Article Text

Abstract
Introduction The Rapid Access Chest Pain Clinics (RACPC) system has become an important way of assessing patients who present with chest pain to their primary care physician. Based on standard protocols up to 50% are discharged with a diagnosis of non-cardiac pain and re-assured. This abstract reviews the longer term outcomes of such patients.
Aims and Objectives We sought to determine the proportion of patients discharged from the University Hospital of Leicester (UHL) RACPC with non-cardiac chest pain, and retrospectively determine the outcomes of these patients specifically with regards to mortality, re-admission with acute coronary syndromes or re-attendance at a cardiology outpatient clinic.
Methods All patients reviewed in the UHL RACPC and discharged with a diagnosis of non-cardiac chest pain between 2010 and 2013 were followed-up for 1 year. Data regarding hospital readmission was obtained from UHL Hospital Episode Statistics. The coded diagnosis for cardiac readmissions was confirmed with review of discharge summaries. Clinic letters and investigations were reviewed for patients who were subsequently referred to cardiology outpatients following discharge from RACPC.
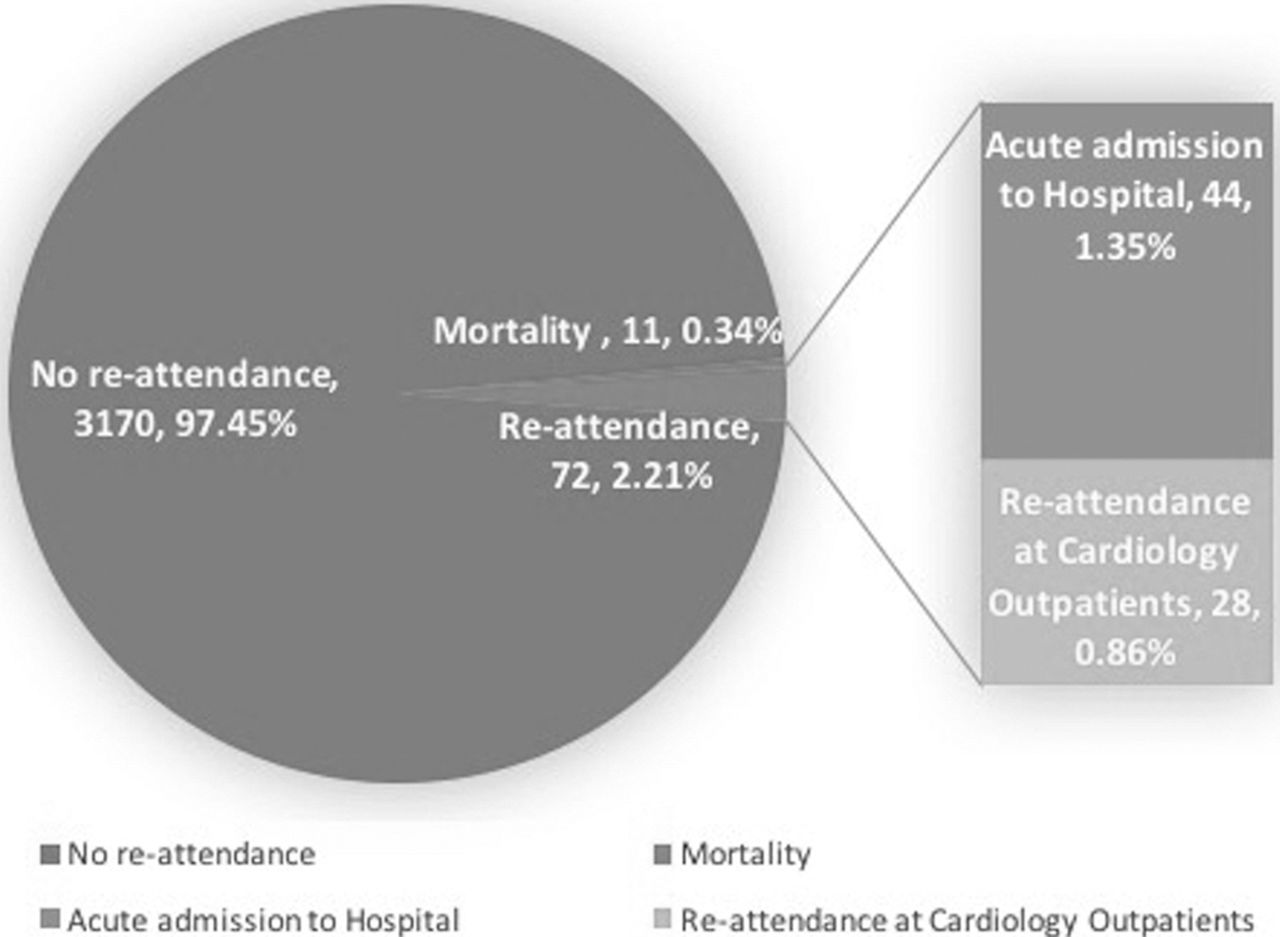
Results Of 7066 patients seen in the RACPC clinic between 2010–2013. 3253 were discharged with a diagnosis of non-cardiac chest pain (46.0%), and consistent/year (2010-2011%–45.8%, 2011-2012%–47.0%, 2012-2013%–45.2%). Outcomes are summarised in fig 1. Follow-up was 12 monthsfor death and re-admission, and 6 months for re-attendance at cardiology OP clinic. Readmission: The 12 month acute readmission rate for patients discharged was 1.4% (44/3253) with most for non-cardiac causes (28 patients). Only 8 patients were readmitted for acute coronary syndromes (0.24% of discharged patients). Non-ACS cardiac admissions (8 patients) were predominantly for arrhythmias (table 1). None of the patients readmitted with ACS or non-ACS cardiac condition died within 1 year of discharge from RACPC. Re-attendance at cardiology outpatients: 28 patients (0.86%) were seen in the cardiology outpatient clinic 6 months following discharge from RACPC. 74% of these patients underwent further cardiac investigations (fig 2), however only 7 patients were diagnosed with ischaemic heart disease (0.2% of patients discharged from RACPC). Mortality: 11 patients (0.3%) died within one year of discharge from the RACPC. Median time from RACPC attendance to death: 210 days (IQR=128 – 285 days). The causes of death included metastatic cancer (4), Large PE secondary to pancreatic cancer (1), acute haemorrhagic pancreatitis (1), Sepsis (2). One recorded death from MI was in the context of sepsis, DKA and CVA.
Conclusions These data show that thorough and accurate assessment of patients with chest pain in the RACPC leads to good outcomes with a subsequent very low hospital admission rate for ACS These are reassuring data.
Abstract 98 Table 1

{kind=link}
{kind=link}
- Chest Pain
- Stable angina
- long-term outcomes