Article Text

Abstract
Introduction Physiological cardiac adaptation to regular exercise, including biventricular dilatation and electrocardiographic T-wave inversion (TWI), may create diagnostic overlap with arrhythmogenic right ventricular cardiomyopathy (ARVC). Accurate differentiation between physiological and pathological cardiac remodelling is essential in order to avoid erroneous exclusion from sporting activity or, conversely, sports-related sudden cardiac deaths. The study objectives were to assess the accuracy of diagnostic criteria for ARVC when applied to athletes exhibiting electrocardiographic TWI, and to identify discriminators between physiology and disease.
Methods The study population consisted of athletes with TWI (n = 45), a control group of athletes without TWI (n = 35), and age-matched ARVC patients (n = 35). Subjects underwent ECG, signal-averaged ECG (SAECG), echocardiography, cardiac magnetic resonance imaging (CMRI), Holter monitoring, and exercise testing. Genetic testing was performed on consenting ARVC patients.
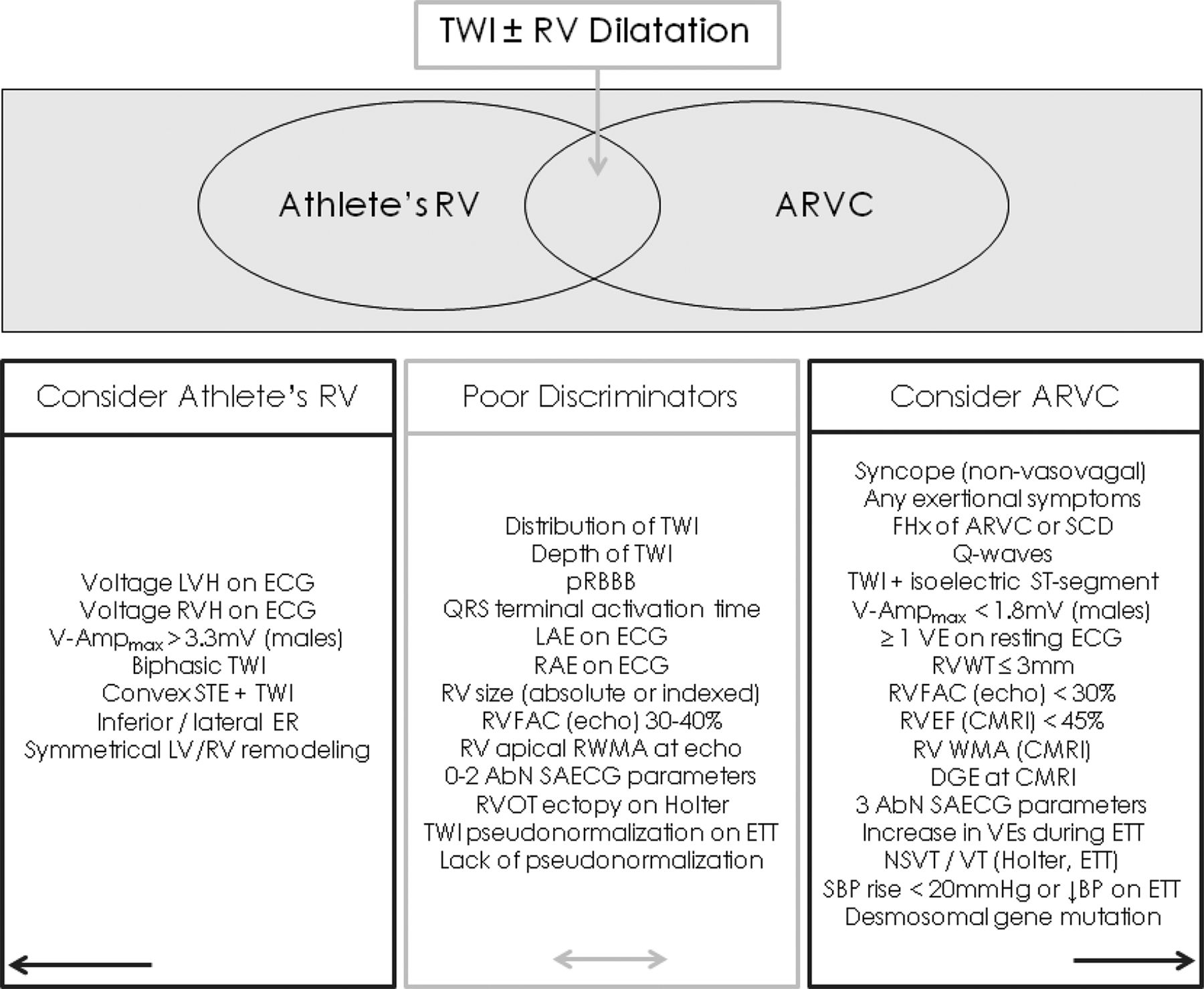
Results There were no electrical, structural, or functional cardiac differences between athletes exhibiting TWI and the control group of athletes without TWI. When athletes were compared with ARVC patients, markers of physiological remodelling included early repolarisation, biphasic TWI, voltage criteria for right ventricular (RV) or left ventricular hypertrophy, and symmetrical cardiac enlargement. Indicators of RV pathology included syncope or adverse family history; Q-waves or precordial QRS amplitudes <1.8 mV; three abnormal SAECG parameters; delayed gadolinium enhancement, RV ejection fraction <45%, or wall motion abnormalities in either ventricle at CMRI; ventricular tachyarrhythmias on Holter monitoring; and symptoms, ventricular tachyarrhythmias, or attenuated blood pressure response during exercise testing. Non-specific parameters that were not useful discriminators between physiological and pathological remodelling included; depth of TWI, distribution of TWI, <3 abnormal SAECG parameters, RV dilatation without wall motion abnormalities, RV outflow tract ectopy on Holter monitoring, and exercise-induced T-wave pseudonormalisation (Tables 1 and 2, Figure 1).
Utility of ECG and SAECG parameters for differentiating physiological and pathological TWI
Utility of echo, CMRI, and exercise parameters for differentiating physiological and pathological TWI

{kind=link}
Clinical differentiators between athletic right ventricular remodelling and ARVC
Conclusions Certain components of the ARVC Task Force criteria are non-specific when applied to athletes, since training-induced electrical and structural remodelling may closely resemble pathology. Additional discriminators are required to avoid erroneous diagnosis in such cases. Comprehensive evaluation using widely available techniques can effectively differentiate phenotypically borderline cases.
- Arrhythmogenic right ventricular cardiomyopathy
- diagnosis
- exercise