Article Text

Statistics from Altmetric.com
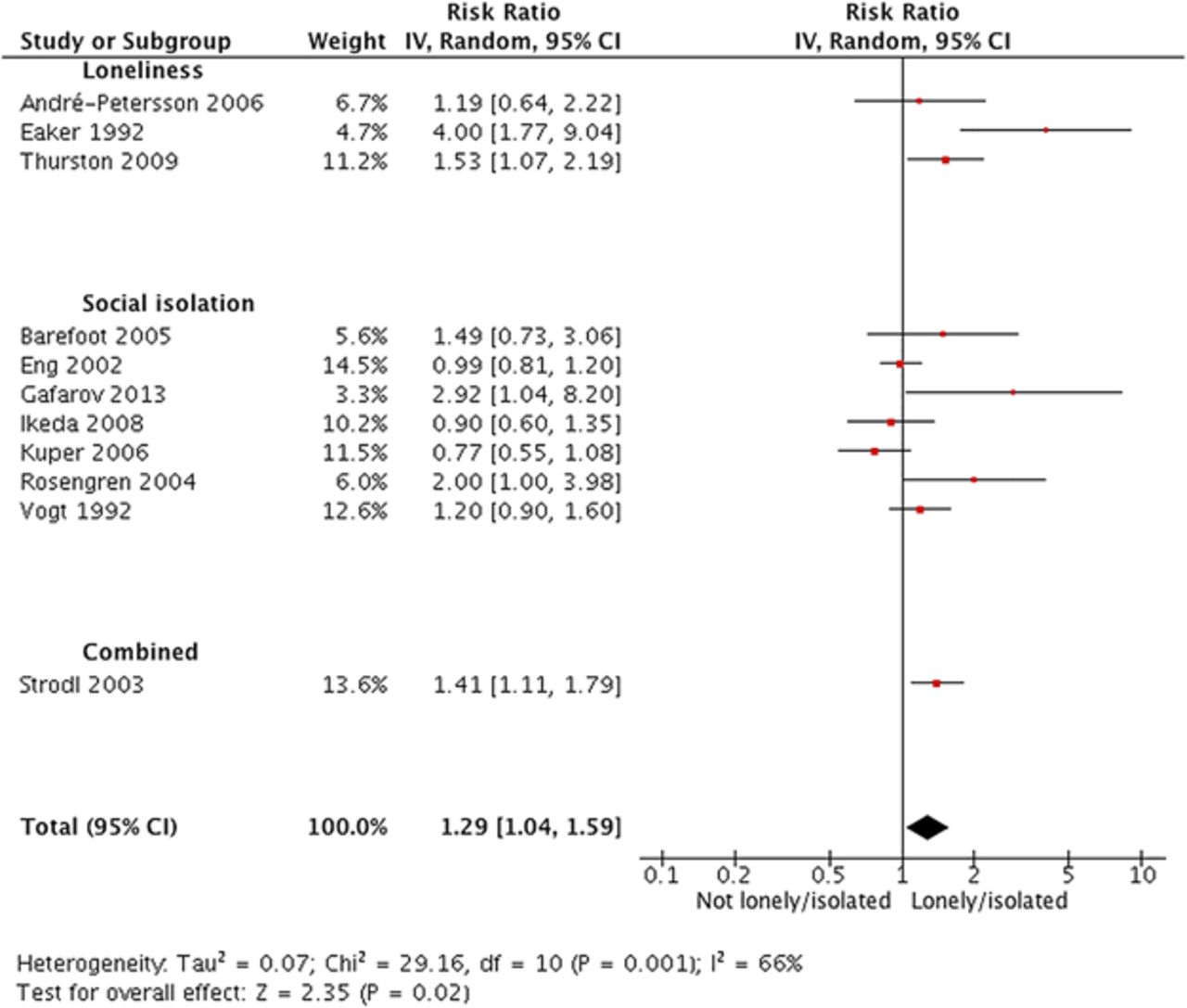
Loneliness and social isolation are associated with an increased risk of premature mortality. This association is related to several factors including behaviors (such as smoking or physical inactivity), reduced psychological well-being, and adverse physiological changes (such as altered immune function and hypertension). In order to better define the magnitude of risk for incident cardiovascular disease attributable to loneliness and social isolation, Valtorta and colleagues (see page 1009) performed a meta-analysis of 16 longitudinal databases with a total of 4628 coronary heart disease (CHD) events and 3002 strokes over 3 to 21 years of follow-up. This analysis showed that loneliness and social isolation were associated with a 29% increased risk of CHD (figure 1) and 32% increased risk of stroke, with no differences by gender. While acknowledging that causality cannot be inferred from an association study, the authors suggest that “tackling loneliness and isolation may be a valuable addition to CHD and stroke prevention strategies. Health practitioners have an important role to play in acknowledging the importance of social relations to their patients”.

Forest plot of studies investigating incident CHD. CHD, coronary heart disease.
In a linked editorial, Holt-Lunstad and Smith (see page 987) provide insight into the likely biological mechanisms underlying this association (figure 2). Further, they emphasize that this association in not simply due to established cardiovascular risk factors: “Taken together, these latest findings specific to loneliness and isolation bolster the already robust evidence documenting that social connections significantly predict morbidity and mortality, supporting the case for inclusion as a risk factor for cardiovascular disease”. Potential approaches to targeting social isolation and loneliness are discussed with the conclusion that: “similar to how cardiologists and other healthcare professionals have taken strong public stances regarding other factors exacerbating cardiovascular disease (e.g., smoking, diets high in saturated fats), further attention to social connections is needed in research and public health surveillance, prevention and intervention efforts”.

Simplified model of possible direct and indirect pathways by which social connections influence disease morbidity and mortality.
The ongoing controversy on the relationship between eating chocolate and heart disease was addressed in a study by Larsson and colleagues (see page 1017) that included over 67 thousand Swedish men and women who completed a baseline food questionnaire and then were followed prospectively for an average of 12 years. Myocardial infarction (MI) occurred in 4417 patients (6.5%) with a relative risk of 0.87 (95% CI 0.77 to 0.98; p for trend =0.04) for eating any type of chocolate at least 3 times per week compared to never eating chocolate. Although people who ate chocolate were less likely to be smokers, overweight, diabetic, hypertension or hypercholesterolemic and more likely to have a university education, the relationship between chocolate consumption and MI remained significant after adjustment for these variables. Based on the data from the current study and a meta-analysis including other prospective studies (figure 3), the authors conclude that: “although chocolate consumption may lower the ischemic heart disease risk, chocolate should be consumed in moderation because it is high in sugar, calories and saturated fat”.

Forest plot for the meta-analysis of chocolate consumption (highest vs lowest category) and risk of myocardial infarction or ischaemic heart disease. Squares indicate study-specific RR (size of the square reflects the study-specific statistical weight); the horizontal lines indicate 95% CIs; diamond indicates the overall RR with its 95% CI. *These studies have multiple categories for chocolate consumption; the other studies have only two categories (see table 3). COSM, Cohort of Swedish Men; EPIC, European Prospective Investigation into Cancer; IWHS, Iowa Women's Health Study; NA, not available; RR, relative risk; SHEEP, Stockholm Heart Epidemiology Program; SMC, Swedish Mammography Cohort.
Commenting on chocolate and cardiovascular outcomes, Donaldson and colleagues (see page 990) echo the view of chocolate lovers everywhere that it has been “both a surprise and a delight to many that recent research has suggested that chocolate in both its milky and dark disguises may have a protective effect against coronary artery disease.” Plausible biological mechanism for beneficial effects of chocolate are related to its high flavanol content which improves endothelial cell and platelet function, reduces insulin resistance, and improves serum lipid profiles, among other effects. Longer lasting effects of chocolate consumption “may be mediated by metabolites derived from chocolate by the gut microbiota which may persist longer in the circulation than the parent compounds”. They conclude: “Future studies will need to narrow down exactly how chocolate exerts its beneficial effects, the optimum type and quantity to consume and indeed, whether there are any subgroups of individuals, for whom there may be no benefit at all. Ultimately, we must not forget that along with its flavanols, chocolate is rich in both fat and sugar. Thus, whether the advice on potential benefit of chocolate consumption will be a moment on the lips of scientists but a lifetime on the hips of the population remains to be seen”.
There has been sparse data on use of direct oral anticoagulants (DOAC) to prevent stroke in adults with atrial fibrillation (AF) and valvular heart disease, leading most clinicians to continue using Vitamin K antagonist (VKA) therapy in these patients. In the Rivaroxaban Oral direct Factor Xa Inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF) study, although patients with prosthetic valves or mitral stenosis were excluded, about 14% of enrolled subjects had native valve disease, including 214 with aortic stenosis (AS) and 1726 with mitral (MR) or aortic regurgitation (AR) (see page 1036). Expressed as rates per 100 patient-years, the risk of stroke, systemic embolism or vascular death was twofold higher for AS (10.84) compared to MR/AR (4.90) or no significant valve disease (4.31) and there was a higher risk of bleeding in patients with valve disease (figure 4). However, the relative efficacy of rivaroxaban compared to VKA therapy was no different in patients with valve disease compared to those without significant heart disease.

Efficacy endpoints by SVD subtype and for patients with no SVD based on ITT patients. Efficacy endpoints (events per 100 patient-years, unadjusted) by SVD subtype and for patients with no SVD based on ITT patients. p Values for any difference among groups are based on Cox proportional hazards models. Patients in both treatment arms are combined. ITT, intention to treat; MI, myocardial infarction; pt-years, patient-years; SE, systemic embolism; SVD, significant valve disease; MR or AR, mitral or aortic regurgitation; vasc. death, vascular death.
These data underscore the high mortality and event rates associated with AS, even when only mild to moderate in severity, with a high stroke rate in AS patients with AF. As the authors note: “For efficacy outcomes, …. the risk relationship between rivaroxaban and warfarin was consistent across significant valve disease (SVD) subgroups. Hazard ratios from the full ROCKET AF cohort are the best estimate of treatment effects”. The clinical implication of these findings is that DOAC therapy might be considered in adults with AF and native valve disease when anticoagulation is indicated, taking the increased risk of bleeding with any therapy into account along with other patient specific factors. In addition, risk for embolism and bleeding may differ depending on the specific type of valve disease.
The Education in Heart article in this issue addresses carotid artery stenting (see page 1059) and provides details of the appropriate diagnostic evaluation of patients with carotid artery disease, discusses the the strengths and limitations of randomized trials comparing carotid artery stenting and endarterectomy, and presents a practical clinical algorithm for patient management (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
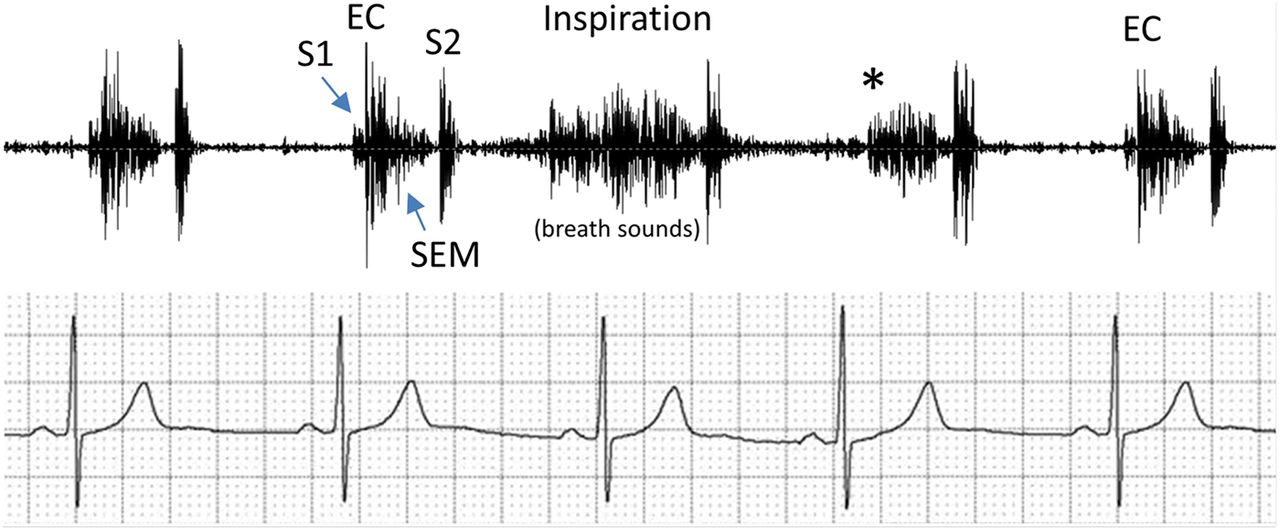
Phonocardiogram of the patient's heart sounds during respiration with simultaneous electrocardiogram
The Image Challenge (see page 1008) in this issue shows a phonocardiogram (the sound clip is online) to test your auscultation skills (figure 5).
Linked Articles
- Education in Heart
- Editorial
- Coronary artery disease
- Cardiac risk factors and prevention
- Editorial
- Valvular heart disease
- Image challenge