Article Text

Statistics from Altmetric.com
Transforming growth factor-β1(TGF-β1) is a multifunctional cytokine that has an important role in the regulation of cell growth, differentiation, and repair in a variety of tissues.1 In addition to its role in the cell cycle and apoptosis, TGF-β1 induces the synthesis of extracellular matrix (ECM) and is upregulated by angiotensin II.1 2 Dilated cardiomyopathy is characterised by myocyte loss, hypertrophy of residual myocytes, increased interstitial fibrosis, and abnormalities of the cytoskeleton.3 Cytotoxic lymphocytes and macrophages are also present in the myocardium in increased numbers which may provide a source of TGF-β1.4 Therefore in this study we have investigated whether patients with chronic heart failure caused by idiopathic dilated cardiomyopathy have increased plasma concentrations of TGF-β1, and whether this is associated with increased macrophage gene expression for TGF-β1compared to those with normal left ventricular function. Patients with ischaemic or hypertensive heart disease were excluded because of the potential confounding effects on TGF-β1 concentrations of atherosclerosis and pressure overload with left ventricular hypertrophy.
Twenty patients who presented with symptoms and signs of chronic heart failure with no obvious cause and with the clinical diagnosis of dilated cardiomyopathy (by the World Health Organization criteria) were studied. All patients had right and left cardiac catheterisation with standard haemodynamic measurements, and coronary angiography was performed to exclude significant valvar, coronary artery disease, hypertensive heart failure, as well as constrictive pericardial disease or restrictive cardiomyopathy before proceeding to right ventricular biopsy. Twenty age and sex matched healthy controls with no evidence of cardiac disease (all with normal echocardiograms) were also studied. Serum TGF-β1 was assayed with an enzyme linked immunosorbent assay (ELISA) (R & D System, Minneapolis, USA) The intra- and interassay coefficient of variation was < 15%. Peripheral blood mononuclear cells were isolated and were resuspended in medium for total cell counting. CD14 cells were isolated using dynabeads M-450 CD14 (Dynal, AS, Oslo, Norway). The cells were incubated at 37°C in a humidified 5% carbon dioxide atmosphere, in the presence of phytohaemagglutinin (10 μg/ml) and Phorbol 12-myristate 13 acetate (1 ng/ml). The cells were harvested at time 0 and 24 hours after stimulation for total RNA extraction. After RNA extraction TGF-β1 gene expression was quantified by the PCR MIMIC method (Clontech, Palo Alto, California, USA). Clontech, primers sequences are: 5' GCC CTG GAC ACC AAC TAT TGC T 3' and 5' AG GCT CCA AAT GTA GGG GCA GG 3'. The PCR product generated from MIMIC fragment has 270 bp while those from target cDNA has 161 bp, and were separated by 1.7–2% agarose gels and stained with ethidium bromide. Densitometry was performed and a standard curve was established by plotting the log value of the band intensity ratio of the MIMIC fragment and the target fragment with log MIMIC molecule number. The initial target molecule number can be calculated and is equal to the MIMIC molecule number when the log band intensity ratio is zero. The value was normalised as cDNA molecule per cell or gram of tissue.
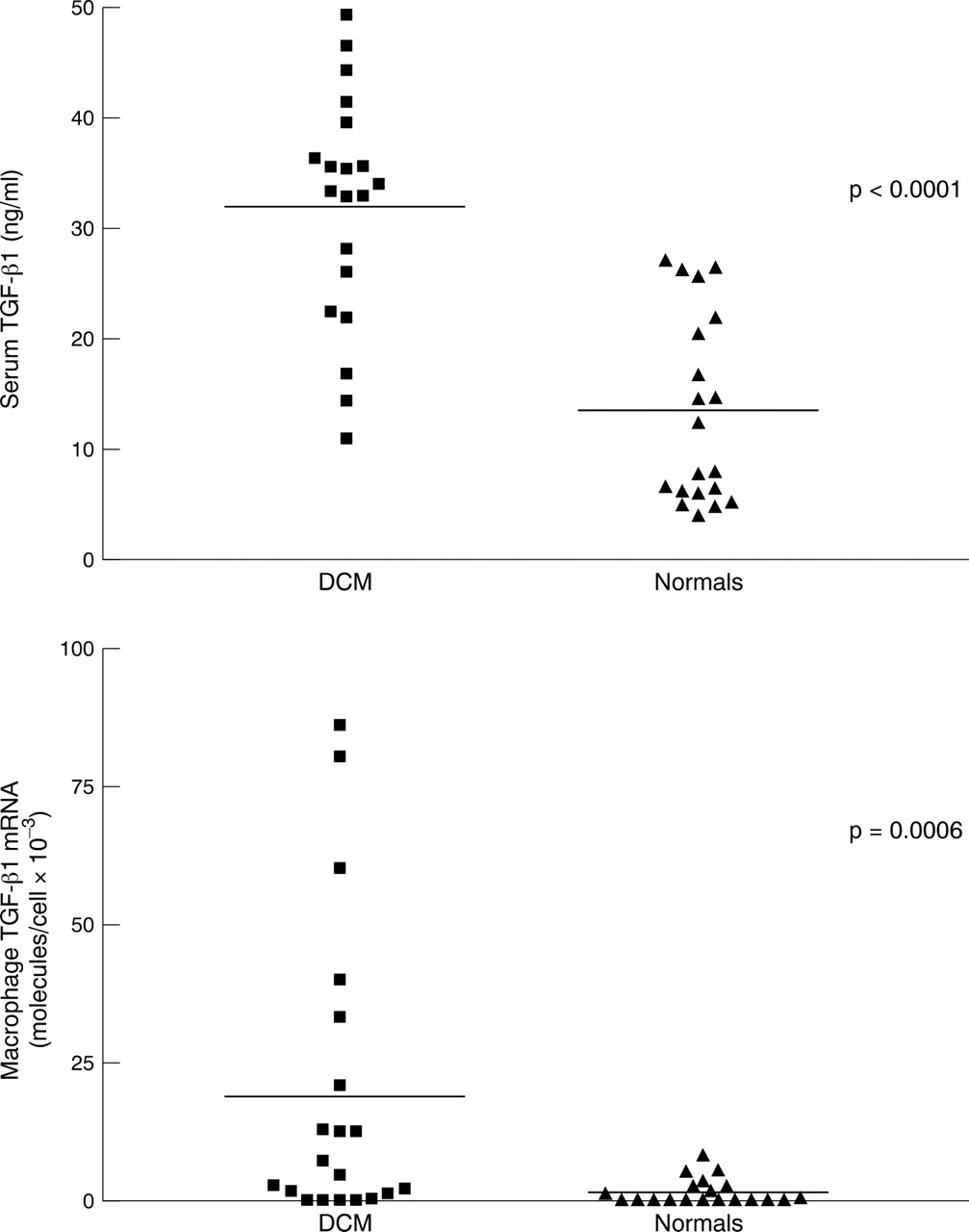
The results showed that serum TGF-β1 concentrations were higher in the dilated cardiomyopathy group (mean (SE) 28.4 (2.2) ng/ml) compared to normals (14.7 (1.6) ng/ml; p = 0.0001, Mann Whitney test). The individual values are shown in fig 1. There was a significant increase in macrophage TGF-β1 mRNA in dilated cardiomyopathy patients compared to controls (18.9 (6.0)v 1.54 (0.5) × 10−3molecules/cell; p = 0.006). Individual values are also shown in fig1. There was no relation between TGF-β1 mRNA, and ejection fraction (r = 0.027; p = 0.5), clinical course over the previous 6–24 months as assessed by the change in ejection fraction (r = 0.005; p = 0.77), or left ventricular diastolic function (TGF-β1 mRNA expression in those with a restrictive left ventricular filling pattern on echocardiography was the same as those without: 2.02 (0.29) and 2.05 (0.26), respectively).

{kind=link}
Scattergram showing individual values for serum TGF-β1 concentrations (upper) and macrophage mRNA concentrations (lower). DCM, idiopathic dilated cardiomyopathy.
In response to injury or disease, the production of TGF-β1 increases cell proliferation and ECM production is stimulated to repair and heal the tissue1. This is achieved through simultaneously stimulating the synthesis of ECM proteins, inhibiting the actions of proteases that degrade ECM, and increasing receptors on cell surfaces. Increased concentrations of TGF-β1 produced by injury, injecting TGF-β1or transferring the TGF-β1 gene invariably leads to tissue fibrosis.
TGF-β1 may be especially important in dilated cardiomyopathy in which there is an overall increase in intramyocardial fibrillar collagen. Recently, Pauschinger presented results in 18 patients with dilated cardiomyopathy suggesting that the gene expression of collagen type III correlated with the gene expression of TGF-β1 in myocardial biopsy specimens, although they did not identify the cell type responsible.5 However, ours is the first published report to demonstrate in patients with idiopathic dilated cardiomyopathy increased macrophage gene expression for TGF-β1 associated with increased circulating concentrations.
It is well documented in patients with idiopathic dilated cardiomyopathy that cytotoxic lymphocytes and macrophages may be present in significant numbers within the myocardium, which is not apparent using light microscopy and requires electron microscopy or immunohistologic techniques.4 Using special immunohistologic staining methods we have found that approximately 40% of myocardial biopsy specimens have increased lymphocytes and macrophages, similar to the published results.4 However, we have not been able to detect any enteroviral genome in right ventricular endomyocardial biopsy specimens from this group of patients (unpublished data). Although macrophages are recognised to be important mediators of cardiac injury, repair, and TGF-β1, there may be other cellular sources for the raised plasma TGF-β1 from within the myocardium, and in situ hybridisation PCR studies are required to define precisely which particular cells are the source.
In summary we have shown, for the first time, increased gene expression for TGF-β1 in macrophages from some patients with idiopathic dilated cardiomyopathy associated with increased plasma concentrations. Probably this reflects the role of macrophages in tissue repair, remodelling and healing. But excessive production of TGF-β1 may account for the increased collagen deposition found in dilated cardiomyopathy, which impairs ventricular compliance and diastolic function, and worsens heart failure.
Acknowledgments
This study was supported by a grant from the University Grants Committee, Hong Kong (no CUHK 292/96M). We thank Ms Skiva Chan RN and Ms Leata Yeung RN for their help.