Article Text

Abstract
The physiological changes during pregnancy predispose a woman for the development of new-onset or recurrent arrhythmia. Supraventricular arrhythmia is the most common form of arrhythmia during pregnancy and, although often benign in nature, can be concerning. We describe three complex cases of supraventricular arrhythmia during pregnancy and review the currently available literature on the subject. In pregnancies complicated by arrhythmia, a plan for follow-up and both maternal and fetal monitoring during pregnancy, delivery and post partum should be made in a multidisciplinary team. Diagnostic modalities should be used as in non-pregnant women if there is an indication. All antiarrhythmic drugs cross the placenta, but when necessary, medical treatment should be used with consideration to the fetus and the mother’s altered pharmacodynamics and kinetics. Electrical cardioversion is safe during pregnancy, and electrophysiological study and catheter ablation can be performed in selected patients, preferably with zero-fluoroscopy technique. Sometimes, delivering the fetus (if viable) is the best therapeutic option. In this review, we provide a framework for the workup and clinical management of supraventricular arrhythmias in pregnant women, including cardiac, obstetric and neonatal perspectives.
- pregnancy
- tachycardia
- supraventricular
- arrhythmias
- cardiac
- atrial fibrillation
- atrial flutter
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Anatomical, haemodynamic and hormonal changes in the maternal physiology make pregnancy a high-risk period for the occurrence of new-onset arrhythmia, or the recurrence of pre-existing arrhythmia. The maternal intravascular volume expands up to 45% throughout pregnancy, to compensate for a fall in systemic vascular resistance that facilitates the formation of the uteroplacental circulation.1 The volume expansion causes atrial and ventricular stretch, which in combination with a physiologically increased heart rate and contractility, increased sympathetic activity and altered catecholamine sensitivity creates an arrhythmogenic state.2–4 Arrhythmia risk peaks in the third trimester.5 Maternal risk factors are previous arrhythmia, advanced maternal age, African ancestry and congenital heart disease, in which surgical scars and aberrant cardiac anatomy compound the situation.6–8
Data on the prevalence of arrhythmia during pregnancy are scarce and conflicting, and lack clarity because complaints of palpitations are common and predominantly benign.4 Arrhythmia was observed in 68 per 100 000 pregnancy-related hospitalisations, which probably underestimates the total prevalence considering the additional cases of arrhythmia without hospitalisation.7 Supraventricular arrhythmias are more common than ventricular arrhythmias and will be the focus of this review.7
Atrial fibrillation or flutter (AF, 31–59 per 100 000 pregnancies) is the most frequently reported arrhythmia in pregnancy, with a growing prevalence in the past two decades that may be partly explained by the increasing maternal age.7 9 Non-AF supraventricular tachycardia (SVT) is reported in 22–33 per 100 000 pregnancies,5 7 10 including atrioventricular (nodal) re-entry tachycardia (AV(N)RT) and atrial tachycardia.
Although most arrhythmias are benign, they are associated with increased maternal mortality (OR 13 for AF and OR 6 for SVT).7 Appropriate workup and multidisciplinary management are therefore important, but the literature to guide clinical decisions is scarce. In this review, we describe three complex cases seen in a tertiary referral centre and provide a step-by-step guide for the management of supraventricular arrhythmias during pregnancy.
Case series
Case 1
A primigravid woman aged 34 years presented at the emergency department of an affiliated secondary care centre with complaints of palpitations at 37 weeks of gestation. She previously had an uneventful pregnancy, had no relevant history of cardiac disease, but was known with Crohn’s disease and hypothyroidism. Her ECG showed a regular SVT of 220 bpm. A short RP narrow complex tachycardia was observed, consistent with AVNRT or atrioventricular re-entry tachycardia (AVRT) (figure 1). She showed no signs of congestion.

ECG of a woman aged 34 years presenting at 37 weeks of gestation with a regular supraventricular tachycardia of 220 bpm with a retrograde P wave, suggestive of an atrioventricular (nodal) re-entry tachycardia. Hyperthyroidism and an atrioventricular re-entry tachycardia with concealed bypass were later discovered.
The patient was admitted and repeatedly treated with adenosine intravenously, with only temporary conversion to sinus rhythm. A cumulative dosage of 7.5 mg of metoprolol intravenously and 50 mg metoprolol orally were given next, without success. After 4 hours of sustained tachycardia, intravenous verapamil was administered to a total amount of 10 mg. The heart rate decreased to 180 bpm, but stable sinus rhythm was not achieved. The patient remained haemodynamically stable and the fetal heart rate pattern on the cardiotocogram (CTG) was reassuring.
In consultation with our tertiary care centre, we decided to eliminate the most-likely trigger of the tachycardia: the pregnancy itself. An uneventful emergency caesarean section was performed, six-and-a-half hours after the patient’s first presentation. After induction of general anaesthesia, the patient spontaneously converted and remained in sinus rhythm. A son of 3206 g (67th percentile) was born with initially low Apgar scores of 4/5/8 at 1/5/10 min, based on transient respiratory insufficiency due to the anaesthesia. After 4 days in the neonatology ward, he was discharged in good health. In the mother, a hyperthyroidism due to oversupplementation of her levothyroxine was diagnosed and treated accordingly. One year later, the patient was seen for preconception counselling and although no recurrence of the AV(N)RT had occurred, an electrophysiological (EP) study was performed. An orthodromic AVRT with a left posteroseptal accessory pathway could be induced and was successfully ablated.
Case 2
A woman aged 35 years, gravida 2 para 1, first presented in a secondary hospital with AF at 12 weeks of gestation. She was known with Marfan syndrome and had undergone an ascending aorta replacement and implantation of a mitral bioprosthesis (for regurgitation) in 2004, followed by a bioprosthesis replacement in 2014. Her current AF was treated with a trans-oesophageal echo-guided electrocardioversion (ECV) and Coumadin, after which she was referred to our centre for further follow-up. At 20 weeks of gestation, a transthoracic echocardiogram showed normal systolic function of the left ventricle, but a moderate stenosis of the mitral valve prosthesis with a mean gradient of 7 mm Hg (figure 2A). A recent prepregnancy MRI of the thoracic aorta showed normal aortic dimensions and good status of her ascending aorta graft, so imaging was not repeated. Our multidisciplinary pregnancy heart team considered her to be in class II–III following the modified WHO (mWHO) maternal cardiovascular risk classification.11 According to the European Society of Cardiology (ESC) guidelines on delivery in women with arrhythmia, she was at low risk for haemodynamic compromise during delivery and rhythm surveillance level 1 was recommended, as for all stable SVT (table 1).11 An elective caesarean section was planned at 39 weeks of gestation, because of a previous caesarean section.

Transthoracic echocardiogram and ECG of a woman aged 35 years with Marfan syndrome and a mitral valve bioprosthesis, presenting at 14 weeks of gestation with atrial fibrillation. (A) Transthoracic echo at 20 weeks of gestation showing parasternal and apical view of the bioprosthesis. Continuous wave Doppler showing a mean peak gradient of 7 mm Hg. (B) ECG showing recurrent atrial fibrillation with rapid ventricular response at 37 weeks of gestation. (C) Continuous wave Doppler at 2 months post partum, showing worsening mitral stenosis with a mean PG of 10 mm Hg of the prosthetic valve and tricuspid regurgitation velocity of 2.4 m/s.
Recommended surveillance levels during delivery in women with supraventricular arrhythmia
However, at 37 weeks of gestation she presented with AF with rapid ventricular response (figure 2B). Beta-blockers were started, and we decided there was an indication for ECV within 48 hours and to expedite the delivery. The ECV was successful, but the therapeutic anticoagulation that is required after ECV would increase the risk of bleeding complications during the caesarean section. Because the fetal heart trace on the CTG remained reassuring, we decided to postpone the delivery for 1 week. Fraxiparine 0.8 mL subcutaneous twice daily was started after the ECV and stopped again 24 hours before the uncomplicated caesarean section. A healthy boy of 3550 g (81st percentile) was born with Apgar scores of 9/10. Coumadin was started 48 hours after surgery and continued for 4 weeks.
Two months post partum, the patient suffered from recurrent palpitations after she decreased the beta-blocker dosage on her own initiative. The echocardiogram showed an increase of the mean gradient of the mitral valve prosthesis to 10 mm Hg, with normal right ventricular pressure (figure 2C). Holter monitoring for 48 hours showed no recurrence of AF, but considering the progressive mitral valve prosthesis stenosis and markedly increased size of the left atrium, we decided to restart Coumadin for the associated thromboembolic risk. One year after delivery, she had a new episode of AF which could be terminated by ECV. An exercise echocardiogram was performed and showed an increase in the mean gradient of the mitral valve prosthesis from 9 mm Hg at rest to 16 mm Hg during exercise. After discussion in the multidisciplinary heart team, she underwent a re-operation and a mechanical mitral valve prosthesis (considering her family was complete) was inserted successfully. No complications occurred during hospitalisation and at latest follow-up, 3 months after surgery.
Case 3
A primigravid woman aged 38 years presented at 16 weeks of gestation at a secondary hospital with palpitations that had increased in intensity during pregnancy. She had no history of cardiac disease. She was diagnosed with an AV(N)RT and treated with metoprolol 12.5 mg twice daily without sufficient effect, after which she was referred to our centre. Here, the ECG showed a regular SVT of 205 bpm with an intermediate axis and a narrow QRS complex (figure 3A). A mid-RP narrow complex tachycardia was observed, consistent with AVNRT, AVRT or less likely atrial tachycardia. The arrhythmia terminated spontaneously, but afterwards many recurrences were observed, provoked by light physical activity. There were no signs of congestion. An echocardiogram showed that there was no structural heart disease.

ECG and echocardiogram of a woman aged 38 years at 16 weeks of gestation, presenting with atrioventricular (nodal) re-entry tachycardia (AV(N)RT). (A) ECG of a regular supraventricular tachycardia of 205 bpm with an intermediate axis and a narrow QRS complex. A retrograde P wave was observed 120 ms behind the QRS complex, suggestive of an AV(N)RT. (B) Subcostal view of an echocardiogram after an electrophysiological (EP) study with ablation for a left lateral concealed bypass atrioventricular re-entry tachycardia, showing moderate pericardial effusion as complication of the EP study.
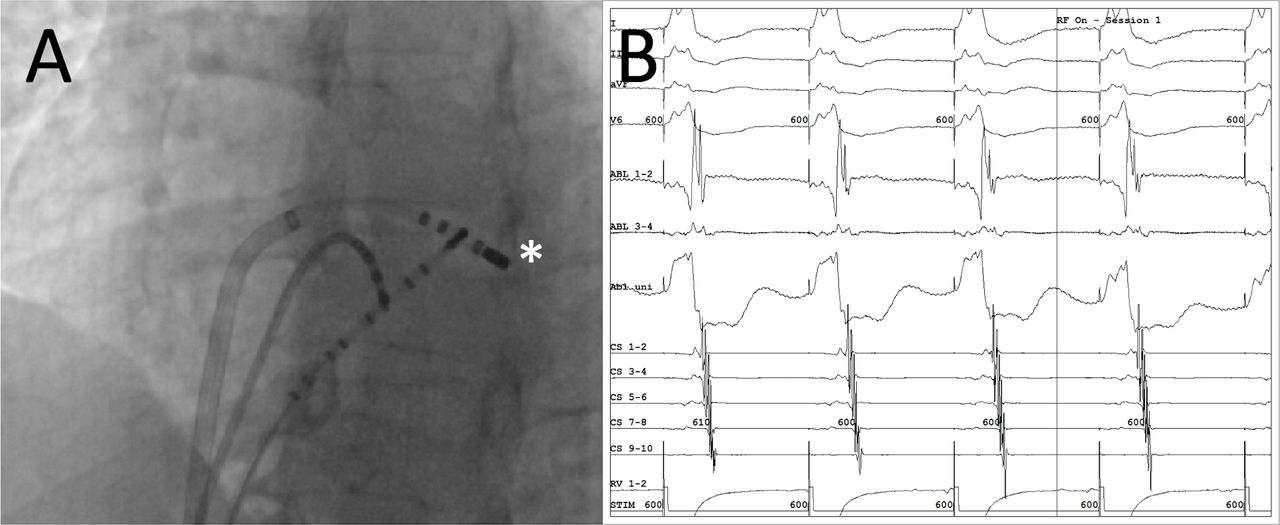
According to the ESC guidelines, our multidisciplinary pregnancy heart team classified her as mWHO II, as all supraventricular arrhythmia without underlying structural heart disease.11 Rhythm-surveillance level 1 was recommended during delivery (table 1). An EP study with ablation was discussed, but we decided to first pursue pharmacological treatment and only perform an ablation in case of refractory complaints. Verapamil 120 mg once daily replaced the metoprolol, and she was advised to avoid excessive exertion. The dosage was gradually increased to 120 mg three times daily, with an acceptable but incomplete result on the frequency and intensity of her complaints. The fetal status and growth were monitored regularly in the obstetric outpatient clinic with CTG and fetal ultrasound, and remained reassuring. Labour was induced at 37 weeks of gestation because of the persisting complaints of arrhythmia. The patient had an uncomplicated delivery of a girl of 3585 g (90th percentile), with Apgar scores of 9/10. Because of the maternal verapamil use during pregnancy and lactation, the neonate was observed for 24 hours. The neonatal heart rate and ECG were normal, while the serum verapamil levels were very low and below therapeutic range (norverapamil <15 μg/L and verapamil <10 μg/L). Two months post partum, an EP study with ablation was performed due to persisting palpitations after delivery. A left lateral concealed bypass with inducible AVRT was ablated (figure 4). Unfortunately, the procedure was complicated by pericardial effusion needing pericardiocentesis (figure 3B). Afterwards she developed a postpericardiocentesis pericarditis, which was treated with analgesia and colchicine.

Electrophysiological study and ablation in a woman with persisting palpitations post partum. (A) Location of catheters in left anterior oblique (LAO) view. The ablation catheter (*) is positioned at the site of successful ablation of the left lateral concealed bypass. (B) Intracardiac electrograms during RV apical pacing at a cycle length of 600 ms. There is an eccentric retrograde atrial activation during RV pacing with earliest activation at the distal coronary sinus. Note the short local ventricular to atrial interval at the site of successful ablation (ABL 1–2). ABL, ablation catheter; CS, coronary sinus; RF, radiofrequency; RV, right ventricle.
Discussion
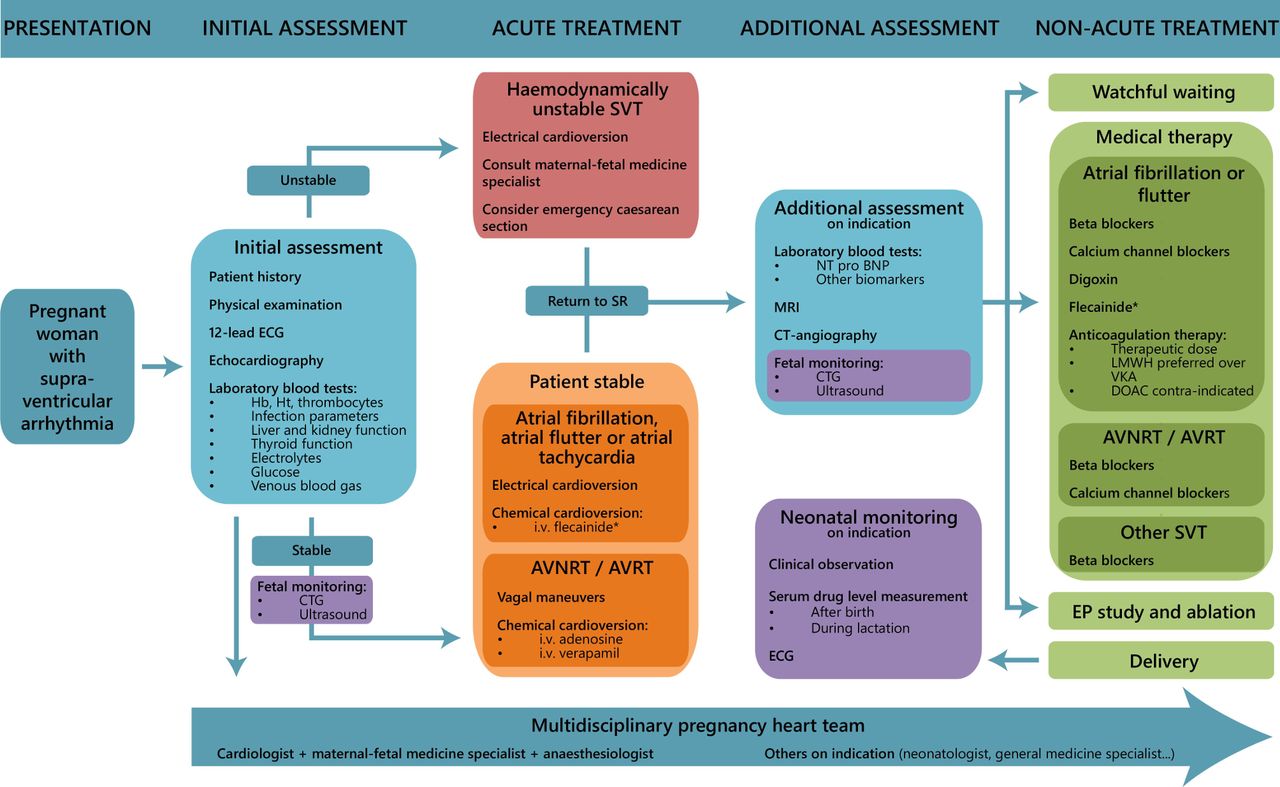
We have described three cases of supraventricular arrhythmia during pregnancy where different forms of intervention were necessary. Figure 5 presents a step-by-step guide for the diagnosis and management of supraventricular arrhythmia in pregnancy. We discuss the current knowledge on the subject, using the cases and the figure as a framework.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow chart of the diagnosis and treatment of supraventricular arrhythmia during pregnancy. *Flecainide is relatively contraindicated in women with structural heart disease, and is also contraindicated in case of atrial flutter due to risk of 1:1 AV conduction. AVNRT, atrioventricular nodal re-entry tachycardia; AVRT, atrioventricular re-entry tachycardia; CTG, cardiotocogram; DOAC, direct oral anticoagulants; EP, electrophysiological; Hb, haemoglobin; Ht, haematocrit; LMWH, low molecular weight heparin; NT-proBNP, N-terminal pro b-type natriuretic peptide; SR, sinus rhythm; SVT, supraventricular tachycardia; VKA, vitamin K antagonist.
Case 1
Although AV(N)RT in pregnancy are usually well tolerated, they can become symptomatic or cause haemodynamic instability, especially in the presence of underlying heart disease. After primary examination with appropriate workup, vagal manoeuvres, pharmacological treatment with adenosine intravenously are the first choice of treatment in the acute setting in haemodynamically stable patients (figure 5). In case of insufficient effect or haemodynamic compromise, ECV is indicated, especially as in pregnancy some medication may be harmful.12
Drugs
All antiarrhythmic drugs (AAD) cross the placenta, although data on fetal toxicity are often limited. If possible, drug therapy may be avoided or postponed until after the first trimester, in which the teratogenic risk is highest, but therapy can be necessary and justified in persisting arrhythmias.12 Due to the altered maternal pharmacodynamics and kinetics, the required drug dosage may be either lower or higher (eg, digoxin, due to increased clearance and volume of distribution) than in non-pregnant women. Table 2 lists the safety during pregnancy and lactation of commonly used drugs for rhythm and rate control and anticoagulation.
Drugs used in the treatment of arrhythmia and their safety during pregnancy and lactation
In case 1, adenosine and verapamil were used, both of which prolong the effective refractory period of the AV node and have a success rate of 90% in terminating acute attacks.13 Alternatively, digoxin or beta-blockers could be used to terminate or supress AV(N)RT. Adenosine can be safely administered in the same dosage as in non-pregnant patients. There are few data on verapamil or diltiazem, but no teratogenicity or maternal side effects during pregnancy are reported.14 Caution is warranted when combining class 1C or 1A because of potentially deleterious negative inotropic and chronotropic effects on mother and fetus.
In case 1, sinus rhythm was established only after the delivery, which shows the crucial role that pregnancy physiology has in provoking the new onset or (frequent) recurrence of arrhythmia. The initial and additional assessment should also consider other triggers, such as anaemia, stress or thyroid dysfunction (figure 5). In AV(N)RT, there are usually no underlying cardiac abnormalities. In case 1, both the hyperthyroidism and the concealed bypass contributed to the arrhythmia. However, the delivery of the child was the most important step and best option in this patient’s treatment, considering her pregnancy was at term gestational age.
Delivery and post partum
Neurohormonal changes and pain during labour stimulate the sympathetic nervous system, which increases the heart rate and contractility.15 The cardiac output is further increased by exertion and fluid shifts. The timing and mode of delivery and surveillance level should be individualised in a delivery plan by a multidisciplinary pregnancy heart team, considering cardiac, obstetric and fetal factors. The ESC guidelines consider paroxysmal SVT, AF and Wolff-Parkinson-White syndrome to be low risk, and consultation of a cardiologist is the only recommendation (table 1).11 Unstable SVTs are classified as medium risk and consultation of a specialised multidisciplinary team, including arrhythmologists, is advised. The mode and location of the delivery are on obstetric indication, although continuous telemetry, intravenous access and an external cardioverter defibrillator should be available.11
Due to physiological fluid shifts or complications such as postpartum haemorrhage, haemodynamic changes in the first days post partum may trigger arrhythmia and even heart failure, especially in case of prepregnancy decreased ejection fraction or valvular disease. Monitoring by 3-lead ECG and vital functions should be continued for at least 24–48 hours after delivery for women with a medium-risk or high-risk pregnancy.16
Preconception counselling
In case 1, the patient received preconception counselling before she started her second pregnancy, and subsequently her AVRT could be ablated before she got pregnant. This illustrates the added value of preconception counselling in women with a history of arrhythmia, or an increased risk of developing it because of structural heart disease. In general, the recurrence rate during pregnancy for women with previous AF is 25%–52%8 and the incidence of AF for women with structural heart disease is 1.3%.17 The recurrence rate of SVT during pregnancy is 50%.8 However, the risk may be higher in patients with more complex cardiac disease, ranging from 0.8% in patients with an atrial septal defect to 15.6% in patients with transposition of the great arteries.18 Besides the recurrence rates, the preconception counselling should educate the patient about the symptoms suggestive of arrhythmia and what they should do in case of complaints. There might be a role for haemodynamic testing as part of preconception counselling, however, data are scarce on what kind of tests are the most informative and what the cut-off values should be to base clinical decisions on.
Case 2
Contrary to other types of supraventricular arrhythmia, AF in a young woman with a structurally normal heart is uncommon and additional cardiac assessment to rule out any underlying structural heart disease is essential (figure 5).19 The most important risk factors are a history of AF (OR 7.1), mitral valve disease (OR 6.9) and left-sided cardiac lesions (OR 2.9).17
Electric cardioversion
In case of sustained supraventricular arrhythmia or haemodynamic instability, ECV is recommended as in non-pregnant women (figure 5).11 20 No deleterious effects of ECV on fetal haemodynamics are reported21 and the risk of inducing fetal arrhythmias or inducing premature labour is deemed very low, but it is recommended to perform CTG monitoring directly after ECV.22 If the cardioversion must be postponed, drug therapy for rate control should be instated and the patient could be observed for 24 hours to see if drug therapy is sufficient as treatment. However, this increases the duration of maternal tachycardia and AADs may have fetal effects (table 2).
Anticoagulation
It is not clear whether the same rules for stroke-prediction risk stratification can be used as in non-pregnant patients,20 because pregnancy should be considered a prothrombotic state because of a physiological increase in clotting factors and a decrease in anticoagulant and fibrinolytic factors.15 In women with congenital heart disease underlying the arrhythmia, thromboembolic risk is increased even in those with a low CHADS2/CHA2DS2 VASc (congestive heart failure, hypertension, age, diabetes, previous stroke/transient ischemic attack (vascular disease)) scores, and therapeutic anticoagulation should be considered.23 Patients with moderate mitral stenosis, like in case 2, may have an increased risk of developing intra-atrial thrombi and if there is also severe left atrial enlargement or spontaneous contrast, we advise low molecular weight heparin (LMWH) in a prophylactic dose. Careful timing of anticoagulation around the period of delivery is crucial because of the bleeding risk. In case 2, we postponed the delivery to allow for enough time after stopping the LMWH and waited for 48 hours to restart Coumadin post partum. Coumadin was restarted considering the combination of the congenital heart disease and pregnancy as thrombogenic risk factors in this patient.
Case 3
In case 3, a high dosage of verapamil was necessary to supress the AVRT, of which the fetal effects are unknown. Therefore, regular follow-up was performed of the fetal heart rate and growth during pregnancy, and post partum the neonate was observed for 24 hours in the neonatology ward.
Fetal and neonatal monitoring
There are few data on the offspring risks after supraventricular arrhythmia during pregnancy. Paroxysmal SVT is associated with low birth weight (OR 1.7), but the attributable effect of the SVT versus the medication used is unclear.24 Consequently, there is no consensus on the requirements for fetal monitoring, which may depend on the type of SVT, the gestational age and the effects of the type of medication used (table 2). Beta-blockers, for example, may cause intrauterine growth restriction, which requires regular monitoring of fetal growth, and also fetal bradycardia and hypoglycaemia, which requires neonatal monitoring post partum.25
In case 3, an EP study was considered but postponed until after the delivery. The procedure was complicated by pericardial effusion that required pericardiocentesis, which illustrates the risks, as this complication would have been even more dramatic during pregnancy.
EP study and catheter ablation
EP study and ablation could be considered in highly selected patients with drug-refractory SVT.11 12 After multidisciplinary team consultation, a careful risk-benefit discussion with the patient should be conducted. EP study might be considered in patients presenting with AV(N)RT, focal atrial tachycardia and cavotricuspid isthmus-dependent atrial flutter, but not for other macrore-entry tachycardia or AF.26 27 If possible, catheter ablation should be performed only in experienced high-volume centres, and either be postponed to the second trimester to avoid radiation exposure in the first trimester, or use a zero-fluoroscopy technique as a successful and safe alternative to conventional fluoroscopy.26 28 29 Overall frequency of cardiac tamponade after EP study is 0.6%.30
Conclusions
Pregnancy creates an arrhythmogenic environment and the pregnant population is increasingly at risk of arrhythmias. Starting at the initial presentation, a multidisciplinary approach is crucial to balance maternal cardiac, obstetric and fetal considerations. In any case, optimal maternal health is a prerequisite for good fetal health, so diagnostic modalities and therapeutic options (such as electrical or chemical cardioversion) should be used where necessary and not be avoided or delayed because of the fetus. Knowledge of the physiology of pregnancy helps to predict the effects and consequences of interventions and drug therapy. A good secondary assessment for underlying causes of arrhythmia, such as structural heart disease or endocrine disorders, should not be forgotten. However, often the pregnancy itself is the most important contributor to the burden of arrhythmia, and the delivery of the child is sometimes a viable therapeutic option.
Ethics statements
Patient consent for publication
Ethics approval
When exclusively describing an individual case history, it is not required to obtain Ethics Committee approval or official exemption by Dutch national law. All patients gave their written informed consent, reviewed their own case description and images and saw the final version of the manuscript.
Footnotes
Contributors Study design: KPR, RMK, NS, JC, JWR-H. Data collection: KPR, RMK, NS, DS, S-CY, MCP. Manuscript draft: KPR, RMK, NS. Critical revision, editing and approval of the final manuscript: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.