Article Text

Statistics from Altmetric.com
Clinical cardiologists are often overwhelmed by the number and complexity of new clinical guidelines published by our professional societies. Heart now publishes frequent short editorials summarizing new guidelines to provide a quick update and highlight key changes. In this issue of Heart, Dr Elliott summarizes the new hypertrophic cardiomyopathy (HCM) guidelines, which include recommendations for placement of an implantable cardiac defibrillator in patients with HCM. (See page 506 figure 1).
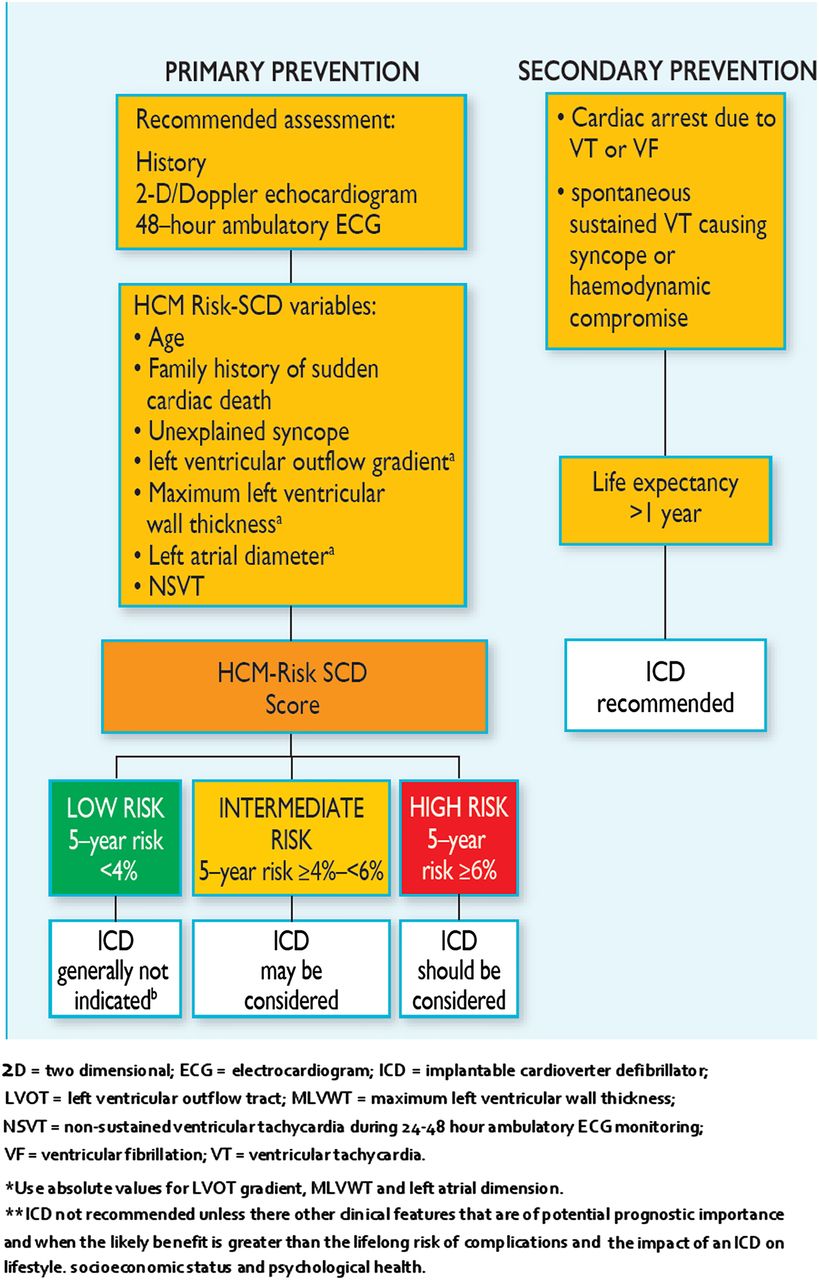
Recommendations for implantable cardioverter defibrillators based on hypertrophic cardiomyopathy (HCM) RISK-SCD score.
The Editor's choice in this issue of Heart focuses on the risk of pregnancy in women with coronary artery disease. Although relatively uncommon, we are likely to see an increased prevalence of this problem with women having children at an older age and with population trends towards an increased prevalence of cardiovascular risk factors, such as diabetes, hypertension and obesity, in younger women. From a multicenter retrospective study at 6 academic medical centers over a 17-year time span, Dr Silversides and colleagues identified 50 pregnancies in 43 women with a diagnosis of coronary atherosclerosis (40%), coronary thrombosis (36%), coronary spasm (12%) or an acute coronary syndrome of unknown etiology. (See page 525) The primary composite outcome occurred in 10% of women – 1 with cardiac arrest resulting in death, 3 with an acute coronary syndrome, and 1 with heart failure. In addition, 18% of women had new or worsening angina, 16% had obstetric complications and 30% of infants suffered adverse fetal or neonatal events table 1.
(TABLE 3 from heartjnl-2014-306676) Timing of adverse maternal cardiac events
In an accompanying editorial, Dr Polewczyk notes that coronary disease is present in about 2% of pregnant women and that cardiovascular conditions account for an increasing number of pregnancy-related deaths. (See page 502) In addition to standard coronary risk factors, physiologic changes during pregnancy may exacerbate coronary disease including a prethrombotic state, vascular dysfunction, physiologic anemia, a lower diastolic blood pressure, and hormonal effects on the vasculature. She comments: “In patients with coronary lesions, these factors may induce anginal pain and even deterioration of cardiac function. Birth-related pain and effort, as well as sudden changes in blood volume and pressure postpartum, may also significantly increase the risk of cardiovascular complications.”
The management of pregnant women with heart disease remains controversial. Specifically, despite an insufficient evidence base, cardiologists and obstetricians often have strong opinions about the optimal mode of delivery. Some experts advocate caesarean section (CS) based on the rationale that this delivery mode is safer. Others recommend vaginal delivery with epidural anesthesia because hemodynamic changes are less severe and there is a lower rate of maternal hemorrhage, infection or thrombosis. In an effort to shed some light on this controversy, Dr Roos-Hesselink and colleagues looked at outcomes in 393 women with planned CS compared to 869 women with planned vaginal delivery in women with heart disease enrolled in the Registry of Pregnancy and Cardiac Disease (ROPAC) study. (See page 530) Emergency CS for obstetric reasons was performed in 13% of those with planned CS and 16% of those with a planned vaginal delivery. Using an intention to treat analysis, “the planned CS group had higher rates of maternal death, 2% versus 0.6% (p=0.018), postpartum heart failure, 8.4% versus 3.9% (p<0.001) and pre-eclampsia, 5.9% versus 2.3% (p=0.001). Fetal outcome was better in the patients who had a planned vaginal delivery, with longer pregnancy duration (p<0.001) and higher birth weight (p<0.001) even after correction (p=0.013)”. This study also found wide geographical variation in the rate of CS, which was related to the number of high risk patients and background rates of CS in each country (figure 2).
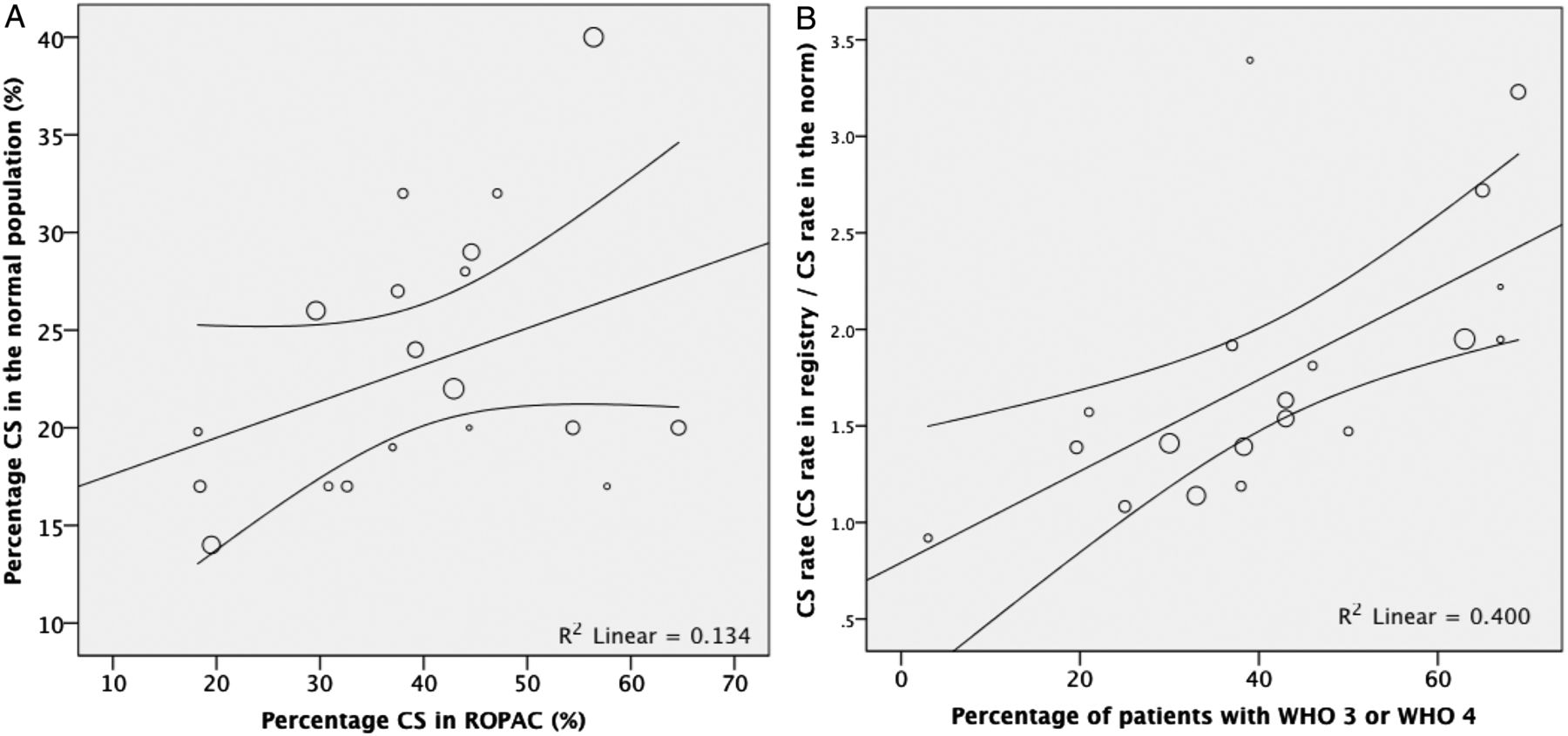
Distribution of the number of caesarean sections performed in countries with their rates in the background population and in high risk patients. Every point represents a country; the size of the points corresponds to the number of subjects included. (A) Distribution of expected (normal) caesarean section rate against caesarean section rate in the Registry of Pregnancy and Cardiac disease (ROPAC). (B) Distribution of caesarean section rate (caesarean section rate in women included in the ROPAC registry divided by the caesarean section rate in the background population) compared with percentage of patients with WHO category 3 or WHO category 4.
Dr Tutarel reminds us that “The current guidelines of the European Society of Cardiology about pregnancy in cardiac disease recommend that the preferred mode of delivery is vaginal, while generally speaking CS is reserved mainly for obstetric indications, with the exception of some maternal cardiac lesions regarded as high risk, like patients on oral anticoagulants in preterm labour, patients with Marfan syndrome and an aortic diameter >45 mm, patients with acute or chronic aortic dissection and those with acute intractable heart failure, in which CS should be considered.” (See page 504) However, this study is not the final answer – “Considering that the planned CS for cardiac reasons group in their study included more high-risk cases with valvular heart disease, cardiomyopathy, worse overall New York Heart Association class and greater anticoagulant use, and also displayed greater maternal mortality, I am not convinced that this group would have the same outcome if vaginal delivery was tried first.” Clearly adequate planning is the key to avoiding adverse outcomes in pregnant women with heart disease. Unfortunately, we still need better data on which cardiac patients benefit from CS compared to vaginal delivery.
The current Education in Heart topic is the clinical use of multimodality imaging in the assessment of dilated cardiomyopathy. (See page 565) with a proposed diagnostic algorithm for evaluation of these patients (figure 3).

{kind=link}
{kind=link}
{kind=link}
Proposed diagnostic imaging algorithm for the aetiologic evaluation of patients with suspected dilated cardiomyopathy (DCM). CAD, coronary artery disease; LGE-CME, late gadolinium enhancement-cardiac magnetic resonance.
The image challenge (See page 552) ask you to select the most appropriate management plan based on the results from an implantable loop recorder in a 64 year old man with palpitations and dizziness.
Linked Articles
- Image challenge
- Editorial
- Editorial
- Special populations
- Editorial
- Special populations
- Education in Heart