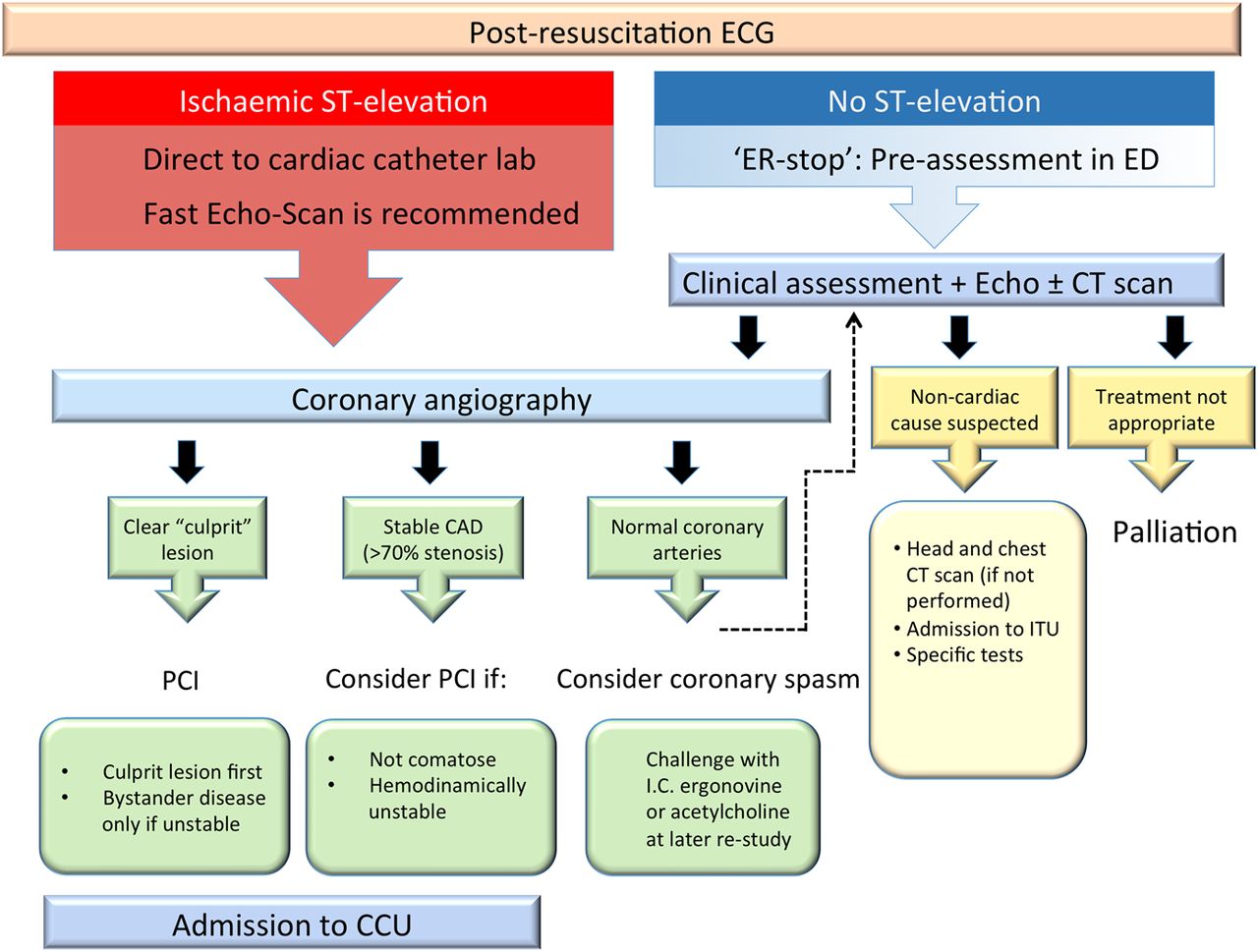
The Education in Heart article in this issue focuses on management of out of hospital cardiac arrest (see page 1505) with detailed flow diagrams and a concise summary of the published evidence supporting current practice (figure 3).

{kind=link}
{kind=link}
{kind=link}
Proposed patient pathway for OOHCA survivors to hospital admission, and management of coronary disease at angiography.
The Image Challenge in this issue (see page 1462) shows an interesting echocardiographic finding in a 15 year old presenting with dyspnea. You can make the diagnosis from the still frame images but the online videos are well worth viewing. Once you see this case, you will recognize this finding easily in your own practice.
Reference
Linked Articles
- Education in Heart
- Editorial
- Heart failure and cardiomyopathies
- Special populations
- Valvular heart disease