Article Text

Abstract
Objective We studied evolving antithrombotic therapy patterns in patients with newly diagnosed non-valvular atrial fibrillation (AF) and ≥1 additional stroke risk factor between 2010 and 2015.
Methods 39 670 patients were prospectively enrolled in four sequential cohorts in the Global Anticoagulant Registry in the FIELD-Atrial Fibrillation (GARFIELD-AF): cohort C1 (2010–2011), n=5500; C2 (2011–2013), n=11 662; C3 (2013–2014), n=11 462; C4 (2014–2015), n=11 046. Baseline characteristics and antithrombotic therapy initiated at diagnosis were analysed by cohort.
Results Baseline characteristics were similar across cohorts. Median CHA2DS2-VASc (cardiac failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled)-vascular disease, age 65–74 and sex category (female)) score was 3 in all four cohorts. From C1 to C4, the proportion of patients on anticoagulant (AC) therapy increased by almost 15% (C1 57.4%; C4 71.1%). Use of vitamin K antagonist (VKA)±antiplatelet (AP) (C1 53.2%; C4 34.0%) and AP monotherapy (C1 30.2%; C4 16.6%) declined, while use of non-VKA oral ACs (NOACs)±AP increased (C1 4.2%; C4 37.0%). Most CHA2DS2-VASc ≥2 patients received AC, and this proportion increased over time, largely driven by NOAC prescribing. NOACs were more frequently prescribed than VKAs in men, the elderly, patients of Asian ethnicity, those with dementia, or those using non-steroidal anti-inflammatory drugs, and current smokers. VKA use was more common in patients with cardiac, vascular, or renal comorbidities.
Conclusions Since NOACs were introduced, there has been an increase in newly diagnosed patients with AF at risk of stroke receiving guideline-recommended therapy, predominantly driven by increased use of NOACs and reduced use of VKA±AP or AP alone.
Trial registration number NCT01090362; Pre-results.
- Stroke
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is associated with a fivefold increase in stroke risk.1 Strokes associated with AF have a poorer prognosis compared with non-AF stroke.2 Evidence-based guidelines for stroke prevention in AF recommend anticoagulant (AC) therapy for patients with additional stroke risk factors,3–5 but AC therapy is underused in eligible patients.6 Furthermore, data from registries suggest that AC therapy is underused in patients at high stroke risk and potentially overused in those at low stroke risk.7–11
The most recent European and North American guidelines for the management of AF incorporate recommendations on using non-vitamin K antagonist oral ACs (NOACs) as an alternative to vitamin K antagonists (VKAs).3–5 In the present study, the evolving patterns of antithrombotic therapy were investigated using data from a large, prospective, global cohort study of patients with newly diagnosed non-valvular AF in different countries, geographic regions, care settings, and in patients at different levels of stroke and bleeding risks.
Methods
Study design and participants
The Global Anticoagulant Registry in the FIELD-Atrial Fibrillation (GARFIELD-AF) is an ongoing, prospective, observational, worldwide study of adults with recently diagnosed non-valvular AF from 1215 sites in 35 countries. The study design has been described previously.12 Briefly, men and women aged ≥18 years with non-valvular AF diagnosed according to standard local procedures within the previous 6 weeks and ≥1 additional risk factor for stroke as judged by the investigator are eligible. These risk factors are not prespecified in the protocol, nor are they limited to the components of existing risk stratification schemes. Patients with a transient reversible cause of AF and those for whom follow-up is not envisaged or possible are excluded. Enrolment takes place in five independent, sequential cohorts. To minimise recruitment bias, investigator sites were selected randomly from representative care settings in each participating country and consecutive patients were enrolled. Sample size calculations are based on the 95% confidence intervals for estimates of each of the registry endpoints.12
This paper reports cross-sectional data at baseline including treatment patterns before and after the introduction of NOACs, for cohorts 1–4 (cohort 1: March 2010 to October 2011; cohort 2: August 2011 to June 2013; cohort 3: April 2013 to October 2014; cohort 4: March 2014 to July 2015), and has been written according to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.
Data collection
The electronic case report form (eCRF) was designed by Dendrite Clinical Systems Ltd (Henley-on-Thames, UK). Oversight of operations and data management was conducted by the sponsor and coordinating centre (Thrombosis Research Institute—TRI, London, UK), with support from Quintiles (Durham, North Carolina, USA), The University of Birmingham Department of Primary Care Clinical Sciences (Birmingham, UK), Thrombosis Research Group—Brigham and Women's Hospital (Boston, Massachusetts, USA), and AIXIAL (Paris, France). The GARFIELD-AF protocol requires source data verification of 20% of eCRFs, an electronic audit trail for all data modifications, and additional audit of critical variables.12 Data for the analysis in this report were extracted from the study database on 3 August 2015.
Definitions
The term AC includes VKAs and NOACs. The term NOAC includes oral direct factor Xa inhibitors (FXaIs) and oral direct thrombin inhibitors (DTIs). Vascular disease was defined as peripheral artery disease and/or coronary artery disease (CAD) with a history of acute coronary syndromes. Hypertension was defined as a documented history of hypertension or blood pressure >140/90 mm Hg. Chronic kidney disease (CKD) was classified according to the National Kidney Foundation's Kidney Disease Outcomes Quality Initiative (NKF KDOQI) guidelines:13 moderate-to-severe includes stages III to V; none or mild includes all other patients. Congestive heart failure (CHF) was defined as a history of CHF for patients in cohorts C1 and C2; from C3 onwards there was a protocol amendment and in these cohorts, CHF consists of current or prior history of CHF.
Ethics statement
Independent ethics committee and hospital-based institutional review board approvals were obtained, as necessary, for the registry protocol. The registry is being performed in accordance with the principles of the Declaration of Helsinki, local regulatory requirements, and the International Conference on Harmonisation–Good Pharmacoepidemiological and Clinical Practice guidelines. All patients gave written informed consent to participate.
Statistical analysis
The analysis provides descriptive statistics to summarise data patterns. Continuous variables are expressed as mean±SD and categorical variables as frequency and percentage. Treatment patterns were analysed by cohort, by cohort and CHA2DS2-VASc (cardiac failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled)-vascular disease, age 65–74 and sex category (female)) score,14 and by cohort and ‘modified’ HAS-BLED (hypertension, abnormal renal/liver function (1 point each), stroke, bleeding history or predisposition, labile international normalised ratios, elderly (>65), drugs/alcohol concomitantly (1 point each)) score15 (fluctuations in international normalised ratios were not collected). The risk scores were calculated retrospectively. NOAC use (relative to VKA) was analysed according to patient characteristics, comorbidities, and cohort. Patients in cohorts C2, C3, and C4 using VKA or NOACs were included in the analysis. We removed patients in C1, since NOACs were not globally available during this time period. Adjusted odds ratios were estimated using a logistic model based on the following variables: gender, age group, race, smoking, CHF, hypertension, diabetes, CAD, vascular disease, dementia, moderate-to-severe CKD, non-steroidal anti-inflammatory drug (NSAID) usage, history of bleeding, previous stroke/transient ischaemic attack (TIA)/systemic embolism (SE), and cohort. Multiple Imputation by Chained Equations (MICE) was used to fill in missing values, creating five complete datasets.16 ,17 First-degree interaction between baseline characteristics and time (cohort) or between comorbidities and time (cohort) were tested using likelihood ratio tests. Only significant interactions were included in the final model.
Both SAS V.9.4 (SAS Institute Inc, Cary, North Carolina, USA) and Stata Statistical Software: Release 14 (StataCorp, College Station, Texas, USA) were used for the data analysis.
Results
Study population
Between March 2010 and July 2015, 39 670 patients were enrolled in four sequential cohorts: C1 (2010–2011), n=5500; C2 (2011–2013), n=11 662; C3 (2013–2014), n=11 462; C4 (2014–2015), n=11 046. Baseline characteristics across the four cohorts were similar, although C3 and C4 had a slightly lower prevalence of prior stroke/TIA (table 1).
Baseline characteristics of patients in cohorts 1 to 4
Antithrombotic therapy use by cohort
Figure 1 shows the prescribing patterns at diagnosis of AF in all four cohorts. The proportion of patients on AC therapy at diagnosis, with or without an antiplatelet (AP) agent, increased from C1 to C4. This rise was due to increasing use of NOACs, with or without AP, and was greater for FXaIs than for DTI. At the same time, there was a decline in the use of VKA, with or without AP, as well as AP therapy alone, while the proportion of patients not receiving antithrombotic therapy remained unchanged. Table 2 shows the baseline characteristics for all patients by treatment group. Patients receiving no treatment were generally younger and healthier, with a lower incidence of comorbidities, and had lower CHA2DS2-VASc and HAS-BLED scores.
Baseline characteristics of patients in cohort 1 to cohort 4 by antithrombotic treatment type

Antithrombotic treatment at diagnosis by cohort. The total population represented by n excludes unknowns. AP, antiplatelet; DTI, direct thrombin inhibitor; FXaI, factor Xa inhibitor; VKA, vitamin K antagonist.
Table 3 shows the baseline characteristics of patients on NOACs by cohort. Patients treated early after the introduction of NOACs (C1) were more likely than those in later cohorts to suffer from significant underlying disease such as CAD, vascular disease, CKD, and diabetes. Analysis of the baseline characteristics of 20 167 patients in the later cohorts (C2, C3, and C4) who were prescribed either VKA or NOACs found that NOAC use was more frequent than VKA use in men, patients of Asian ethnicity, the elderly, patients with dementia, those using NSAIDs, and current smokers (table 4). VKA use was more common in patients with cardiac, vascular, or renal comorbidities.
Baseline characteristics of patients on NOACs by cohort
Use of NOACs in relation to baseline characteristics for patients on AC at baseline (n=20 167)
Antithrombotic therapy use according to risk score
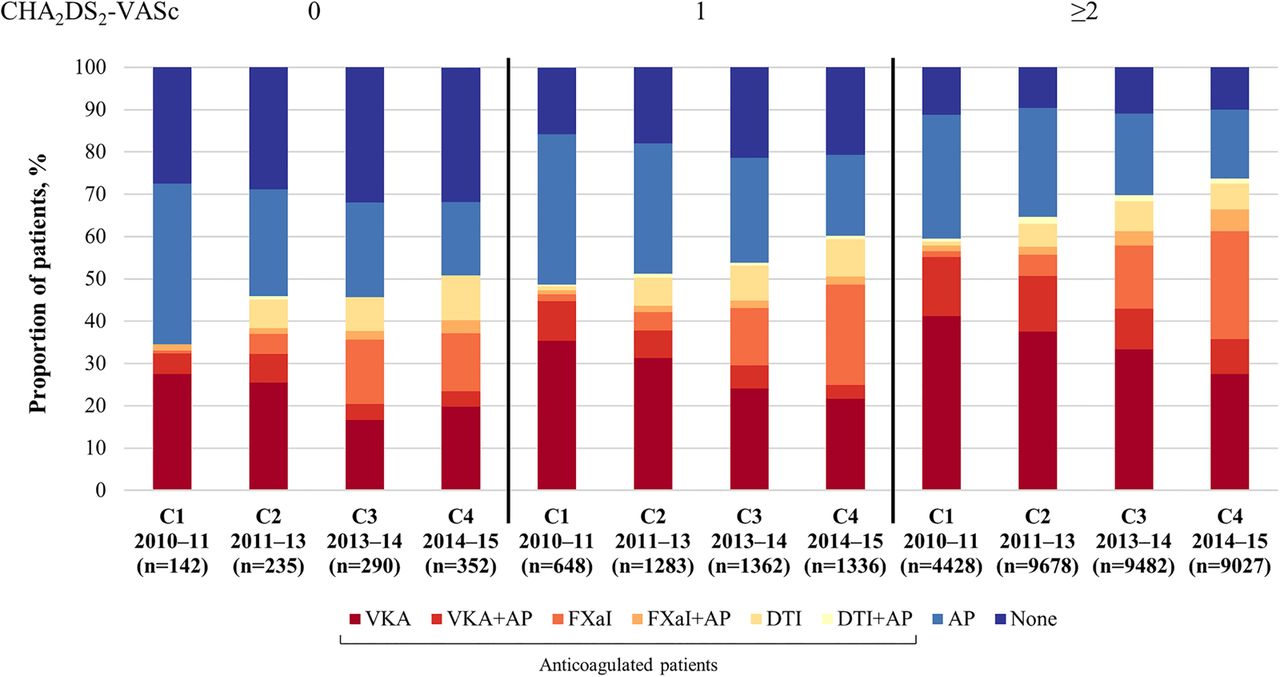
Use of antithrombotic therapy stratified by CHA2DS2-VASc score and cohort is shown in figure 2. Regardless of cohort, the proportion of patients on AC therapy increased with CHA2DS2-VASc score. Although the highest levels of anticoagulation were observed in patients with a CHA2DS2-VASc score ≥2, the increase in anticoagulation from C1 to C4 was greatest in patients with a score of 0. NOAC prescribing increased between C1 and C4 in all CHA2DS2-VASc score strata.

Antithrombotic treatment at diagnosis by CHA2DS2-VASc score and cohort, for patients with a score of 0, 1, and ≥2. The total population represented by n excludes unknowns. Patients with missing CHA2DS2-VASc score: C1 94; C2 369; C3 210; C4 216. AP, antiplatelet; CHA2DS2-VASc, cardiac failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled)-vascular disease, age 65–74 and sex category (female); DTI, direct thrombin inhibitor; FXaI, factor Xa inhibitor; VKA, vitamin K antagonist.
Stratifying treatment by HAS-BLED score (figure 3), the proportion of patients on AC therapy decreased with increasing score, especially beyond a score of 2. In contrast, higher HAS-BLED scores were associated with a greater proportion of patients on AP therapy alone or in combination with an AC. As the HAS-BLED score increased, the proportion of patients on no treatment rose.

{kind=link}
{kind=link}
{kind=link}
Antithrombotic treatment at diagnosis by HAS-BLED score,* for patients with a score of 0, 1, 2, and ≥3, in all cohorts combined. The total population represented by n excludes unknowns. Patients with missing HAS-BLED score: C1 1939; C2 4360; C3 2878; C4 2392. AP, antiplatelet; DTI, direct thrombin inhibitor; FXaI, factor Xa inhibitor; *‘modified’ HAS-BLED, hypertension, abnormal renal/liver function (1 point each), stroke, bleeding history or predisposition, elderly (>65), drugs/alcohol concomitantly (1 point each); VKA, vitamin K antagonist.
Discussion
Data from the GARFIELD-AF cohorts collected over the past 5 years show a pronounced change in the pattern of antithrombotic therapy prescribing in patients with newly diagnosed AF. The use of AC therapy has increased and exceeds 70% in the most recent cohort. This change is predominantly due to increasing use of NOACs. Thromboprophylaxis with AP and VKA therapies alone and in combination has declined.
This paradigm shift in prescribing practice has been driven in part by the availability of NOACs, but also the realisation that APs are barely effective compared with ACs. Evaluating the professional society guidelines published over the last 5 years (especially relating to AP therapy),3 ,4 ,18–22 it is notable that the Japanese guidelines, for example, no longer recommend AP for stroke prevention in patients with AF. European Society of Cardiology and National Institute for Health and Care Excellence (NICE) guidelines also restrict the use of aspirin and other AP therapies for patients who refuse anticoagulation. American College of Cardiology/American Heart Association and Canadian guidelines have curtailed their recommendations on the use of these agents.4 ,21 ,22
Changes in AC therapy have occurred despite initial reluctance on the part of healthcare payers due to the greater cost of NOAC medication compared with VKA or AP therapy. However, the evidence suggests that long-term therapy with NOACs may be cost-effective compared with VKA treatment,23 ,24 primarily due to lower monitoring costs and reduced numbers of patients with strokes and SE.
CHA2DS2-VASc score analysis showed an increase in the use of NOAC therapy at all levels of risk, including those patients with a score of 0. While this may indicate some level of overtreatment, it should be noted that the patients with AF recruited into GARFIELD-AF were judged by their physician to have at least one additional risk factor for stroke. Patients may also have been prescribed ACs for transient purposes such as cardioversion or AF ablation. HAS-BLED score analysis found that AC prescribing diminished as bleeding risk increased, and a surprisingly high frequency of AP therapy alone or combined with ACs was still prescribed.
Notably, we have previously shown that there are no gender differences in the treatment patterns of patients (in C1 and C2).25 Patients treated early after the introduction of NOACs (cohort C1) were more likely than those in later cohorts to suffer from significant underlying disease. Analysis of the later cohorts found that NOACs were more frequently used than VKAs in the elderly and in those with dementia or taking NSAIDs, perhaps because of their ease of use and the perceived lower bleeding risk. The preferential use of NOACs in patients of Asian ethnicity may have been an attempt to lower the incidence of intracranial haemorrhage. A higher frequency of patients with hypertension, CAD, and diabetes was prescribed VKAs, possibly combined with AP therapy, since experience with the combination of NOAC and AP is limited.26 Patients with CKD were more likely to receive VKAs, presumably because of the moderate-to-high dependency of NOACs on renal elimination. It appears that, despite compelling evidence for the use of NOACs in secondary prevention,27–30 prescribers remain relatively wary of NOAC thromboprophylaxis in patients with prior thromboembolic events, predominantly stroke.
The acceptance of AC therapy in AF among physicians is a positive step. However, there has been no decrease in the proportion of patients that receive no antithrombotic treatment, which remains at about 10% of the population. This population includes some patients at high thromboembolic risk, with low HAS-BLED scores, for whom anticoagulation would seem to be appropriate.
GARFIELD-AF provides a unique picture of prescribing at the end of the VKA-only era, showing the global increase in NOAC prescribing. Our findings are strengthened by protocol-mandated source data verification of 20% of eCRFs and central monitoring, ensuring high data quality. A limitation of this study is that only global patterns of antithrombotic therapy were investigated. Regional differences in prescribing trends were not taken into account, nor was the rate of NOAC approvals across each region. Comorbidities were also likely confounders, which were not fully assessed in this analysis.
Conclusion
Since the introduction of NOACs, newly diagnosed at-risk patients with AF are more often receiving guideline-recommended therapy, driven by increased use of NOACs and less treatment with AP and VKA therapies.
Key messages
What is already known on this subject?
Atrial fibrillation (AF) is associated with a fivefold increase in stroke risk. Anticoagulant (AC) therapy is known to reduce this risk in patients with AF, but evidence shows that it is underutilised.
What might this study add?
In this large, global, observational study of patients with newly diagnosed non-valvular AF and ≥1 additional risk factor for stroke, we investigated prospectively the changing pattern of antithrombotic therapy over the past 5 years, before and after the introduction of non-vitamin K antagonist oral ACs (NOACs). Since the introduction of NOACs, there has been an increase in newly diagnosed patients with AF at risk of stroke receiving guideline-recommended therapy, predominantly driven by increased use of NOACs and reduced use of vitamin K antagonists±antiplatelet therapy or antiplatelet therapy alone.
How might this impact on clinical practice?
The acceptance of AC therapy in AF among physicians is a positive step. However, there has been no change in the proportion of patients that receive no antithrombotic treatment, including apparently eligible patients at high stroke risk and low bleeding risk.
Supplemental material
Acknowledgments
We thank the physicians, nurses, and patients involved in the GARFIELD-AF registry. We would also like to thank the following people who were involved in the preparation of this manuscript: Bernard J Gersh (Mayo Medical School, Rochester, USA) and Keith AA Fox (University of Edinburgh, Edinburgh, UK) for their work in the audit of GARFIELD-AF data; Antonello Ciccarone (TRI, London, UK), SAS programming support; Claire Aukim-Hastie, Emily Chu, and Rae Hobbs (TRI, London, UK), medical writing support.
References
Footnotes
Collaborators The full list of GARFIELD-AF Investigators are listed in an online supplementary file which is available with this article.
Contributors AJC, J-PB, DAF, SZG, SG, SH, GK, LGM, FM, AGGT, FWAV, and AKK contributed to the study design. GAm, DA, EB, FC, SZG, YK, and SO contributed to data acquisition. GAc analysed the data. All authors contributed to data interpretation. AJC drafted the report. All authors critically reviewed the report and approved the final manuscript.
Funding The GARFIELD-AF registry is sponsored by the TRI, London, UK, and is supported by an unrestricted research grant from Bayer Pharma AG, Berlin, Germany (AKK). The funding source had no involvement in the data collection, data analysis, or data interpretation.
Competing interests AJC: advisor to Bayer, Boehringer Ingelheim, Pfizer/BMS, and Daiichi Sankyo. GAm: advisor to Merck, Menarini, and Angelini. DA: personal fees from Bayer Healthcare, BMS/Pfizer, Boehringer-Ingelheim, and MSD. J-PB: personal fees from Aspen. FC: personal fees from Bayer, BMS, and Boehringer-Ingelheim. DAF: personal fees from BMS/Pfizer, Boehringer-Ingelheim, Daiichi Sankyo, and Bayer. SZG: grants from BiO2 Medical, Boehringer-Ingelheim, Bristol Meyers Squibb, BTG EKOS, Daiichi Sankyo, National Heart Lung and Blood Institute of the National Institutes of Health, Janssen, and Thrombosis Research Group; personal fees from Bayer, Boehringer-Ingelheim, Bristol Meyers Squibb, Daiichi Sankyo, Janssen, and Portola. SG: personal fees from the TRI, Bayer, and AstraZeneca; grants from Sanofi and Pfizer. SH: personal fees from Aspen, Bayer Healthcare, BMS/Pfizer, Daiichi-Sankyo, and Sanofi. YK: grants and personal fees from Daiichi Sankyo and Boehringer-Ingelheim; personal fees from Bayer, Bristol-Meyers Squibb, and Pfizer. LGM: grants and personal fees from Bayer Healthcare and Pfizer; grants from Boehringer Ingelheim; personal fees from Daiichi Sankyo. FM: employee of Bayer Pharma AG. SO: consultant/advisory board payments from Bayer Pharma AG, Bristol-Myers Squibb Korea, Boehringer-Ingelheim Korea, Pfizer Korea, Sanofi-Aventis, and St Jude Medical. AGGT: personal fees from Bayer Healthcare, Janssen Pharmaceutical Research & Development LLC, Astellas, Portola, and Takeda. FWAV: personal fees from Bayer Healthcare, Daiichi-Sankyo, BMS/Pfizer, and Boehringer-Ingelheim. AKK: grants and personal fees from Bayer Healthcare; personal fees from Boehringer-Ingelheim Pharma, Daiichi Sankyo Europe, Sanofi SA, Janssen.
Patient consent Obtained.
Ethics approval Independent ethics committees and hospital-based institutional review boards.
Provenance and peer review Not commissioned; externally peer reviewed.