Article Text

Abstract
Despite prompt reperfusion by primary percutaneous coronary intervention (PPCI), the mortality and morbidity of patients presenting with an acute ST-segment elevation myocardial infarction (STEMI) remain significant with 9% death and 10% heart failure at 1 year. In these patients, one important neglected therapeutic target is ‘myocardial reperfusion injury’, a term given to the cardiomyocyte death and microvascular dysfunction which occurs on reperfusing ischaemic myocardium. A number of cardioprotective therapies (both mechanical and pharmacological), which are known to target myocardial reperfusion injury, have been shown to reduce myocardial infarct (MI) size in small proof-of-concept clinical studies—however, being able to demonstrate improved clinical outcomes has been elusive. In this article, we review the challenges facing clinical cardioprotection research, and highlight future therapies for reducing MI size and preventing heart failure in patients presenting with STEMI at risk of myocardial reperfusion injury.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
For patients presenting with an acute ST-segment elevation myocardial infarction (STEMI), the most effective therapy for reducing myocardial infarct (MI) size, preserving LV systolic function and preventing the onset of heart failure, is timely reperfusion by primary percutaneous coronary intervention (PPCI). Although, myocardial reperfusion is a pre-requisite to salvaging viable myocardium, the process of restoring coronary blood flow can paradoxically induce myocardial injury and cardiomyocyte death, thereby mitigating the full benefits of reperfusion in terms of MI size reduction—a phenomenon which has been termed ‘myocardial reperfusion injury’.1 ,2 The fact that a therapeutic intervention administered solely at the time of myocardial reperfusion can reduce MI size by up to half suggests that myocardial reperfusion injury may account for up to 50% of the final MI size.1 Although, the process of myocardial reperfusion has been optimised by advances in stent technology, new antiplatelet drugs (eg, prasugrel, ticagrelor and abciximab) and novel antithrombotic agents (eg, bivalirudin therapy), the latter being provided to maintain the rheology of blood flow, there is still no effective therapy for preventing myocardial reperfusion injury in PPCI patients. Following a STEMI, the size of the resultant myocardial infarct has been strongly linked with the development of adverse LV remodelling and heart failure,3 and subsequent prognosis following PPCI.4 Larose et al5 have shown that an MI size of ≥23% LV volume was associated with a HR of 6 for major adverse cardiac events.
In this article, we review the challenges facing clinical cardioprotection research, and highlight future opportunities for reducing MI size and improving clinical outcomes in patients presenting with STEMI at risk of myocardial reperfusion injury.
Challenges facing clinical cardioprotection research
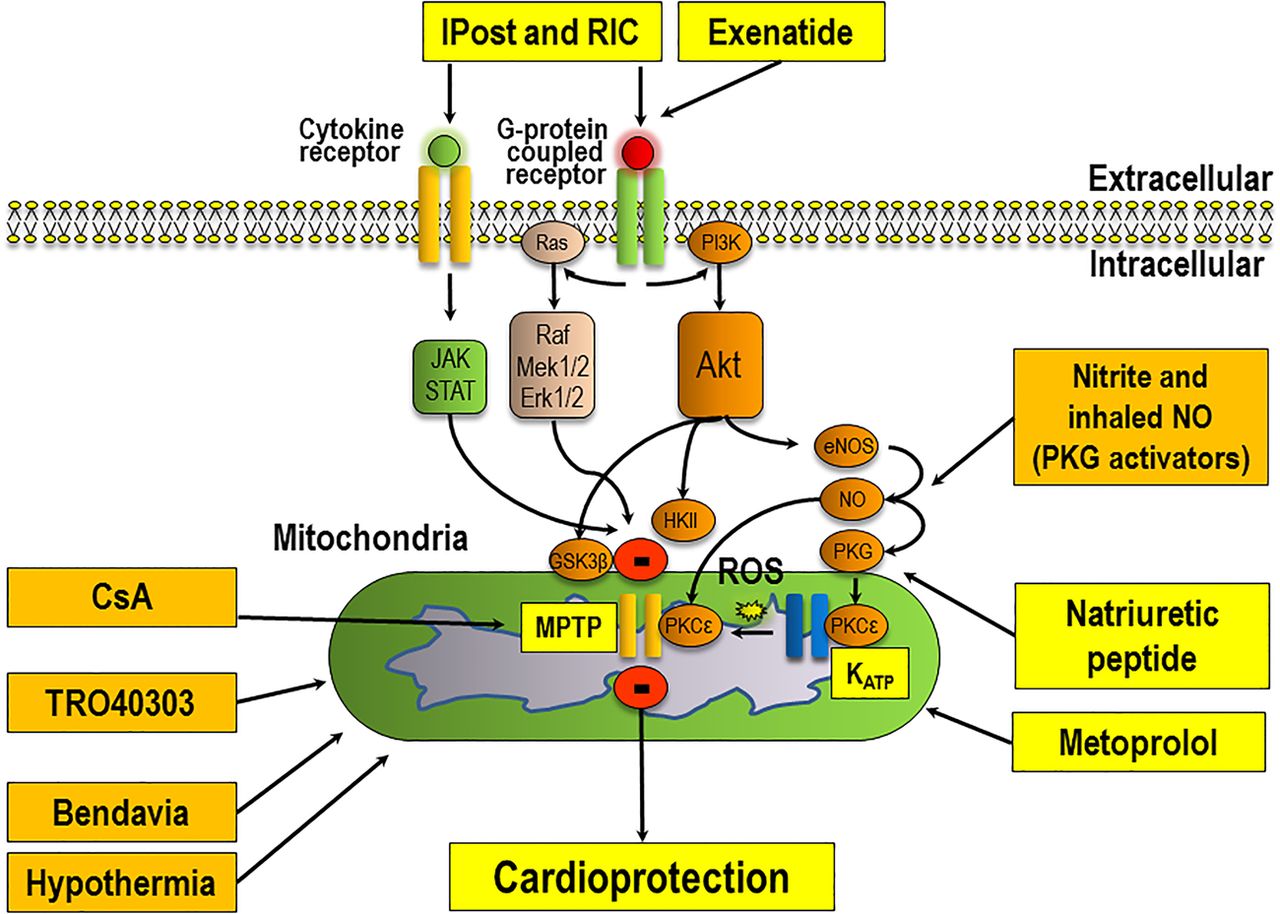
There are a number of challenges facing clinical cardioprotection research. First, the translation of novel cardioprotective therapies into the clinical setting for patient benefit has been extremely difficult. Extensive literature exists on the complex array of prosurvival signalling pathways which underlie cardioprotection, and the readers are referred to a number of recent reviews6 ,7—in figure 1, a simplified overview is provided which illustrates some of the major prosurvival pathways which mediate cardioprotection at the time of reperfusion. These have provided researchers with a number of molecular targets for pharmacological targeting of myocardial reperfusion injury. Over the past 30–40 years, a vast number of therapies with proven efficacy for preventing myocardial reperfusion injury and reducing MI size in experimental animal studies (eg, antioxidants, magnesium, calcium-channel blockers, anti-inflammatory agents, erythropoietin, atorvastatin, glucose-insulin-potassium therapy, adenosine) have produced disappointing results when investigated in the clinical setting as adjunctive therapy to reperfusion (reviewed in Ref. 9). More recently, a number of attempts to reduce MI size in patients presenting with STEMI have also failed to meet their primary end point of cardioprotection—these have included studies investigating therapeutic hypothermia, targeting mitochondrial function, and modulation of nitric oxide signalling as adjuncts to myocardial reperfusion (table 1 and figure 1).
Recent attempts to reduce MI size in reperfused patients presenting with STEMI
{kind=link}
This scheme depicts the main prosurvival signalling pathways underlying ischaemic conditioning and the potential sites of actions for novel therapies which have recently been investigated in clinical studies to reduce myocardial infarct (MI) size in reperfused ST-segment elevation MI (STEMI) patients (please see tables 1⇓–3, for details on the novel therapies and their potential sites of actions). The orange boxes indicate those therapies which have had mainly neutral effects on MI size and/or clinical outcomes (table 1) and the yellow boxes indicate those therapies which have the potential to improve clinical outcomes in reperfused patients presenting with STEMI (table 2). The signalling cascade underlying cardioprotection begins at the cardiomyocyte plasma membrane with the activation of G-protein coupled or cytokine receptors by autocoids such as adenosine, bradykinin or opioids (released in response to the ischaemic conditioning stimulus)—this results in the recruitment of signalling pathways such as the Reperfusion Injury Salvage Kinase (phosphatidylinositol 3-kinase-Akt (PI3K-Akt) and Mitogen-activated protein kinase kinase 1/2 -Extracellular signal-Regulated Kinase 1/2 (MEK1/2-Erk1/2)), Survivor Activator Factor Enhancement (SAFE), Janus kinase and Signal Transducer and Activator of Transcription (JAK-STAT) and the PKG pathways. These salvage pathways have been shown to activate downstream mediators such as endothelial Nitric Oxide Synthase (eNOS), Glycogen Synthase Kinase 3 Beta (GSK-3β), Hexokinase II (HKII), Protein Kinase C-epsilon (PKC-ε), the mitochondrial ATP-dependent potassium channel (KATP) which then mediate an inhibitory effect on mitochondrial permeability transition pore (MPTP) opening (adapted from Ref. 8).
The reasons for this failure to translate cardioprotection into the clinical setting have been attributed to a number of factors including the use of inappropriate animal MI models and poorly designed clinical studies—a topic which has been discussed extensively in the literature and is highlighted in a following section.9 ,17
A second challenge facing clinical cardioprotection research is that clinical outcomes of patients presenting with STEMI following PPCI continue to improve, making it increasingly difficult to demonstrate a reduction in MI size and improvement in clinical outcomes with a novel cardioprotective therapy. However, although mortality following STEMI is in decline, the number of patients surviving STEMI and going on to develop heart failure is increasing. There remains, therefore, an unmet need to discover novel therapeutic strategies capable of preventing myocardial reperfusion injury and reducing MI size, so as to preserve LV systolic function and prevent the onset of heart failure in patients presenting with reperfused STEMI. In the next section and in tables 2 and 3 we highlight a number of therapeutic strategies, which hold promise for reducing MI size and improving clinical outcomes in patients presenting with reperfused STEMI.
Potential pharmacological strategies for reducing MI size and improving clinical outcomes in patients presenting with reperfused STEMI
Potential mechanical strategies for reducing MI size and improving clinical outcomes in patients presenting with reperfused STEMI
Potential therapies for reducing MI size
Ischaemic postconditioning: interrupting myocardial reperfusion to limit MI size
Interrupting myocardial reperfusion with several short-lived episodes of myocardial ischaemia has been demonstrated in experimental animal studies to prevent myocardial reperfusion injury and reduce MI size—a phenomenon which has been termed ‘ischaemic postconditioning’ (IPost).40 This therapeutic approach was rapidly translated into the clinical setting by Staat et al,27 who demonstrated that IPost (using four 1-min low-pressure inflations and deflations of the angioplasty balloon following direct stenting of the culprit lesion) led to a 36% reduction in MI size in PPCI-treated patients presenting with STEMI. Although a number of subsequent studies have reported similar beneficial findings with IPost, there have been a substantial number of neutral studies29 ,30 (table 3). The reasons for this are unclear but it appears that most benefit is obtained in patients with anterior STEMI presenting with a completely occluded artery (TIMI 0).29 ,28 Furthermore, the IPost protocol is best delivered following direct stenting and upstream of the stent rather than within it. Whether IPost can improve long-term clinical outcomes is not known, and is currently being investigated in the ongoing Danish Study of Optimal Acute Treatment of Patients with ST-Elevation Myocardial Infarction (DANAMI-3) trial.31
Natriuretic peptide
Experimental animal studies have found that administering atrial natriuretic peptide (ANP) prior to myocardial reperfusion can reduce MI size through the activation of known prosurvival signalling pathways.41 Kitakaze et al18 translated this therapeutic approach in a large clinical study comprising 569 patients presenting with STEMI, in which administering Carperitide (an ANP analogue) at the time of PPCI was associated with a 14.7% reduction in enzymatic MI size (table 2). Further studies are required to confirm these findings and investigate whether this therapeutic approach can improve clinical outcomes in patients presenting with reperfused STEMI.
Ciclosporin-A: targeting the mitochondrial permeability transition pore
The opening of the mitochondrial permeability transition pore (MPTP) in the first minutes of reperfusion is a critical mediator of reperfusion-induced cardiomyocyte death, and preventing its opening using pharmacological inhibitors of the MPTP such as ciclosporin-A (CsA) has been reported in experimental studies to limit MI size.42 The first study to translate this therapeutic approach into the clinical setting was by Piot et al19 who found in a small study of 58 patients presenting with STEMI that administering a single intravenous (IV) bolus of CsA prior to PPCI reduced MI size by approximately 40% as measured by creatine kinase (CK) (table 2). The recently completed CYCLosporinE A in Reperfused Acute Myocardial Infarction (CYCLE) study investigated the effect of MPTP inhibition using CsA (Sandimmune preparation) on ST-segment resolution, and the results of this study are eagerly awaited (table 2). Rather surprisingly, the large randomised Cyclosporine and Prognosis in Acute Myocardial Infarction Patients (CIRCUS) Phase III trial (comprising 791 patients presenting with acute anterior STEMI with data on the primary end point), which investigated the effect of CsA as an adjunct to PPCI on long-term clinical outcomes, failed to show any beneficial effect on the primary combined end point of all-cause mortality, hospitalisation for heart failure and adverse LV remodelling at 1 year21 (table 2). The reason for this neutral result is not clear—whether it relates to the Ciclomulsion preparation used in the study or failure of the drug to reach its target is not clear.2 Should MPTP inhibition ever be implemented as a therapeutic approach into the clinical setting, novel, more specific MPTP inhibitors will be needed, given the potential side effects and off-target effects of CsA.
Exenatide: lizard saliva and cardioprotection
Exenatide (Byetta), a synthetic version of exendin-4 (a peptide isolated from the saliva of the Gila lizard), is a long-acting analogue of glucagon-like peptide-1 (GLP-1), a hormone which lowers blood glucose by stimulating insulin secretion.43 Interestingly, GLP-1 and its analogues such as exenatide have been reported in experimental animal studies to reduce MI size through the activation of prosurvival intracellular signalling pathways when administered prior to reperfusion.44 ,45
Lonborg et al23 showed that initiating a 6 h infusion of exenatide prior to PPCI reduced MI size by 30% as measured by cardiovascular magnetic resonance (CMR) in patients presenting with STEMI, and most benefit was seen in those patients presenting <132 min from first medical contact.22 Woo et al24 also showed a significant reduction in MI size by CMR (26.4±11.6 g in the placebo arm vs 12.8±11.7 g in the exenatide arm: p<0.01) in 58 patients with subcutaneous exenatide (table 2). Whether this effect of exenatide portends to improved clinical outcomes in patients presenting with reperfused STEMI is not known and remains to be determined in a large randomised clinical trial.
Remote ischaemic conditioning: transient limb ischaemia/reperfusion
Inducing brief non-lethal episodes of ischaemia and reperfusion in the arm or leg, using serial inflations and deflations (three to four 5 min cycles) of a standard blood pressure cuff placed on the upper arm or thigh, has been shown to protect the heart against acute ischaemia-reperfusion injury (IRI)—a phenomenon known as ‘remote ischaemic conditioning’ (RIC).46–48 It has been suggested that a blood-borne factor, of as yet unknown identity, is generated in response to the limb RIC stimulus, and this then transfers the cardioprotective stimulus from the limb to the heart where prosurvival intracellular signalling pathways are then activated and confer cardioprotection.48
A number of proof-of-concept clinical studies have demonstrated MI size reduction using limb RIC in patients presenting with STEMI treated by either PPCI32–34 ,37 ,39 ,49 ,50 and by thrombolysis38 (table 3). Whether this simple, non-invasive, low-cost, non-pharmacological intervention can improve long-term clinical outcomes in this patient group is currently being investigated in the Effect of RIC on Clinical Outcomes in STEMI Patients Undergoing PPCI and the Effect of Remote Ischaemic Conditioning on Clinical Outcomes in STEMI Patients Undergoing PPCI (CONDI2/ERIC-PPCI) trial. This European multicentre (Denmark, UK and Spain) randomised clinical trial of 4300 patients presenting with STEMI will determine whether upper limb RIC applied prior to PPCI can reduce the rate of cardiac death and heart failure hospitalisation at 1 year (ClinicalTrials.gov Identifiers: NCT02342522 and NCT01857414).
Repeated RIC post MI has attracted attention as a potential chronic cardioprotective therapy. Wei et al51 demonstrated in the rat heart that daily limb RIC for 28 days prevented adverse post-MI LV remodelling. The Chronic Remote Ischemic Conditioning to Modify Post-MI Remodeling (CRIC-RCT, NCT01817114) study and the Daily Remote Ischaemic Conditioning following Acute Myocardial Infarction (DREAM, NCT01664611) study are currently investigating this therapeutic strategy (daily RIC for 1 month) on post-MI LV remodelling following PPCI.
Metoprolol: β-blockers and MI size reduction
Whether early β-blocker therapy is beneficial in patients presenting with reperfused STEMI is controversial and had not previously been investigated in the PPCI era. Using a porcine mode of acute myocardial IRI, Ibanez et al52 demonstrated that IV metoprolol administered prior to reperfusion resulted in a fivefold increase in myocardial salvage. The same researchers went on to apply this therapeutic strategy in the clinical setting by demonstrating that IV metoprolol administered in the ambulance prior to PPCI reduced MI size by 20% (assessed by CMR)52 and improved clinical outcomes in patients presenting with STEMI (as a secondary end point)25 ,26 (table 2). Whether this pharmacological approach to reducing MI size can improve clinical outcomes will need to be tested in a large prospectively powered randomised controlled clinical trial.
Combination reperfusion therapy: a novel therapeutic strategy
Prior attempts to reduce MI size in patients presenting with STEMI have relied on targeting one single component of myocardial reperfusion injury with a single agent. Whether, using combination reperfusion therapy can provide more effective cardioprotection against myocardial reperfusion injury remains to be investigated. In this regard, Alburquerque-Bejar et al53 have recently demonstrated an additive 26% reduction in MI size when combining RIC with insulin-like therapies (such as glucose-insulin-potassium and exenatide) in a porcine acute MI model. The Combination Therapy in Myocardial Infarction (COMBAT-MI) study (ClinicalTrials.gov Identifier: NCT02404376) will investigate the potential benefits of combined reperfusion therapy using RIC with exenatide on MI size reduction in patients presenting with STEMI treated by PPCI. Although an initial clinical study of 54 patients in patients presenting with reperfused STEMI failed to show an additive cardioprotective effect with RIC and IPost administered in combination,37 a recently published larger study of 696 patients found increased myocardial salvage in those patients administered RIC in combination with IPost when compared with controls (49 (IQR 30–72) vs 40 (IQR 16–68), p=0.02)39 (table 3).
Optimising the clinical translation of cardioprotection
There are number of factors which need to be taken into consideration when designing clinical cardioprotection studies for reducing MI size in patients presenting with reperfused STEMI, as this may help facilitate the translation of novel cardioprotective therapies into the clinical setting for patient benefit.9
Patient selection—where possible, consider selecting those patients presenting with STEMI who are most likely to benefit from the novel cardioprotective therapy—those presenting: early (<2–3 h as shown by Lonborg et al22 and Garcia-Dorado et al54); with a large area-at-risk (>30% of the LV volume)29 and an occluded artery prior to PPCI (TIMI <1) may be more likely to benefit from adjunctive therapy for reducing MI size. However, restricting patient selection has to be balanced with confining the testing of the novel cardioprotective therapy to a smaller selected group of patients.
The cardioprotective therapy—consider only testing those novel therapies which have shown conclusive cardioprotection in a number of experimental small and large animal MI studies. In this regard, the NIH CESAR network in the USA offers the opportunity to test the cardioprotective efficacy of novel therapies in a multicentre small and large animal model setting akin to a multicentre clinical trial.55 Similarly, where possible it is important to demonstrate that the novel cardioprotective therapy is efficacious in several different clinical studies before proceeding to testing it in clinical outcomes studies.
Confounders of cardioprotection—the presence of certain comorbidities (such as age, diabetes, pre-existing coronary artery disease, heart failure, hypertension, dyslipidaemia) and concomitant medication (nitrates, morphine, nicorandil, sulfonylureas, platelet inhibitors) may interfere with the efficacy of the novel cardioprotective therapy.56 Where possible this should be taken into consideration when designing experimental or clinical cardioprotection studies.
Timing of the cardioprotective therapy—as myocardial reperfusion injury manifests in the first minutes of reperfusion, it is essential that the novel cardioprotective therapy is administered prior to myocardial reperfusion if it is to be effective. A number of neutral clinical studies were due to administering the cardioprotective therapy after reperfusion had already taken place.
Study end points—consider selecting study end points which are most likely to be affected by the novel cardioprotective therapy—these include surrogate end points such as MI size (enzymatic, myocardial single-photon emission CT or CMR), myocardial salvage index (which is more sensitive than MI size reduction but requires the assessment of the AAR); microvascular obstruction (coronary no-reflow, index of microcirculatory resistance, or CMR), LV size and function and hard clinical end point such as heart failure hospitalisation, and cardiac death.
Future perspectives
Clinical cardioprotection research remains a challenge—mortality rates following a PPCI-treated STEMI are in decline, which makes demonstrating a further reduction in MI size and improved clinical outcomes increasingly more difficult. However, an increasing number of patients are developing heart failure—as such, novel cardioprotective therapies which target myocardial reperfusion injury and reduce MI size provide the opportunity to preserve LV systolic function and prevent the onset of heart failure. The failure to translate a large number of infarct-limiting therapies into the clinical setting should not be taken as evidence that myocardial reperfusion injury does not exist in humans. Rather, it should provide the impetus to optimise the design of our experimental animal and clinical studies, and improve how we select which novel cardioprotective therapy to test in the clinical setting—this may hopefully facilitate the discovery of new effective therapies for reducing MI size and preventing heart failure in patients presenting with reperfused STEMI. Initial data suggest that using a combination of therapies to target myocardial reperfusion injury may be more beneficial than using a single therapy approach, and using this approach may result in improved clinical outcomes in this patient group.
References
Footnotes
Contributors All authors contributed to writing paper.
Funding DJH is supported by the Rosetrees Trust, the NIHR University College London Hospitals Biomedical Research Centre and a BHF Senior Clinical Research Fellowship (FS/10/039/28270). This work was undertaken at UCLH/UCL who received a proportion of funding from the Department of Health's NIHR Biomedical Research Centres funding scheme of which DMY is a senior investigator.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.