Article Text

Abstract
Introduction TTN truncating variants (TTNtv) cause severe dilated cardiomyopathy (DCM), but sometimes occur in healthy individuals, posing significant challenges for the interpretation of these variants in an era of accessible genome sequencing. The mechanism by which TTNtv impact clinical outcomes is poorly understood.
Methods Here, we integrated the power of quantitative cardiac MRI and capacity of next generation sequencing to assess the relationship between TTN genotype and cardiac phenotype. We sequenced TTN in 4,440 subjects including 308 healthy volunteers, 3,603 Framingham Heart Study (FHS) and Jackson Heart Study (JHS) participants, 374 prospective, unselected DCM cases and 155 end-stage retrospective DCM cases including 84 for whom left ventricular (LV) tissue was available for RNA and protein studies.
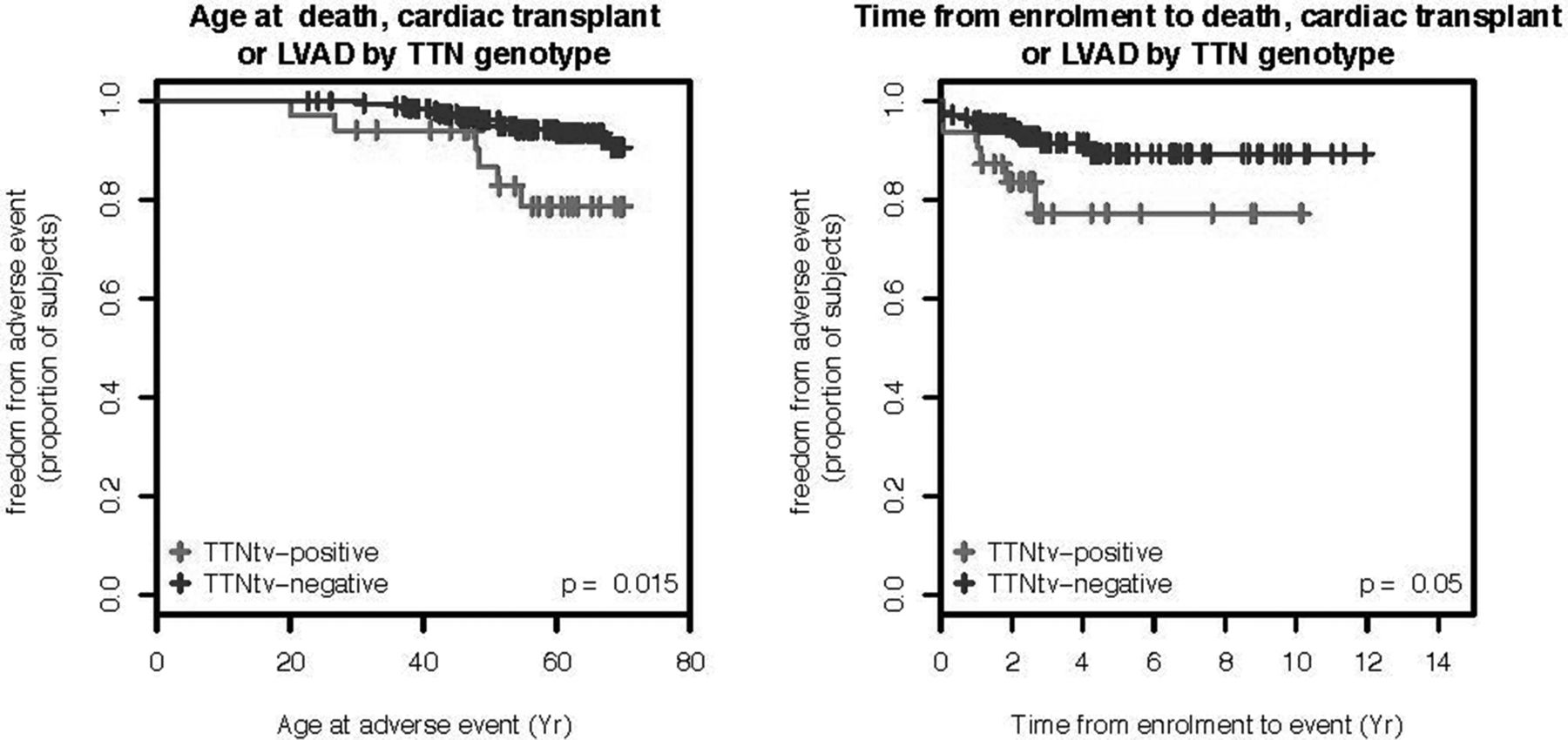
Results TTNtv were identified in 1.4% of controls (healthy volunteers, FHS and JHS participants), in 13% of unselected and 22% of end-stage DCM cases (OR 16.6, P = 4.8 × 10–45, DCM vs controls). More than 45% of controls have at least one rare TTN non-synonymous SNP (nsSNP). Rare and novel TTN nsSNPs were not enriched in DCM, either alone or in combination with a TTNtv (P = 0.8 (38.85% in DCM vs 38.24% in controls) suggesting that TTN nsSNPs are not an important cause of DCM. To improve TTN transcript annotations, we determined average cardiac TTN exon usage de novo from RNA-sequencing. TTNtv in DCM cases were enriched in highly utilised exons and isoforms (P = 2.5 × 10–4) compared to controls. We estimate that TTNtv in highly utilised exons have >93% probability of pathogenicity (likelihood ratio 14) in DCM cases. TTNtv-positive DCM patients had more depressed LV ejection fraction (LVEF: P = 0.02), thinner LV walls (P < 0.02), and a higher incidence of sustained ventricular tachycardia (P = 0.001). C-terminus TTNtv were associated with lower LVEF vs N-terminus (β=–18 ± 7%, p = 0.006) and were more common in end-stage disease. No change was detected in total TTN mRNA or protein levels in TTNtv-positive hearts.
Conclusion TTNtv are the most common cause of DCM. TTN nsSNPs are not an important cause of DCM in the absence of other discriminating features. Incorporation of variant position and exon-specific expression improves interpretation of TTNtv. Most individuals with TTNtv do not develop DCM, but TTNtv in highly utilised, particularly distal exons commonly cause DCM with severely impaired LV function and life-threatening ventricular arrhythmias, likely through dominant-negative mechanisms. In DCM patients, presence and position of TTNtv may aid prognostication and management.
{kind=link}
- Titin
- Genetic
- Dilated Cardiomyopathy