Article Text

Abstract
Introduction Heart failure with preserved ejection fraction (HFPEF) carries poor prognosis and definitive therapies are lacking. Transthoracic echocardiography (TTE) remains the primary diagnostic modality in HFPEF. We aimed to evaluate the diagnostic and prognostic utility of cardiovascular magnetic resonance (CMR) in HFPEF.
Methods Patients were recruited as part of Developing Imaging And plasMa biOmarkers iN Describing-HFPEF (DIAMOND-HFPEF): a prospective, single-centre study. Inclusion criteria were: clinical or radiographic evidence of heart failure (HF) and ejection fraction > 50% on TTE. Exclusion criteria were: myocardial infarction (MI) in the preceding 6 months, suspected or confirmed cardiomyopathy, constrictive pericarditis, non-cardiovascular life expectancy < 6 months and severe valve/ lung/ renal disease. The CMR protocol included cine, adenosine stress/rest perfusion and late gadolinium enhancement imaging on a 3-Tesla scanner. Both TTE and CMR were performed during the index study visit and reported independently. Follow-up outcome data was collected at a minimum of 6 months post-enrollment for the primary endpoint (death and/or re-hospitalisation with HF).
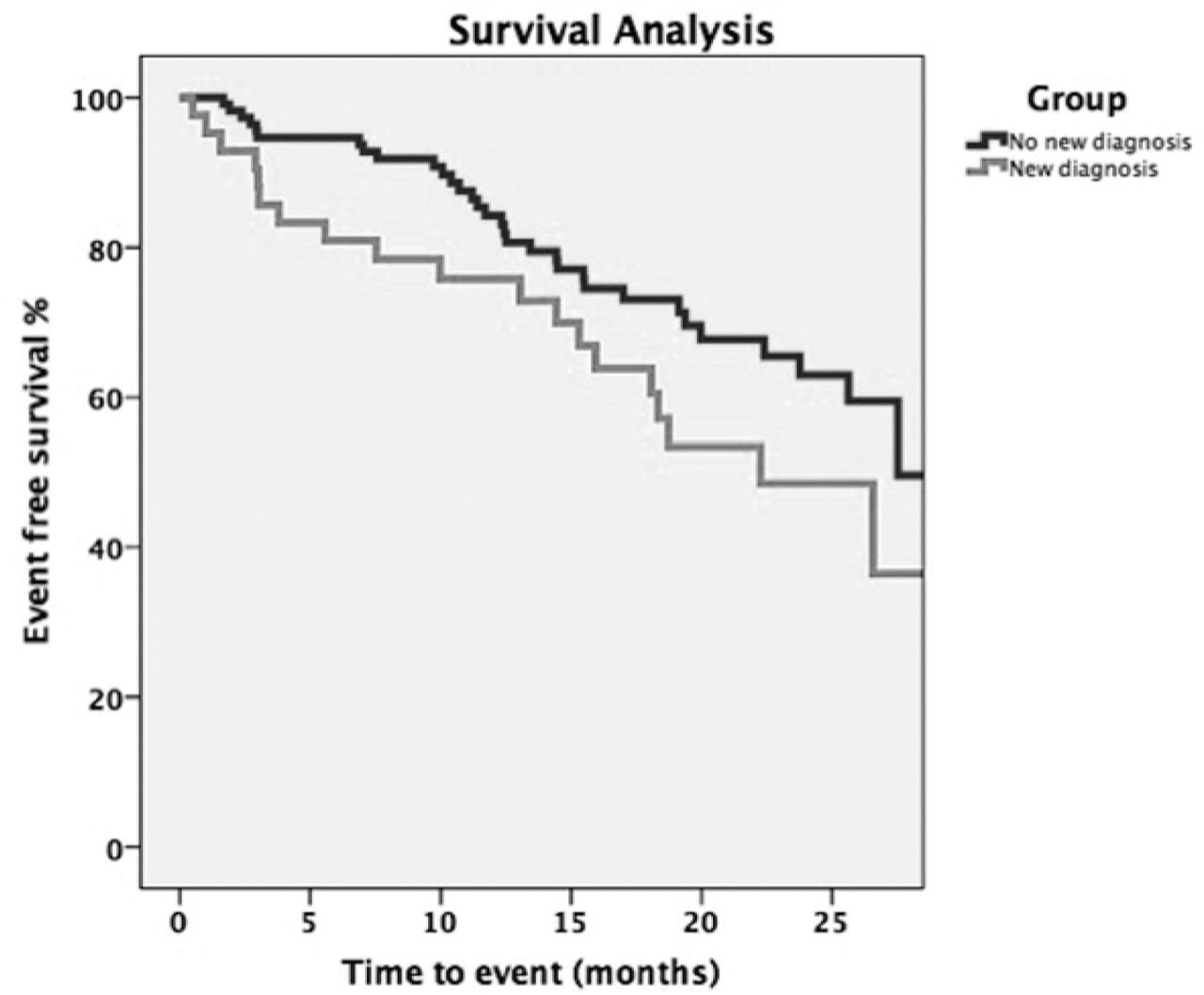
Results 154 patients (mean age 72.4 ± 10.0 years, 51% Male) underwent both CMR and TTE. CMR detected the following previously unknown diagnoses (total n = 42): significant coronary artery disease (n = 16, including 14 with 'silent'), microvascular dysfunction (n = 11), hypertrophic cardiomyopathy (n = 10) and constrictive pericarditis (n = 5). During follow-up (median = 623 days, interquartile range 455 -– 753), there were 53 primary outcome events. Kaplan-Meier survival analysis (see Figure 1) revealed worse outcomes in the 'new diagnoses group' (Log Rank test p = 0.046). In a multivariate Cox Regression model comprising significant independent predictors during univariate analysis (diastolic blood pressure, NHYA class, urea, eGFR and log BNP), the ‘new diagnoses group’ (hazard ratio [HR]: 1.917; 95% confidence interval [CI]: 1.064 to 3.454; p = 0.03) remained a significant independent predictor of primary outcomes (see Figure 2).


{kind=link}
{kind=link}
Conclusion In HFPEF, CMR identifies previously unknown pathologies in a significant minority (>25%). This group of ‘new diagnoses’ is associated with worse outcomes and is an independent predictor of death and/or re-hospitalisation with HF.
- HFPEF
- CMR
- prognosis