Article Text

Abstract
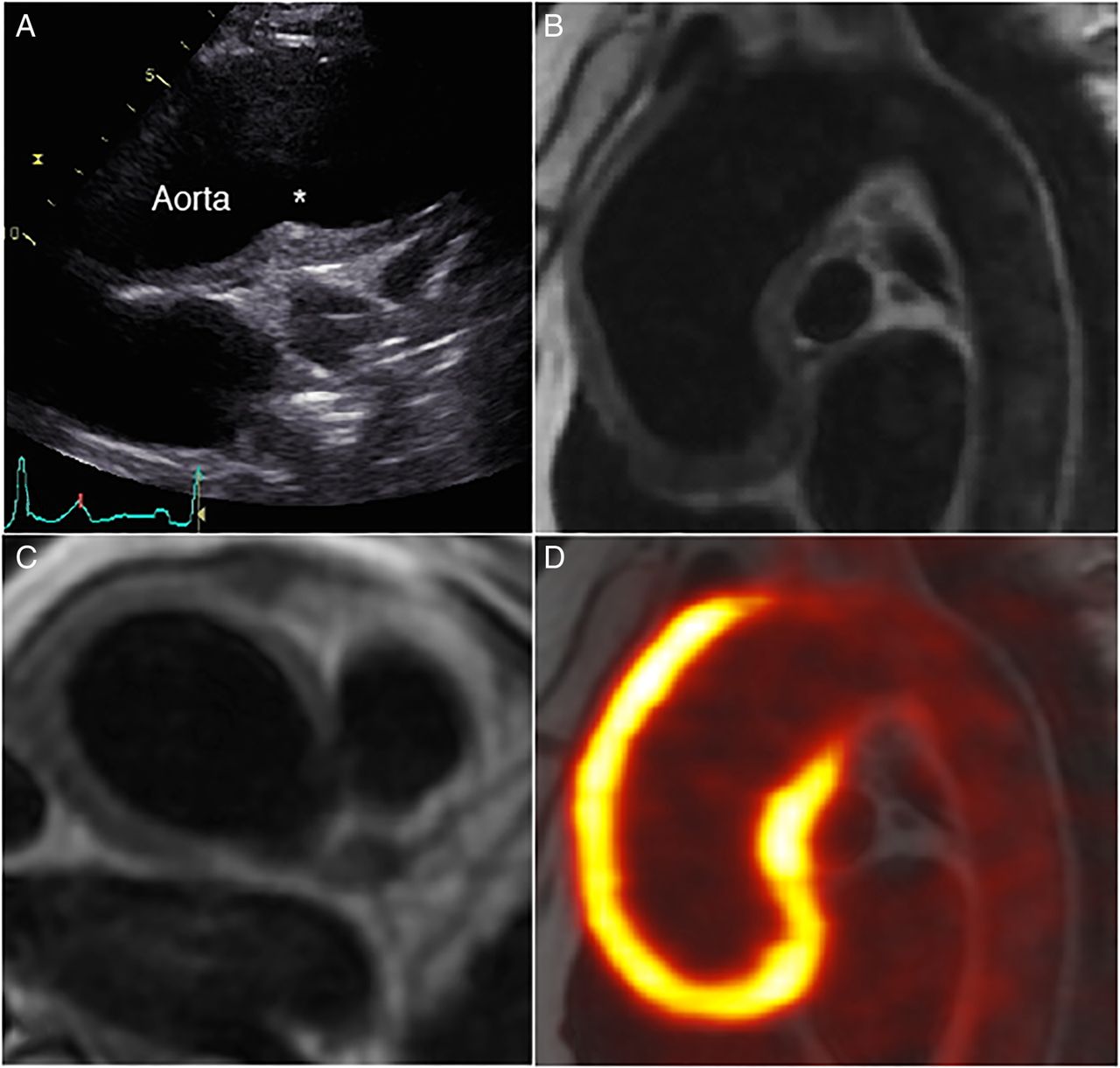
Clinical introduction A 57-year-old woman presented to our clinic with breathlessness brought on while walking uphill. She had been recently diagnosed with systemic hypertension. There was no known family history of cardiac disease, or prior smoking habit. On examination, pulse was 73 bpm and blood pressure 155/73 mm Hg, which was asymmetrical in her arms. Auscultation revealed a readily audible early diastolic murmur in the aortic area and bilateral subclavian bruits. ECG showed sinus rhythm with no abnormality. Transthoracic echocardiography demonstrated mild-to-moderate aortic regurgitation, and normal left ventricular size and function. The ascending aorta was mildly dilated (41 mm), with para-aortic thickening noted. Owing to the abnormal appearance of the aortic wall, cardiac MRI, and subsequently 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) scan was performed (figure 1).
Question Which complication of the underlying disease is evident in figure 1, panel C?
Aortic aneurysm
Aortic dissection
Aortic thrombus
Coronary artery aneurysm
Coronary sinus fistula
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com

Transthoracic echocardiogram in high left parasternal long-axis view (A); cardiac MRI with black-blood sequence in sagittal (B) and axial planes (C); fused 18F-fluorodeoxyglucose positron emission tomography-MRI (D). The asterisk in 1A refers to para-aortic thickening.
Answer: D
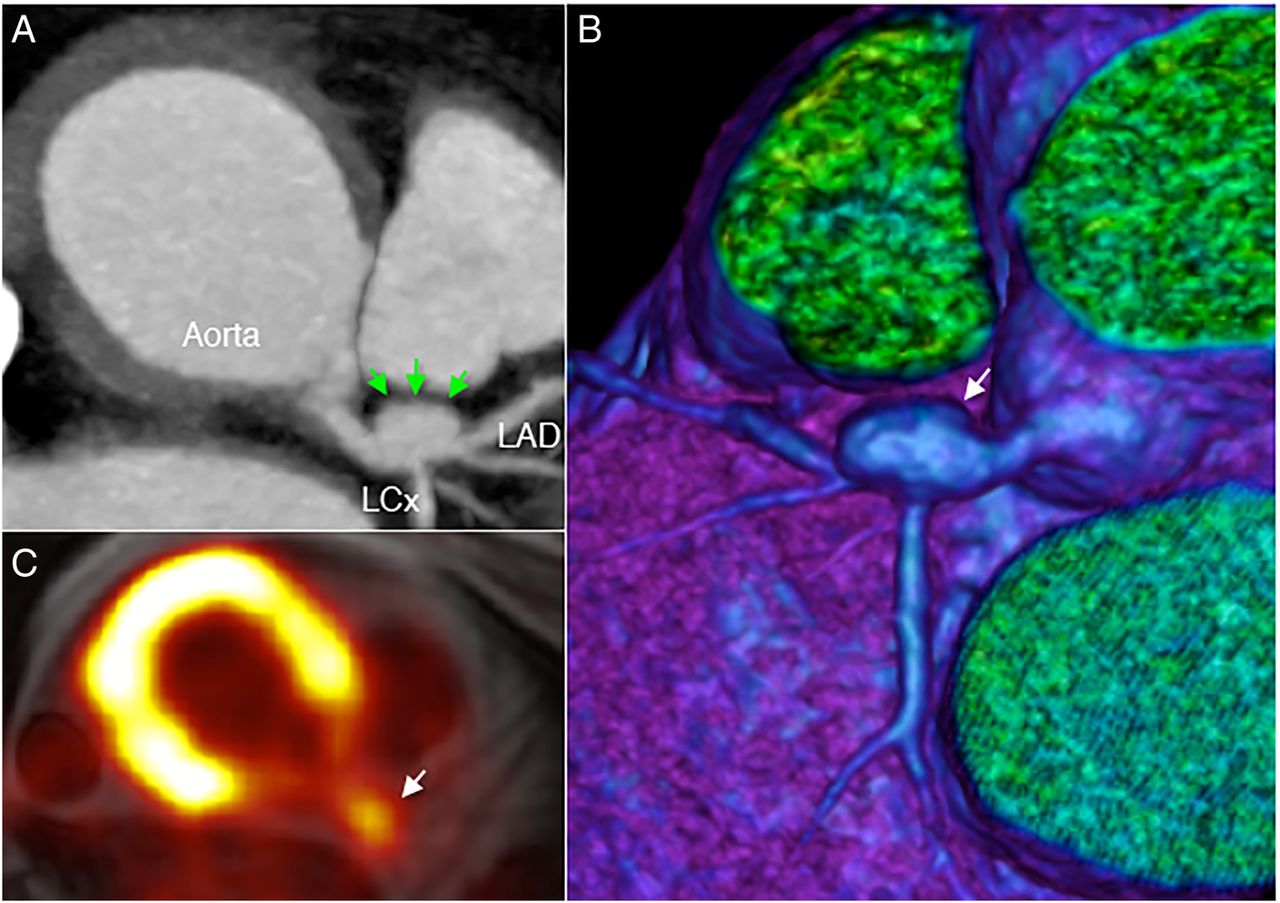
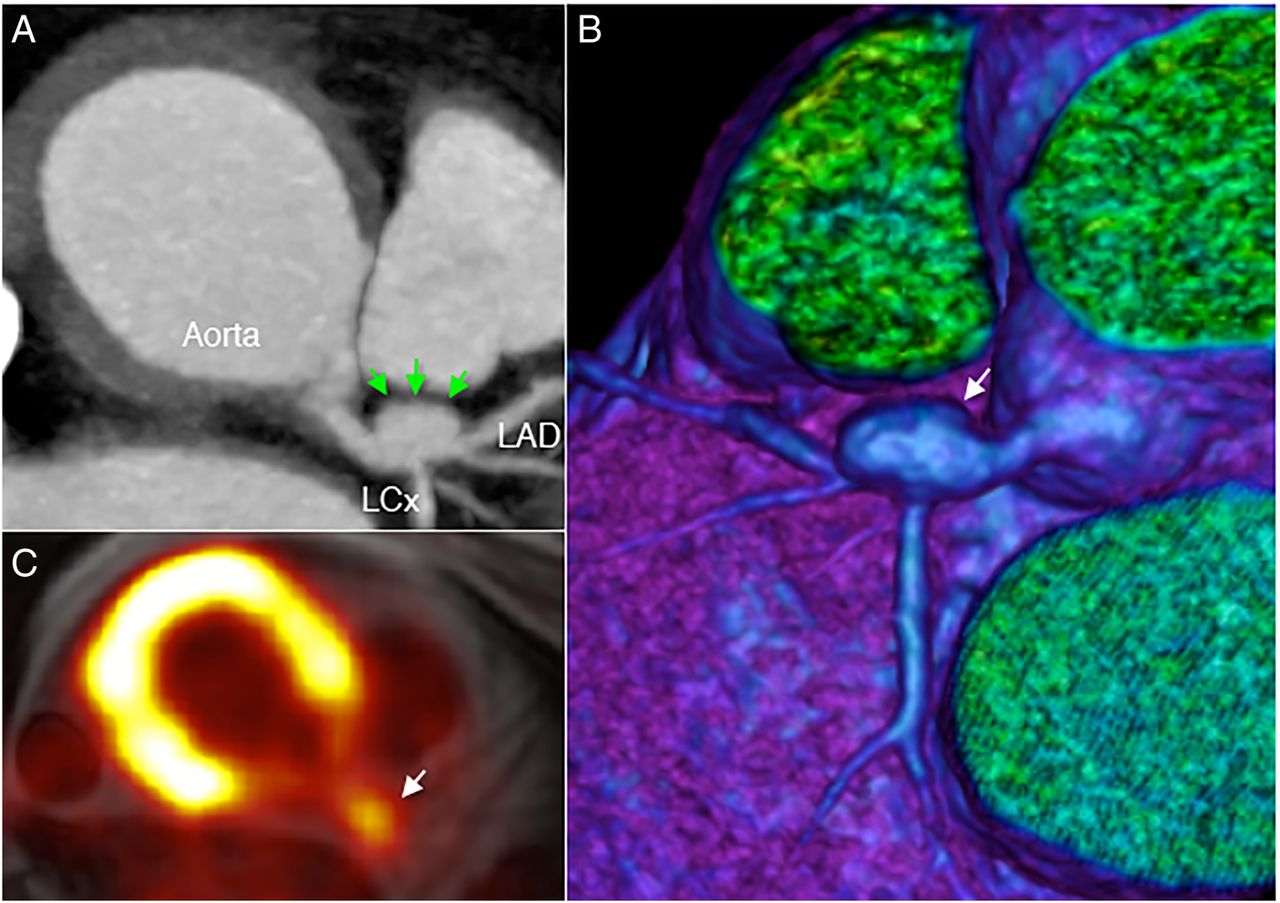
Cardiac MRI shows marked circumferential proximal para-aortic soft tissue thickening, measuring 8.5 mm. Strikingly, a large (8 mm) coronary artery aneurysm involving the left main stem and proximal left anterior descending artery is also evident on MRI. The coronary artery aneurysm (arrows) was further characterised using CT angiography, shown in axial view and three-dimensional volume-rendered CT (figure 2). There was also a non-calcified atherosclerotic plaque at the transition of the aneurysmal and tubular left anterior descending artery, and bilateral subclavian stenoses. 18F-FDG PET images demonstrated severe inflammation of the proximal aorta (maximum standardised uptake value 6.7) and the coronary aneurysm. The underlying unifying diagnosis was vasculitis, most likely Takayasu's arteritis in type. While other vasculitides can cause aortitis, coronary involvement and presence of subclavian stenoses support the diagnosis of Takayasu's arteritis. This large-vessel granulomatous vasculitis typically affects the aorta and its main branches, causing stenosis at the vessel origin.1 Up to 40% of patients with Takayasu's arteritis also exhibit cardiac complications, which include aortic regurgitation, accelerated atherosclerosis, and, rarely, coronary artery aneurysm.2 Multi-modal cardiac imaging plays an important role in diagnosis and therapeutic monitoring.3 ,4
{kind=link}
{kind=link}
Coronary artery aneurysm (arrows) shown using CT angiography (A), three-dimensional CT reconstruction (B) and 18F-fluorodeoxyglucose positron emission tomography-MRI (C). LAD, left anterior descending artery; LCx, left circumflex artery.
Acknowledgments
J.M.T. is supported by a Wellcome Trust research training fellowship (104492/Z/14/Z). J.H.F.R. is part-supported by the HEFCE, the NIHR Cambridge Biomedical Research Centre, the British Heart Foundation, and the Wellcome Trust.
Footnotes
Twitter Follow James Rudd at @jhfrudd
Contributors JMT drafted the article. DG performed imaging. JMT, JHFR, RAR, DRJ and DG revised the article and contributed to its intellectual content.
Funding Wellcome Trust (104492/Z/14/Z).
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.