Article Text

Abstract
Objectives Cardiovascular disease (CVD) and chronic obstructive pulmonary disease (COPD) often coexist. We assessed the effect of inhaled COPD treatments on CVD outcomes and safety in patients with COPD and at heightened CVD risk.
Methods The SUMMIT (Study to Understand Mortality and MorbidITy) was a multicentre, randomised, double-blind, placebo-controlled, event-driven trial in 16 485 patients with moderate COPD who had or were at high risk of CVD. Here, we assessed the prespecified secondary endpoint of time to first on-treatment composite CVD event (CVD death, myocardial infarction, stroke, unstable angina or transient ischaemic attack (TIA)) by Cox regression and by clinician-reported CVD adverse events across the four groups: once-daily inhaled placebo (n=4111), long-acting beta2-agonist (vilanterol (VI) 25 µg; n=4118), corticosteroid (fluticasone furoate (FF) 100 µg; n=4135) and combination therapy (FF/VI; n=4121).
Results Participants were predominantly middle-aged (mean 65 (SD 8) years) men (75%) with overt CVD (66%). The composite CVD endpoint occurred in 688 patients (first event: sudden death (35%), acute coronary syndrome (37%) and stroke or TIA (23%), and was not reduced in any treatment group versus placebo: VI (HR 0.99, 95% CI 0.80 to 1.22), FF (HR 0.90, 95% CI 0.72 to 1.11) and their combination (HR 0.93, 95% CI 0.75 to 1.14). Outcomes were similar among all subgroups. Adverse events, including palpitations and arrhythmias, did not differ by treatment.
Conclusions In patients with COPD with moderate airflow limitation and heightened CVD risk, treatment with inhaled VI, FF or their combination has an excellent safety profile and does not impact CVD outcomes.
Trial registration number NCT01313676.
- pulmonary disease
- cardiovascular disease
- inhaler therapies
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Cardiovascular disease (CVD), comprising both coronary heart disease and strokes, in conjunction with chronic obstructive pulmonary disease (COPD), accounts for the top three leading causes of death worldwide.1 Not only are they prevalent in the population, there is a well-established overlap of these conditions where CVD and COPD frequently coexist within individuals.2–5 Patients with COPD are more likely to have CVD than the general public.2–5 Roughly one-third of all deaths in those with COPD are due to CVD causes and the prognosis following a myocardial infarction (MI) is substantively worse in those with concomitant COPD.6–8 While a growing number of studies have helped to explain these observations,9 10 the optimal management of patients diagnosed with both illnesses continues to be a matter of debate.11
One important issue contributing to present-day clinical equipoise is the unclear safety versus benefit of inhaled therapies for COPD in patients with coexisting CVD.11 Early studies and meta-analyses gave rise to the long-standing contention that beta2-agonists heighten the risk for cardiovascular (CV) events.12 An analysis of a large healthcare database suggested that new usage of a long-acting beta2-agonist (LABA) was associated with a 31% increase in CV events among the elderly.13 This was not considered surprising given the mechanisms of action and potential side effects (eg, elevated heart rate) of LABAs.12 On the other hand, a post hoc analysis of the TORCH (Towards a Revolution in COPD Health) trial reported that salmeterol used alone or in combination with an inhaled corticosteroid (ICS) did not increase CVD events among patients with moderate to severe COPD.6 In fact, combination therapy was associated with a 17% lower risk of all CVD adverse events compared with placebo, and there was no excess CV risk in the small number of patients with a prior history of MI. These findings have been supported by a recent meta-analysis, which also suggested that treatment with a LABA actually decreases fatal CVD events.14 While these results are encouraging, they do not resolve the debate given that most participants enrolled in prior clinical trials were likely at lower CVD risk than real-world patients with COPD.11 In this context, the SUMMIT (Study to Understand Mortality and MorbidITy) in COPD trial was designed to investigate the health effects of an ICS, a LABA, as well as their combination, specifically among patients with moderate COPD who had or were at high risk for CVD.15 The primary endpoint (all-cause mortality) was not significantly affected by combination therapy (HR 0.88, 95% CI 0.74 to 1.04; p=0.14) although a secondary endpoint (rate of decline in postbronchodilator forced expiratory volume in 1 s (FEV1)) was reduced.16 Here, we present the detailed results regarding the other prespecified secondary endpoint of CVD events as well as the cardiac safety profile of the individual treatments.
Methods
SUMMIT was a prospective, double-blind, parallel-group, placebo-controlled, event-driven (1000 deaths from any cause), randomised trial conducted at 1368 centres in 43 countries. Details regarding the trial design and primary results have been previously published.15 16 In brief, eligible participants included current or former smokers (≥10 pack-years) between the ages of 40 and 80 years, with a history of COPD and a postbronchodilator FEV1 ≥50 and ≤70% of the predicted value, a ratio of postbronchodilator FEV1 to forced vital capacity ≤0.70, and a score ≥2 on the modified Medical Research Council dyspnea scale. Patients were additionally required to have a history, or be at increased risk, of CVD. CVD was defined as coronary artery disease, peripheral arterial disease, prior stroke or MI, or diabetes mellitus with target organ disease.15 Increased CV risk was defined as being ≥60 years plus receiving medications for two or more of the following: hypercholesterolaemia, hypertension, diabetes mellitus or peripheral vascular disease. While ICS and LABA treatments were discontinued before study entry, other COPD medications were permitted during the trial. Participants were then allocated equally to one of four randomised treatments: placebo, fluticasone furoate (FF, 100 µg), vilanterol (VI, 25 µg) or their combination (FF/VI, 100/25 µg) inhaled once daily as a dry powder. A total of 16 485 patients were enrolled and included in the final intent-to-treat (ITT) efficacy population.
In addition to the primary outcome of all-cause mortality by ITT analysis, a prespecified secondary composite CV efficacy endpoint (CV death, MI, stroke, unstable angina and transient ischaemic attack (TIA)) was also evaluated for patients on study treatment. Categorisation of the cause of each death was adjudicated by a clinical endpoint committee who also adjudicated whether any reported CVD event met the definition of the secondary endpoint.15 Individuals discontinuing study treatments, who remained in the primary ITT analysis, could not be assessed for the adjudicated secondary CV endpoints as follow-up visits were not performed and only data regarding mortality were available. Adverse events were also reviewed at each study visit by the study investigators and coded using the Medical Dictionary for Regulatory Activities (MedDRA version 18.0; International Federation of Pharmaceutical Manufacturers and Associations, Geneva, Switzerland). Adverse events of special interest are those associated with the known pharmacological action of a medication (eg, ICS or LABA therapy). For CV adverse events, Standardised MedDRA Queries are available for specific adverse events of special interest. These are predefined MedDRA-derived lists of preferred terms that allow a comprehensive review of safety data not limited to a specific preferred term.
To control for multiplicity of testing, a closed testing procedure (gatekeeper) approach was used. The hierarchy was the primary endpoint followed by the rate of decline in FEV1, followed by the composite CV endpoint. Since significance at the 5% level was not achieved for the primary endpoint, tests for the composite CV endpoint were interpreted as descriptive only. Kaplan-Meier graphs were produced, comparing the time to between-treatment groups, for both the reported and adjudicated CVD events. Details of CVD events were tabulated by treatment group. A Cox proportional hazards regression model was used to analyse the time to the first adjudicated on-treatment composite CV event, with the covariates of age, sex, an indicator for ischaemic heart disease (previous MI or previous coronary revascularisation of any type) and an indicator for vascular disease (previous TIA, stroke, arterial bruits, or medication and/or surgery for carotid or aortofemoral arterial disease). Patients were divided into a number of subgroups, and a comparison of the time to first CVD event for patients on treatment with combination therapy versus placebo was performed using a separate Cox model for each subgroup, and the results presented in a forest plot.
Results
Safety information was collected from 16 568 patients who were randomised and took study medication. Five centres were closed before the study ended because of failure to meet the standards of Good Clinical Practice and ethical practice, and data from their 83 patients were excluded from the efficacy analysis. Thus, a total of 16 485 patients were included in the ITT population (table 1). The study patients were predominately middle-aged white men, with roughly half remaining active smokers. Mean screening blood pressure levels were controlled and more than half of all patients were receiving antiplatelet agents, statins and renin–angiotensin system inhibitors. A total of 182 patients did not meet CV entry criteria but were included in both primary and secondary analyses. Among all participants in the efficacy analysis, 3535 (21%) were ≥40 and <60 years with CVD, 8127 (49%) were ≥60 years with CVD, and 4641 (28%) were ≥60 years old with increased CV risk only (ie, no prior history of CVD). By our prespecified definition, 11 662 (71%) patients had CVD. Excluding those with diabetes plus target organ disease (n=701) from this definition yields 10 961 (66%) patients who had ‘overt’ CVD (eg, prior MI).
Screening characteristics of study participants
Adjudicated CV outcomes
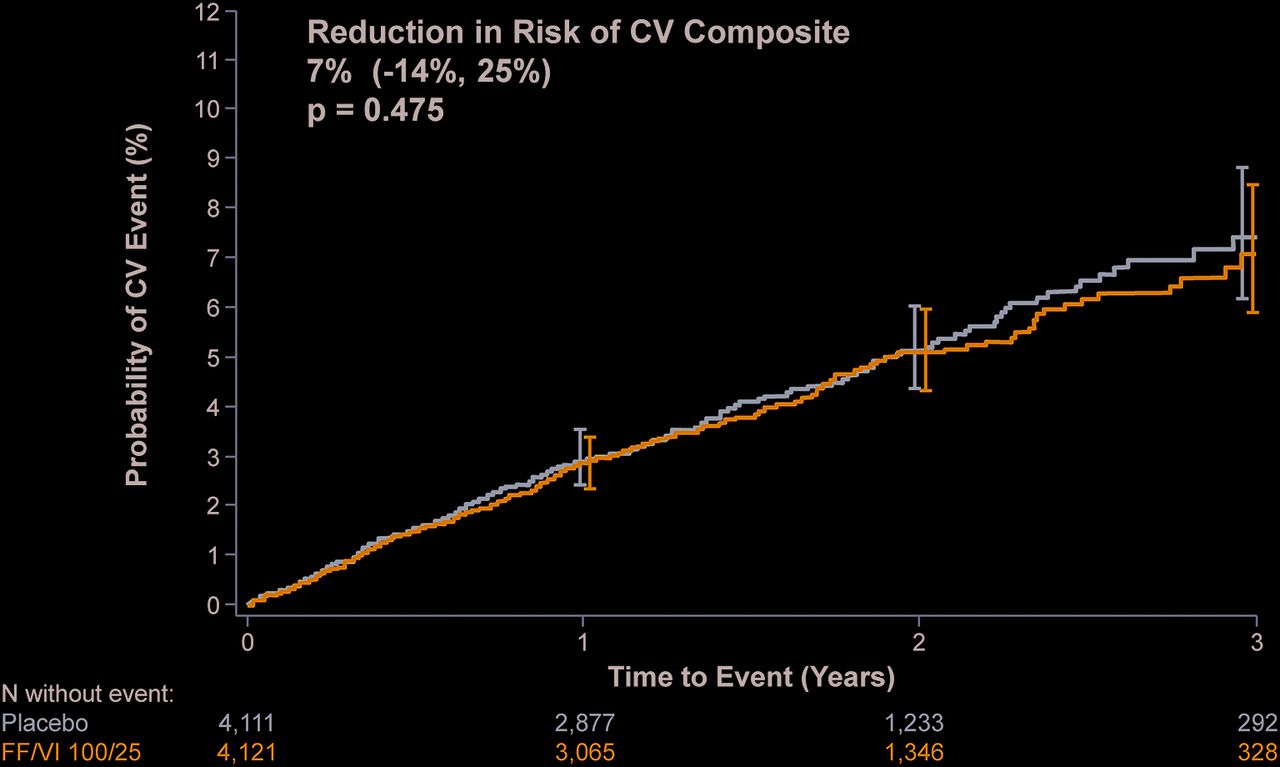
The composite CVD endpoint occurred in 688 patients; for 240 (35%) patients the first event was sudden death, for 256 patients (37%) it was acute coronary syndrome, and for 161 patients (23%) it was stroke or TIA. The proportions of patients with an on-treatment composite CV endpoint as well as the individual component events were similar across treatment groups (table 2). Combination therapy had no effect on the time to first composite CV endpoint compared with placebo (HR 0.93, 95% CI 0.75 to 1.14; p=0.48) (figure 1). Similarly, time to first composite CV endpoint in the FF (HR 0.90, 95% CI 0.72 to 1.11; p=0.32) and VI (HR 0.99, 95% CI 0.80 to 1.22; p=0.91) groups did not differ from placebo (figure 2). There was no evidence for differences in the HRs for the composite CV outcome among subgroups of patients on treatment with combination therapy versus placebo, in particular, between those patients with CVD compared with those with only CV risk (figure 3).
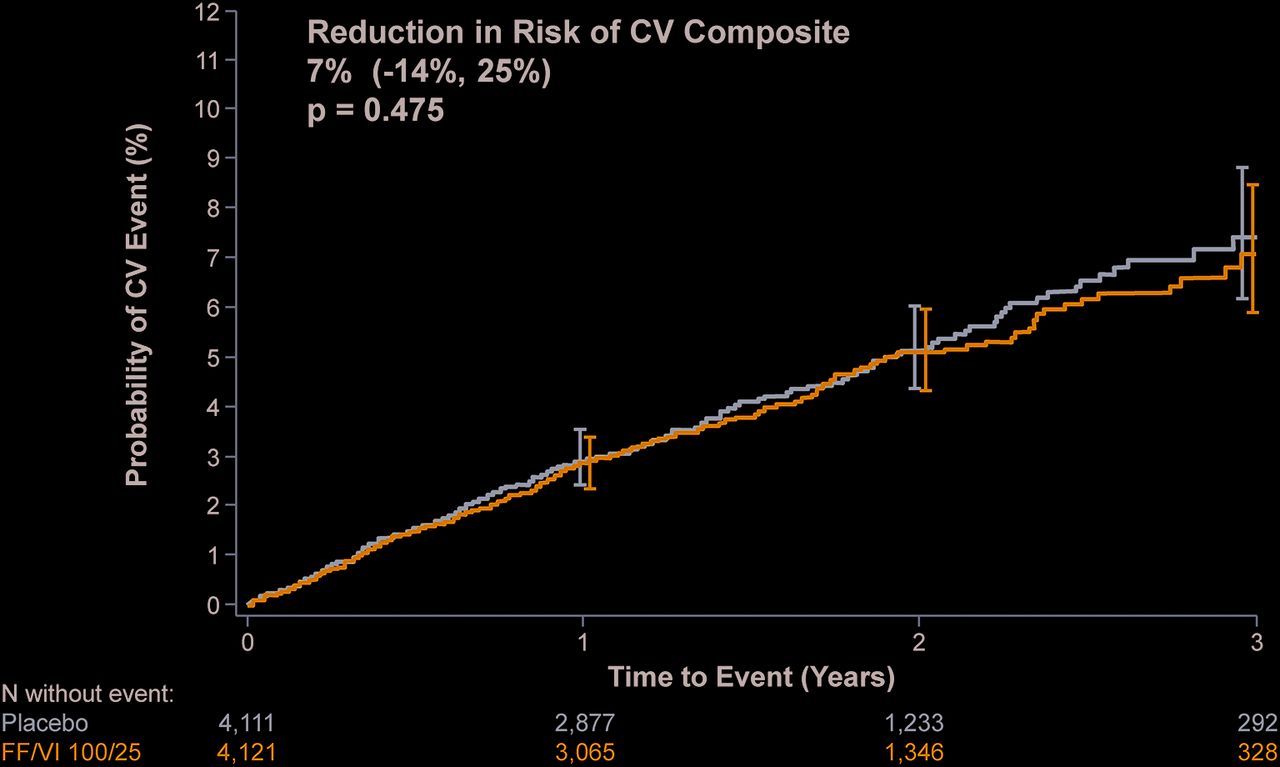
Risks of adjudicated composite CV endpoints in patients treated with combination therapy versus placebo Kaplan-Meier graph for the time to first adjudicated on-treatment composite CVD event (CVD death, myocardial infarction, stroke, unstable angina or TIA) for patients on treatment with combination therapy (VI plus FF) versus placebo. CV, cardiovascular; CVD, cardiovascular disease; FF, fluticasone furoate; TIA, transient ischaemic attack; VI, vilanterol.

Risks of adjudicated composite CV endpoints for all treatment groups. Kaplan-Meier graph for the time to first adjudicated on-treatment composite CVD event (CVD death, myocardial infarction, stroke, unstable angina or TIA) for patients on treatment with VI, FF, combination therapy and placebo. CV, cardiovascular; CVD, cardiovascular disease; FF, fluticasone furoate; TIA, transient ischaemic attack; VI, vilanterol.

Risks of adjudicated composite CV endpoints in subgroups treated with combination therapy versus placebo forest plot of the HRs and 95% CIs for the adjudicated composite CV endpoint in subgroups of patients on treatment with combination therapy versus placebo. Cardiovascular entry criteria with CVD defined as at least one of the following: coronary artery disease, peripheral arterial disease, previous stroke, previous MI or diabetes mellitus with target organ disease. Regions are defined in online supplementary table 3. Ischaemic heart disease indicator defined as previous MI or previous revascularisation of any type; vascular disease indicator defined as previous TIA, stroke, arterial bruits, or medication and/or surgery for carotid or aortofemoral vascular disease. ‘n’ represents number of patients in combined FF/VI and placebo arms shaded regions show overall 95% CI. CV, cardiovascular; CVD, cardiovascular disease; FF, fluticasone furoate; MI, myocardial infarction; TIA, transient ischaemic attack; VI, vilanterol.
Number of patients with adjudicated cardiovascular events in treatment groups*
CV safety parameters
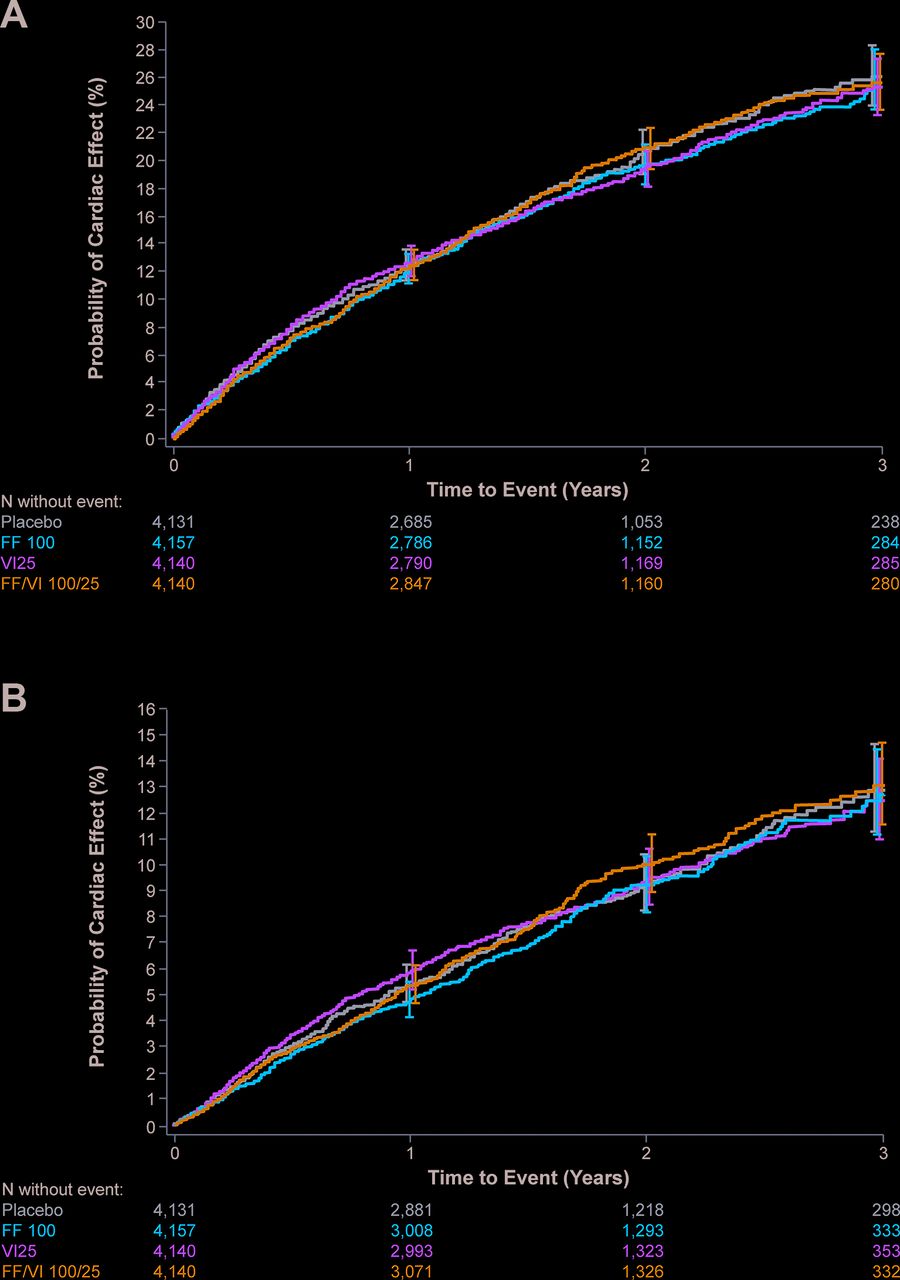
The proportion of participants on treatment reporting any adverse CVD event of special interest during the trial was similar among all groups: placebo (17%), FF (17%), VI (17%) and combination therapy (18%). Reported incidence of arrhythmia (5%, 6%, 5%, 5%), hypertension (5%, 5%, 5%, 6%), cardiac failure (5%, 4%, 4%, 5%), ischaemic heart disease (4%, 4%, 4%, 4%) and any cerebrovascular (2%, 2%, 2%, 2%) adverse events was also similar across placebo, FF, VI and combination treatment, respectively. Serious adverse CVD events of special interest were reported in 8% of all groups. Full details of the adverse and serious adverse CVD events are presented in online supplementary tables 1 and 2. The time to first reported on-treatment adverse CVD event of special interest did not differ among treatment groups (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risks of reported adverse cardiovascular events among treatment groups. Kaplan-Meier graph for time to first reported on-treatment (A) adverse and (B) serious adverse cardiac events of special interest in patients on treatment with VI, FF, combination therapy and placebo. Cardiovascular adverse events of special interest are defined as any untoward medical occurrence falling within Standardised MedDRA (Medical Dictionary for Regulatory Activities) Queries of cardiac arrhythmias, hypertension, cardiac failure, ischaemic heart disease, or central nervous system haemorrhages and cerebrovascular conditions. Details are provided in online supplementary table 1. Serious cardiovascular adverse events of special interest are defined as above as those that also result in death or are life threatening or require hospitalisation or result in disability. Details are provided in online supplementary table 2. FF, fluticasone furoate; VI, vilanterol.
Discussion
The safety and efficacy of inhaled therapies for COPD, especially LABAs, among patients with heightened CV risk has been a long-standing concern.11–13 These findings from SUMMIT provide much needed clinical trial evidence that an inhaled LABA (VI), ICS (FF) and their combination pose no excess CV risks. There were no significant treatment effects on the prespecified secondary composite CV endpoint. Although the original hypothesis was that combination therapy would reduce CVD events compared with placebo, the null results taken in conjunction with the overall favourable safety data support the contention that these inhaled therapies can be safely prescribed as clinically indicated to treat moderate COPD even in patients with, or at high risk for, CVD.
Relationship between COPD and CVD
Patients with COPD are much more likely to have, and die from, underlying CVD than the general population.2–5 Shared risk factors (eg, smoking, advanced age), overlapping biological pathways (eg, systemic inflammation, autonomic imbalance) and common genetic predispositions may help explain part of the association between COPD and CVD. Acute exacerbations of COPD per se (eg, hypoxia, stress) and delays in the diagnosis and management of acute coronary syndromes (eg, difficulties in differentiating the cause of chest pain) may play added roles in explaining the heightened CVD risk of patients with both diseases.7–9 It has also been a long-standing contention that the inhaled therapies for COPD themselves may further potentiate CV events.11–13
Although few studies have evaluated the CVD safety of ICS therapy, many short-term trials12 and large administrative datasets13 have raised concerns regarding possible harm of LABA treatment. Even a ‘highly selective’ beta2-receptor agonist could be detrimental to susceptible patients through chronotropic and proarrhythmic actions.10 11 On the other hand, the TORCH study provided some of the first clues that LABA treatment is safe and might actually reduce CVD events in some patients.6 These observations have also been supported by a recent meta-analysis.14 Our findings from SUMMIT provide some of the most robust clinical trial evidence to date that an ICS (FF), LABA (VI) and their combination appear to be safe, even among patients with, or at high risk for, CVD. There was no evidence to support benefit or harm on the secondary composite CV outcome, nor did a wide array of safety parameters differ among the various treatment groups. We interpret these results to indicate that healthcare providers should be reassured about treating patients for COPD as clinically indicated (ie, to reduce exacerbations) even if they are also at heightened CVD risk. Since this is a common scenario due to the highly prevalent overlap between CVD and COPD, our findings are of key clinical relevance.
Strengths and limitations
This is the first COPD outcome trial to specifically enrol patients with, or at heightened risk for, CVD. This is also the first trial to include a prespecified secondary outcome of composite CVD events among such patients. The primary SUMMIT publication presented only the main trial results.16 This current report significantly adds to the literature as here we present the full details in regard to all CVD outcomes (a prespecified secondary outcome) and safety data. Given high prevalence and overlap of CVD and COPD in the population,2–6 a thorough understanding of the risks and benefits of treating COPD with inhaled therapies is of major clinical importance.10 11
Since the trial did not meet its primary endpoint (all-cause mortality) of superiority, the secondary composite CV results must be correctly interpreted as descriptive or hypothesis generating. An a priori hypothesis of ‘non-inferiority’ of the treatments versus placebo may have provided even further reassurance of their safety from a statistical standpoint. Whether these results represent a class effect applicable to other LABA, ICS or combination therapies is currently unknown. It also remains unclear if these findings can be extrapolated to patients with more severe COPD or with additional high-risk cardiac conditions (eg, recent acute coronary syndrome, heart failure and arrhythmias). The CVD risks related to inhaled anticholinergic therapies were not evaluated by SUMMIT, and it also remains a contentious issue with mixed evidence.17–20 Nevertheless, SUMMIT is one of the largest outcome trials where patients with COPD are at heightened CV risk and its findings are applicable to a number of patients who have concomitant CVD with COPD and as such its findings may help inform clinical decision making. The use of secondary preventive medicines including aspirin, beta blockers and statins (table 1) for the 66% of patients with overt CVD is overall reasonable and indeed matches or exceeds that observed in most real-world settings globally.21 To this point, the influence of risk factor control (eg, blood pressure level) and medication usage (eg, beta blockers) on the health outcomes and their interactions with the health effects induced by the inhaled therapies will be evaluated in future analyses of the SUMMIT trial data. Finally, the use of short-acting beta-agonist therapy, including as rescue inhalers, was not evaluated in this study and requires further investigation regarding its CV safety.
Conclusions
Treatment of moderate COPD with an inhaled LABA (VI), ICS (FF) and their combination appears to be safe among patients at heightened CV risk. Healthcare providers should be more reassured about prescribing evidence-based inhaler therapies as indicated for the management of moderate COPD in people with, or at heightened risk of, CVD.
Key messages
What is already known on this subject?
Patients with chronic obstructive pulmonary disease (COPD) commonly have or are at high risk for cardiovascular disease (CVD). Published studies supporting the safety of inhaled COPD treatments, particularly beta2-agonists, in such patients have reported mixed findings.
What might this study add?
We demonstrate in a prespecified secondary analysis of a large randomised double-blind clinical trial that once-daily usage of an inhaled long-acting beta-agonist, corticosteroid and their combination is safe and significantly impacts CVD outcomes in patients with moderate COPD who have or are at high risk for CVD.
How might this impact on clinical practice?
These findings support that healthcare providers can be more reassured about prescribing these inhaled therapies as clinically indicated to treat moderate COPD even in patients at heightened CVD risk.
References
Footnotes
Acknowledgements The authors acknowledge the work of Veramed employees: Matthew Jones, Abigail Fuller and Nick Cowans on statistical analysis and programming.
Contributors RDB, PMAC, BRC, FJM, JV, DEN, JAA, CC and JY conceived and designed the research; JAA performed statistical analysis; JAA, CC and JY handled funding and supervision; RDB drafted the manuscript; JAA, PMAC, BRC, CC, MAD, SM, FJM, SR, JV, JY and DEN made critical revisions of the manuscript for key intellectual content.
Funding Funded by GSK Study 113782 (NCT01313676).
Competing interests RDB, PMAC, BRC, FJM, JV and DEN are external members of the SUMMIT Steering Committee. JAA, CC and JY are employed by GSK and are members of the SUMMIT Steering Committee. MAD and SM are members of the SUMMIT Clinical Endpoint Committee, and SR is a member of the SUMMIT Independent Data Monitoring Committee.
Ethics approval The study was approved by local ethics committees and was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.
Provenance and peer review Not commissioned; externally peer reviewed.