Article Text

Statistics from Altmetric.com
Bicuspid aortic valve (BAV) disease is common, affecting 1%–2% of the entire population, with nearly all BAV patients eventually requiring aortic valve replacement, often with concurrent aortic surgery for dilation of the sinuses or ascending aorta. Although echocardiography allows easy diagnosis of the presence of BAV disease early in life, we are unable to predict disease progression or aortic dilation in an individual patient and we have no effective therapies to preserve normal valve function.
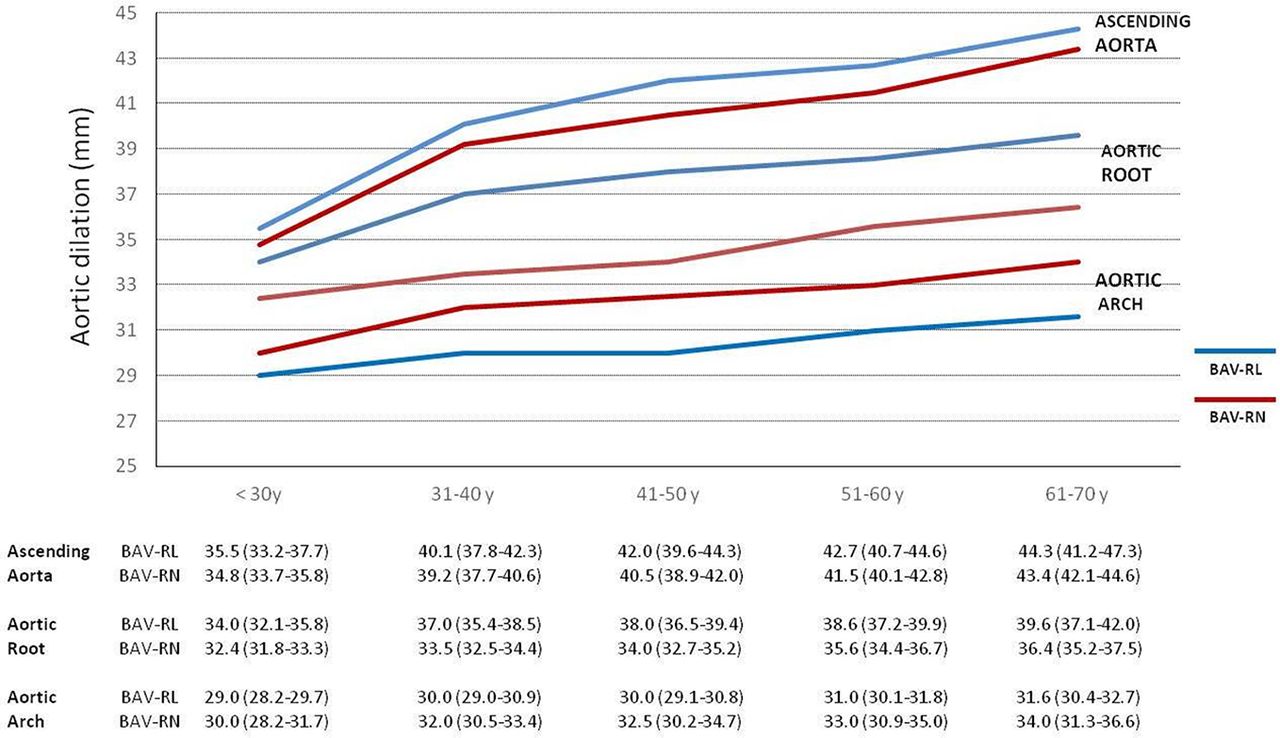
In this issue of Heart, Evangelista and colleagues1 sought to identify phenotypic predictors of valve dysfunction and aortic root dilation in a series of 802 consecutive adults diagnosed with BAV at eight tertiary care hospitals. As in previous studies, BAV leaflet morphology characterised by fusion of the right and left (RL) coronary cusps was most common (73%), followed by fusion of the right and non-coronary cusps (24%). Aortic regurgitation was associated with male sex and leaflet prolapse. Aortic stenosis was associated with RL valve morphology, the presence of a raphe (seen in 82%), age, dyslipidaemia and smoking. Dilation of the ascending aorta was not associated with any specific valve morphology whereas aortic sinus dilation was associated with RL leaflet morphology, male sex, and aortic regurgitation. (figure 1)

Aortic diameters according to age. Graph representing mean aortic diameters at the level of the aortic root, ascending aorta and aortic arch in patients with BAV-RL and BAV-RN. Note the homogeneous enlargement of the diameters over time in the three aorta segments. However, while ascending aorta diameters were similar between BAV types, aortic root diameters were consistently larger in BAV-RL and aortic arch diameters in patients with BAV-RN. Table shows mean and CIs of aortic diameters according to age at the three different aorta levels. BAV, bicuspid aortic valve; RL, right and left; RN, right coronary and non-coronary.
In the accompanying editorial, Krieger and Hung2 raise the concern that “valve morphology and demographics only partially explain the clinical heterogeneity seen in patients with bicuspid aortic valve. The current paper is among the largest and highest quality studies to describe these associations. Nevertheless, even with a large sample size and a core lab to minimise misclassification bias, only relatively small (although significant) differences are seen between bicuspid valve types. Much of the remaining heterogeneity is likely genetic.” They go on to ask: “Can the associations described here and elsewhere help clinicians better manage patients? Unfortunately, it is unlikely. Despite the statistically significant associations between demographics, valve morphology, valve dysfunction and aortic dilation, there remains too much overlap to tailor therapy to valve type.”
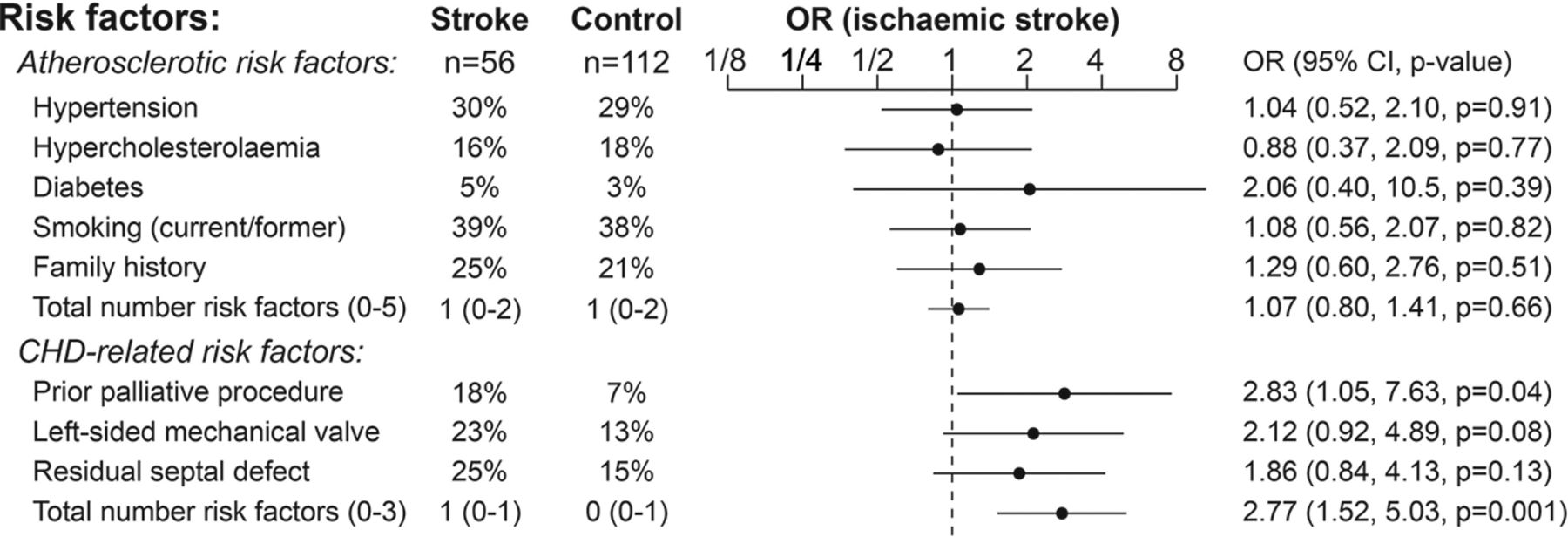
The success of surgical and medical therapy for congenital heart disease means that we now see more older adults presenting with coronary artery disease or stoke who also have underlying adult congenital heart disease (ACHD). To determine if ACHD patients have unique risk factors for adverse cardiovascular events, Bokma and colleagues3 used a case–control design to match 55 ACHD patient with an acute coronary event and 56 cases with stroke to similar adults with coronary disease or a stroke who did not have ACHD. Multivariate analysis showed that in ACHD patients coronary disease was associated with conventional atherosclerotic risk factors. In contrast, stroke was associated with previous shunt operations, residual or unclosed septal defects and left sided mechanical heart valves, suggesting stroke was due to a cardiac embolic event in many of these patients (figure 2).

Factors associated with ischaemic stroke. Univariable logistic regression analysis was performed with ischaemic stroke/transient ischaemic attack as outcome variable. Forest plots displaying OR with 95% CI of different atherosclerotic and congenital heart disease (CHD)-related risk factors. Median number of risk factors displayed with IQR for both groups.
Giannakoulas and Ntiloudi4 point out that ACHD patients have a high risk of stroke compared with the general population. As shown in the study by Bokma and colleagues,3 these patients have additional risk factors for cardioembolic events related to their underlying ACHD anatomy and previous interventions (table 1). The pathophysiology of adverse cardiovascular events in ACHD patients has implications for therapy—first, appropriate risk factor evaluation and primary prevention for coronary disease is essential and, second, we need to address the gap in current recommendations regarding anti-platelet versus anti-coagulant therapy to prevent stroke in ACHD patients, given the additional risk factors for cardioembolic events in this patient group.
Pathophysiology of acquired cardiovascular disease in congenital heart disease
The role of coronary angiography in patients with worsening heart failure remains controversial. In an observational study of 2516 heart failure patients,5 12.5% underwent coronary angiography within 30 days of worsening heart failure symptoms. Factors associated with performance of coronary angiography included hospital admission, an overt acute coronary syndrome, a higher troponin level, younger age and better renal function. Patients who underwent coronary angiography had a lower risk of death (adjusted HR=0.59, 95% CI 0.43 to 0.80, p=0.001) compared with those who did not undergoing coronary imaging. The risk of adverse events was higher in the 34% with a coronary stenosis compared with those with no significant stenosis (adjusted HR for the primary outcome=1.71, 95% CI 1.10 to 2.64, p=0.016).
In an editorial, Petri and Rocchiccioli6 note that previous studies in other populations have shown a similarly low rate of coronary angiography in patients with worsening heart failure. On reviewing the literature and the current study by Ferreira and colleagues,5 they conclude: “the inescapable truth is that little is known of the role of coronary angiography in the diagnosis and treatment of acute or chronic heart failure. There are currently a few answers, but many more questions.”
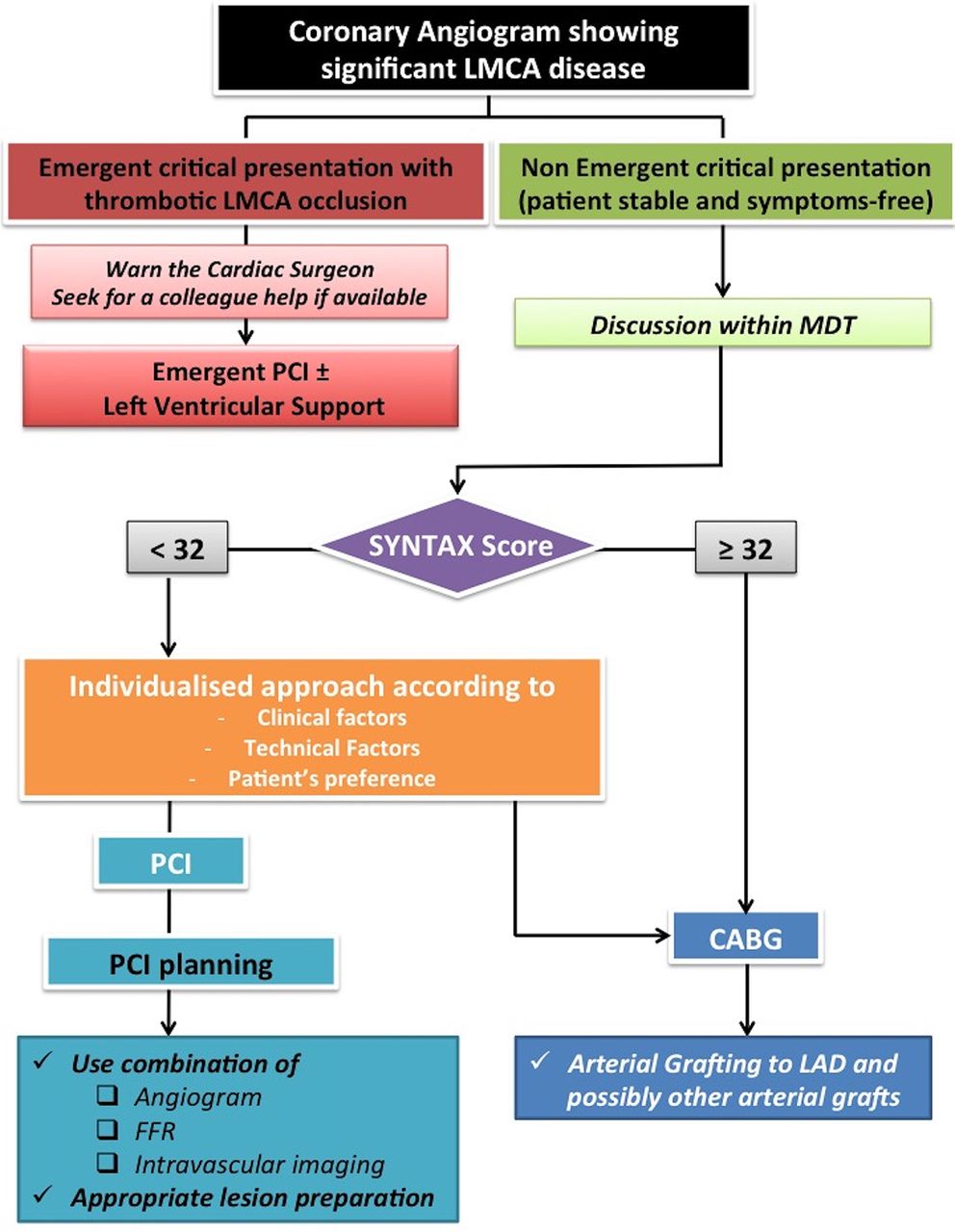
The Education in Heart article7 in this issue discusses coronary stenting for left mainstem coronary artery artery (LMCA) disease. A question and answer format summaries the three principal clinical trials: the Synergy between PCI with Taxus and Cardiac Surgery Substudy (SYNTAX), the Nordic-Baltic-British Left Main Revascularisation (NOBLE) and Evaluation of Xience Versus CABG for Effectiveness of Left Main Revascularization (EXCEL) studies. The authors conclude: ‘With the simultaneous publication of NOBLE and EXCEL studies in 2016, evidence regarding revascularisation in LMCA disease has expanded dramatically. Both trials were large and well conducted, but because of their contrasting results and potential limitations, a uniform recommendation about the relative role of stenting compared with CABG in LMCA disease is inappropriate. A possible algorithm to support and aid the decision-making process is shown in figure 3.”

{kind=link}
{kind=link}
{kind=link}
Decision-making aid for the management of patients with obstructive left main stem disease. CABG, coronary bypass grafting; FFR, fractional flow reserve; LAD, left anterior descending; LMCA, left mainstem coronary artery; MDT, multidisciplinary team; PCI, percutaneous coronary intervention; SYNTAX, Synergy between PCI with Taxus and Cardiac Surgery.
Check out the Image Challenge question in this issue. A unique clinical presentation with diagnostic echo images!8
Footnotes
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; internally peer reviewed.