Article Text

Statistics from Altmetric.com
The likelihood of cardiovascular disease (CVD) in both women and men largely is explained by well-known lifestyle and clinical risk factors. Several studies have suggested that a woman’s reproductive history also might affect the risk of CVD, but results have been inconsistent and methodology suboptimal. In this issue of Heart, Peters and Woodward1 report the association between several reproductive factors and subsequent incident CVD over 7 years of follow-up in 482,000 participants in the UK Biobank study with CVD defined as incident myocardial infarction (fatal or non-fatal) or stroke.1 The risk of CVD was increased in women with early menarche (<12 years), early menopause (<47 years), younger age at first birth, or a history of miscarriage, stillbirth or hysterectomy (figure 1). Interestingly, in both men and women, each additional child was associated with an increased risk of CVD with an HR of 1.03 (1.00 to 1.06) in women and 1.03 (1.02 to 1.05) in men.

Penalised spline plots with adjusted HRs (95% CI) for cardiovascular disease associated with women’s age at menarche and age at natural menopause. Analyses are adjusted for age, Townsend deprivation index, smoking status, systolic blood pressure, history of diabetes and body mass index.
Unfortunately, the question of whether any of these associations are causal remains unanswered. For example, the conventional hypothesis that hormonal changes at menopause are the cause of increased CVD risk might not be correct. As the authors note: “It has also been suggested that it is not menopause that adversely affects cardiovascular risk but rather that cardiovascular risk factors determine the age at menopause, possibly through direct effects on the endocrine system or by inducing ischaemic damage in the ovaries.” They go on to recommend that further studies are needed on each of these reproductive factors to identify potential biological, behavioural or social mechanisms that might explain the association with CVD risk.
Prevention of stroke in patients with atrial fibrillation (AF) is of paramount importance, particularly in patients with heart failure. Despite convincing evidence and guideline recommendations supporting use of oral anticoagulation (OAC) for this indication, many patients are not on effective therapy. In a study by Savarese and colleagues2 that included over 21 000 patients with both heart failure and AF in Sweden, only 58% received OAC. Encouragingly the likelihood of OAC treatment was higher with a higher CHA2DS2-VASc score and OAC use was associated with fewer adverse events. However, underuse of OAC was associated with several factors that actually increase risk of stroke including older age, paroxysmal AF, inappropriate use of anti-platelet therapy and more severe heart failure. Other associations with underuse of OAC, such as follow-up by primary care, living alone and lower income suggest inequities in provision of healthcare services.
In addition, as Cowie and Zakeri3 comment in an editorial: ‘The chance of being anticoagulated did rise as the CHA2DS2-VASc score rose, but at a less steep gradient than the chance dropped as the HAS-BLED score rose. In other words, physicians were more influenced by a rise in bleeding risk than they were by a rise in stroke risk. This example of omission bias is well known and is perhaps explained by physicians still being of the mindset that if a stroke occurs, it can be considered ‘natural’ whereas causing a bleed by anticoagulation is iatrogenic and therefore more likely to be perceived as their ‘fault’.’ In order to overcome this bias, Cowie and Zakeri recommend: ‘As international guidelines suggest, we should ensure we detect atrial fibrillation (whether persistent or paroxysmal), make an objective assessment of both the stroke and bleeding risk using an accepted tool, and then seek to have a discussion tailored to the individual patient so that a shared decision can be made on the best way forward for that individual.’
Resting heart rate (RHR) is a simple measure that reflects physical fitness and cardiovascular health. Based on data from over 40 000 patients in the Melbourne Collaborative Cohort Study, Seviiri and colleagues4 found that both RHR, and the change in RHR over a decade, were associated with an increased risk of death from CVD, cancer or other causes (figure 2).

Association of resting heart rate measured at baseline with all-cause and cause-specific mortality, stratified by sex. Cox models were adjusted for age, country of birth, level of education, waist circumference, alcohol consumption, smoking, physical activity score, alternate healthy eating index, total serum cholesterol, sodium-potassium ratio, caffeine, blood pressure, history of hypertension, angina, asthma and diabetes. Interactions between sex and RHR were tested by comparing models with and without interaction terms between sex and RHR, using likelihood ratio tests. P values for interaction: all-cause mortality: p=0.07; in the 90+bpm category: p=0.02; cancer mortality: p=0.72; CVD mortality: p=0.77; other-cause mortality: p=0.55. bpm, beats per minute; CVD, cardiovascular disease; RHR, resting heart rate.
In the accompanying editorial, Nanchen5 suggests “Even if causality is not yet established, clinicians should now screen for abnormal RHR defined as above 70 bpm for men and above 80 bpm for women when they monitor blood pressure in healthy adults. Because it is unknown if targeting RHR using drugs such as beta-blockers or ivabradine will improve prognosis, the most appropriate preventive attitude towards high RHR values may be lifestyle counselling.”
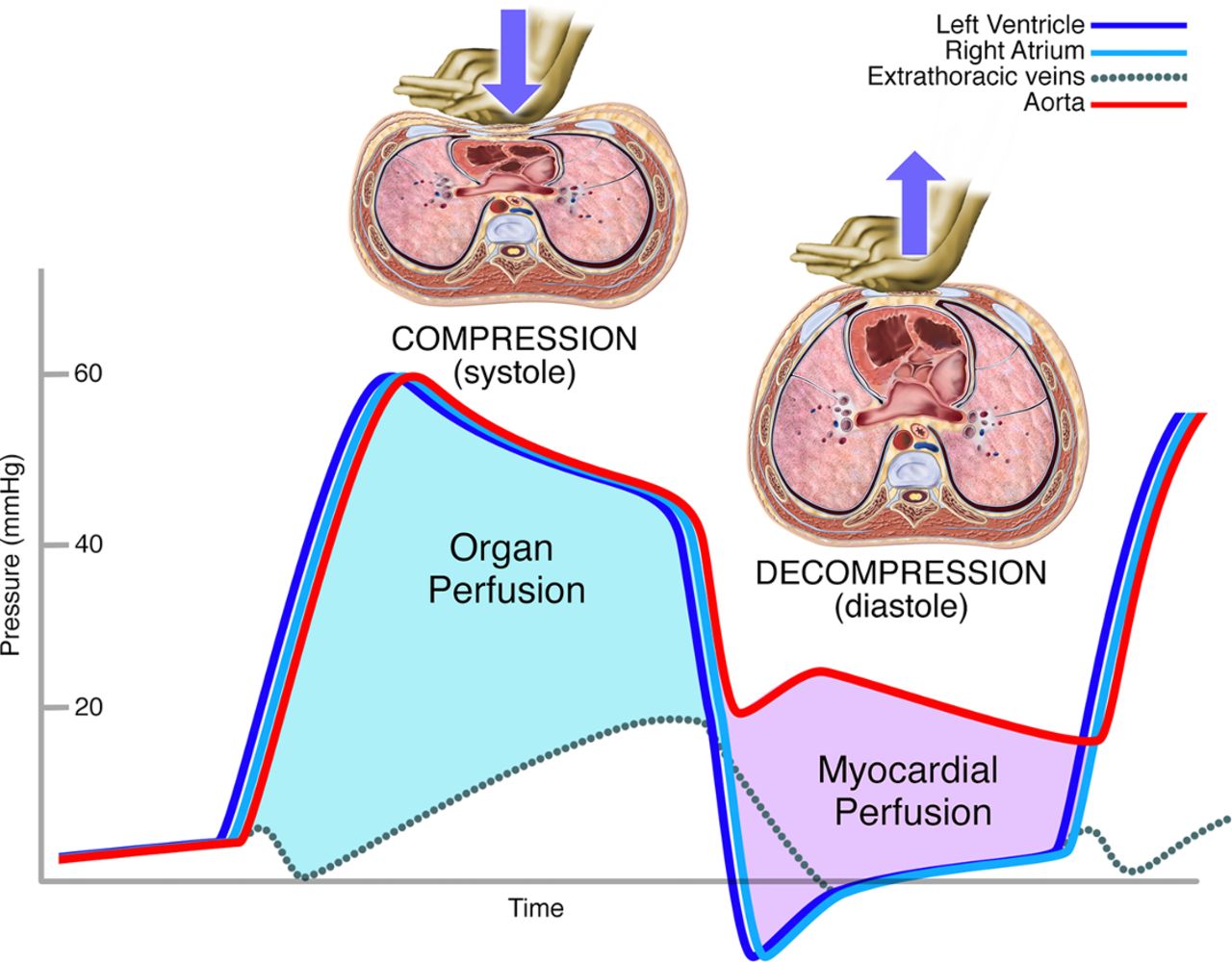
All healthcare providers now consider training in cardiopulmonary resuscitation (CPR) a core competency for patient care. Yet, the effectiveness of CPR varies widely around the world. In a concise review article, entitled ‘Cardiopulmonary resuscitation: the science behind the hands’, Harris and Kudenchuk6 summarise the evidence underlying current recommendations for performing CPR and provide clear explanations of why CPR works (figure 3). Hopefully understanding how it works might improve CPR performance and, ultimately, clinical outcomes.

Haemodynamic effects of compression and decompression phases of cardiopulmonary resuscitation. Compression phase creates organ perfusion pressure (difference between aortic and extrathoracic vein pressure). Decompression phase creates myocardial perfusion pressure (difference between aortic and right atrial pressure). Data adapted from Criley et al.8
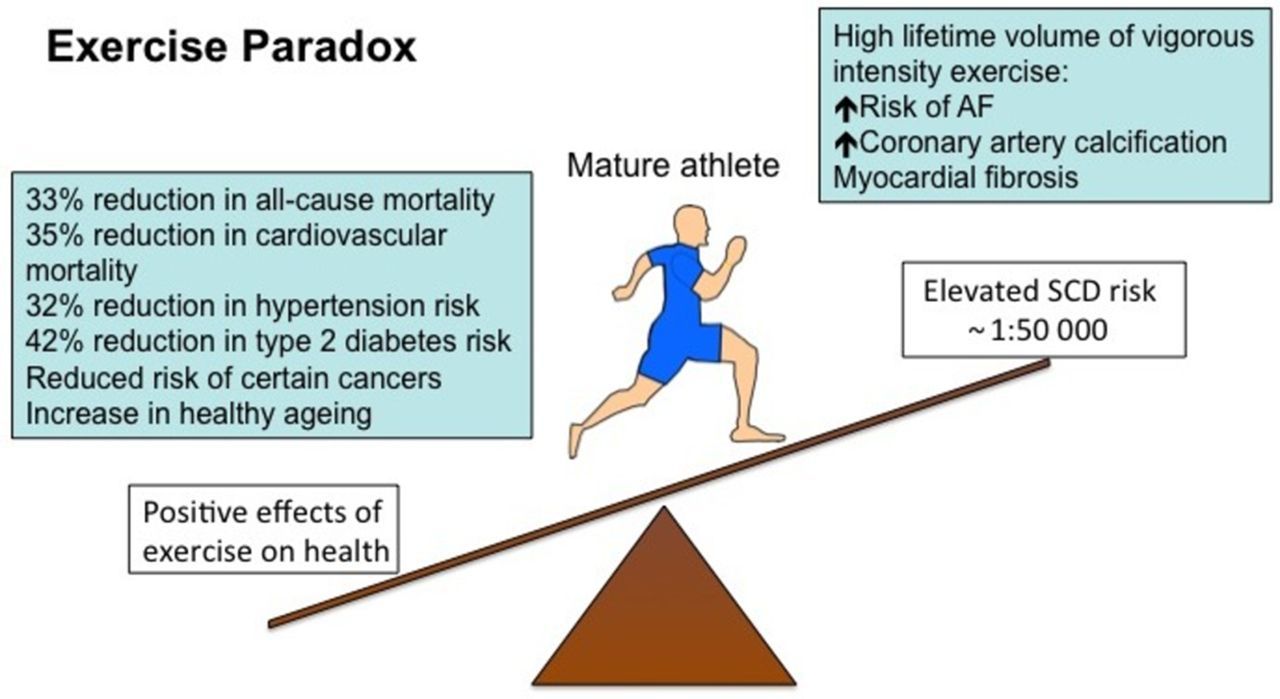
The Education in Heart article in this issue provide an educational review for management of mature athletes,7 including a discussion of the benefits and risks associated with regular high-intensity exercise (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Exercise paradox. AF, atrial fibrillation; SCD, sudden cardiac death.
Footnotes
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; internally peer reviewed.