Article Text

Abstract
Background: Resting left ventricular outflow tract obstruction (LVOTO) occurs in 25% of patients with hypertrophic cardiomyopathy (HCM) and is an important cause of symptoms and disease progression. The prevalence and clinical significance of exercise induced LVOTO in patients with symptomatic non-obstructive HCM is uncertain.
Methods and results: 87 symptomatic patients (43.3 (13.7) years, 67.8% males) with HCM and no previously documented LVOTO (defined as a gradient ⩾30 mm Hg) underwent echocardiography during upright cardiopulmonary exercise testing: 54 patients (62.1%; 95% CI 51.5 to 71.6) developed LVOTO during exercise (latent LVOTO); 33 (37.9%; 95% CI 28.4 to 48.5) had neither resting nor exercise LVOTO (non-obstructive). Patients with latent LVOTO were more likely to have systolic anterior motion of the mitral valve (SAM) at rest (relative risk 2.1, 95% CI 1.2 to 3.8; p = 0.01), and higher peak oxygen consumption (mean difference: 10.3%, 95% CI 2.1 to 18.5; p = 0.02) than patients with non-obstructive HCM. The only independent predictors of Δ gradient during exercise were a history of presyncope/syncope, incomplete/complete SAM at rest and Wigle score (all p<0.05). Subsequent invasive reduction of LVOTO in 10 patients with latent obstruction and drug refractory symptoms resulted in improved functional class and less syncope/presyncope (all p<0.05).
Conclusions: Approximately two-thirds of patients with symptomatic non-obstructive HCM have latent LVOTO. This study suggests that all patients with symptomatic non-obstructive HCM should have exercise stress echocardiography.
Statistics from Altmetric.com
Hypertrophic cardiomyopathy (HCM) is an inherited heart muscle disorder characterised by unexplained left ventricular hypertrophy.1 Approximately 25% of patients have a resting systolic pressure gradient in the left ventricular outflow tract caused by contact between the mitral valve leaflet(s) and the interventricular septum2–6; outflow tract gradients in excess of 30 mm Hg are an important cause of symptoms and an independent predictor of disease progression.7–9
Left ventricular outflow tract obstruction (LVOTO) in HCM is characteristically labile, its magnitude varying spontaneously or following heavy meals and ingestion of alcohol. In some cases, obstruction only appears during a haemodynamic challenge2 10 such as inhalation of amyl nitrite,11 Valsalva manoeuvre12 and infusion of positive inotropes.13 14 However, the clinical significance of outflow tract gradients provoked by such techniques remains controversial as these manoeuvres are difficult to standardise in routine clinical practice and do not reproduce the physiological conditions in which obstruction occurs during daily life.
A recent study by Maron et al suggests that the prevalence of inducible LVOTO in a cohort of patients assessed in a number of referral centres may be as high as 70%.15 However, the clinical significance of this is difficult to interpret as the patients were exercised using different protocols and many patients with severe symptoms or an increased risk of arrhythmia were excluded from the study.
In this study we sought to determine the prevalence of exercise induced obstruction and its relation to symptoms and exercise performance in symptomatic patients with non-obstructive hypertrophic cardiomyopathy using the more physiological stress of upright exercise on a bicycle ergometer.
METHODS
Patients
In all, 135 consecutively reviewed patients (age 43.1 (SD 13.0) years, range 14–73 years, 96 (71.1%) males, and 39 (28.9%) females) with symptomatic non-obstructive HCM were referred for exercise testing. All patients were recruited from a dedicated cardiomyopathy outpatient clinic at The Heart Hospital, University College London and St George’s Hospital Medical School, London, between January 2001 and November 2004. Following initial evaluation, patients were invited to re-attend for an exercise stress echocardiogram during a separate visit.
Inclusion criteria
In order to be eligible for the study, patients had to fulfil the following criteria:
a hypertrophied and non-dilated left ventricle (maximum left ventricular wall thickness ⩾13 mm) in the absence of other cardiac or systemic causes of left ventricular hypertrophy1
No previous documentation of a left ventricular outflow tract gradient of ⩾30 mm Hg on echocardiography
One or more disease-related symptoms defined as central chest pain precipitated by exercise or moderate to severe exertion, lasting ⩽15 minutes; dyspnoea (graded using the New York Heart Association (NYHA) system16) and a history of presyncope/syncope. A history of palpitations was also recorded.
Exclusion criteria
Patients with valvular heart disease, previous myocardial infarction and a history of systemic hypertension (defined as a blood pressure ⩾140/90 mm Hg on three separate occasions) were excluded. Patients with pacemakers and a history of septal reduction therapy (surgical myectomy or alcohol septal ablation) were also excluded. Patients with any previously documented evidence for resting or provoked LVOTO (that is, left ventricular outflow tract gradient ⩾30 mm Hg) were excluded from the study.
Echocardiography
At the initial screening visit to the outpatient department, Doppler, M mode and two-dimensional echocardiography were performed at rest in the left lateral decubitus position using a General Electric Vivid 7 echocardiograph (GE Healthcare, Waukesha, WI, USA) in accordance with American Society of Echocardiography guidelines.17 Left ventricular cavity dimensions were measured in end-diastole and end-systole from M-mode images obtained from parasternal long-axis views. Fractional shortening (FS) was calculated using the formula: ((left ventricular end-diastolic diameter − left ventricular end-systolic diameter)/left ventricular end diastolic diameter) × 100.
The magnitude and distribution of left ventricular hypertrophy were assessed in the parasternal short-axis view and confirmed from parasternal long-axis and apical views. The ventricle was divided into four regions: anterior septum, posterior septum, lateral wall and posterior walls. Wall thicknesses were measured at the level of the mitral valve and papillary muscles in each of the four segments. Maximal left ventricular wall thickness was defined as the greatest thickness in any segment. Patterns of hypertrophy were defined in accordance with previously published methods.18 A semi-quantitative point score of left ventricular hypertrophy (Wigle score) was calculated as previously described.2 In brief the following parameters are measured: the degree of septal hypertrophy (1–4 points); the extension of hypertrophy up to the basal two-thirds of septum (2 points); apical involvement (total septal involvement) (2 points); and extension of hypertrophy into the lateral wall (2 points). The maximum score is 10.
Left ventricular outflow tract diameter was determined at the onset of systole by measuring the minimal distance between the left side of the interventricular septum and the initial echo of the anterior mitral leaflet in the parasternal long-axis view. Systolic anterior motion (SAM) was defined as incomplete if there was any movement of the mitral valve leaflet(s) towards the ventricular septal endocardium without septal contact or complete when there was contact with the ventricular septal endocardium during systole seen in either M-mode or two-dimensional echocardiographic images.1 2 5 6
Left ventricular outflow tract gradient was measured with continuous-wave Doppler in the apical five-chamber view using the modified Bernoulli equation (4V2) where V = peak systolic velocity. LVOTO was defined as a gradient ⩾30 mm Hg. Mitral regurgitation was graded at rest and at peak exercise as absent, trace, mild, moderate or severe according to the criteria set by the American Society of Echocardiography.19 A significant change in the grade of mitral regurgitation was defined as a resting grade of mitral regurgitation ⩽ mild, increasing to a peak exercise mitral regurgitation of ⩾ moderate. Care was taken to differentiate mitral regurgitant jets from left ventricular outflow tract turbulence using the timing and shape of Doppler signals from the two sources.
Upright exercise testing
Following their initial screening visit, patients underwent an upright exercise test on a separate occasion. All cardiac medications (except amiodarone) were discontinued for at least five half-lives before the exercise study. On the day of the exercise study, left ventricular outflow tract velocities were measured in the supine and in the upright position using continuous wave Doppler from the apical five-chamber and three-chamber views. Patients then went on to perform symptom-limited upright exercise on a bicycle ergometer (SensorMedics ErgoMetrics 800S cycle ergometers, Yorba Linda, CA, USA) using a ramp protocol of 10–15 W/min with respiratory gas sampling (VMax 29 Console, Sensormedics, Yorba Linda, CA, USA). During exercise the ECG was continuously recorded and blood pressure measurements were performed at 3-minute intervals and every 3 minutes into recovery until return to baseline using a cuff sphygmomanometer. Patients cycled at a rate of 60–70 revolutions per minute to the point of exhaustion or symptom limitation. Peak exercise VO2 was defined as the highest VO2 achieved during exercise and was expressed as percentage of the predicted maximal VO2 corrected for age, gender and body size. Peak exercise heart rate was defined as the highest heart rate achieved during maximum exercise and expressed as a percentage of the target heart rate adjusted for age.
During exercise and recovery, left ventricular outflow tract velocities were measured every minute. Latent obstruction was defined as a peak left ventricular outflow tract gradient ⩾30 mm Hg measured during exercise or recovery. The highest gradient measured during exercise or recovery was taken as the peak left ventricular outflow tract gradient. The change in gradient (Δ gradient) was calculated as peak gradient − resting gradient.
Clinical follow-up
Follow-up data were collected at routine clinic visits and from attending physicians or general practitioners. All data were verified by the investigators.
Statistical analysis
Sample size
The prevalence of resting LVOTO has been shown to be approximately 25%. We hypothesised that the prevalence of latent obstruction in a cohort of symptomatic patients without resting obstruction would be at least 15% higher than this. This resulted in a sample size of 97 patients at a α = 0.05 and a 90% power.
Statistical analysis was performed using SPSS (version 12.0) statistical software (SPSS Inc, Chicago, IL, USA). All continuous data are expressed as mean (SD). Continuous variables were compared using the Student t test and non-continuous variables were compared using the χ2 test. The McNemar test was used to assess response to septal reduction therapy after exercise testing. In order to determine independent predictors of Δ gradient, multivariable analysis was performed using a stepwise linear regression analysis. A univariate analysis was performed to assess the relation between Δ gradient and age, gender, symptoms, echocardiographic parameters and exercise parameters listed in tables 1 and 2; only those variables that had a significant association (p<0.05) with Δ gradient in univariate analysis were entered into a forward stepping linear regression algorithm. Statistical significance was defined by p<0.05 (two sided).
RESULTS
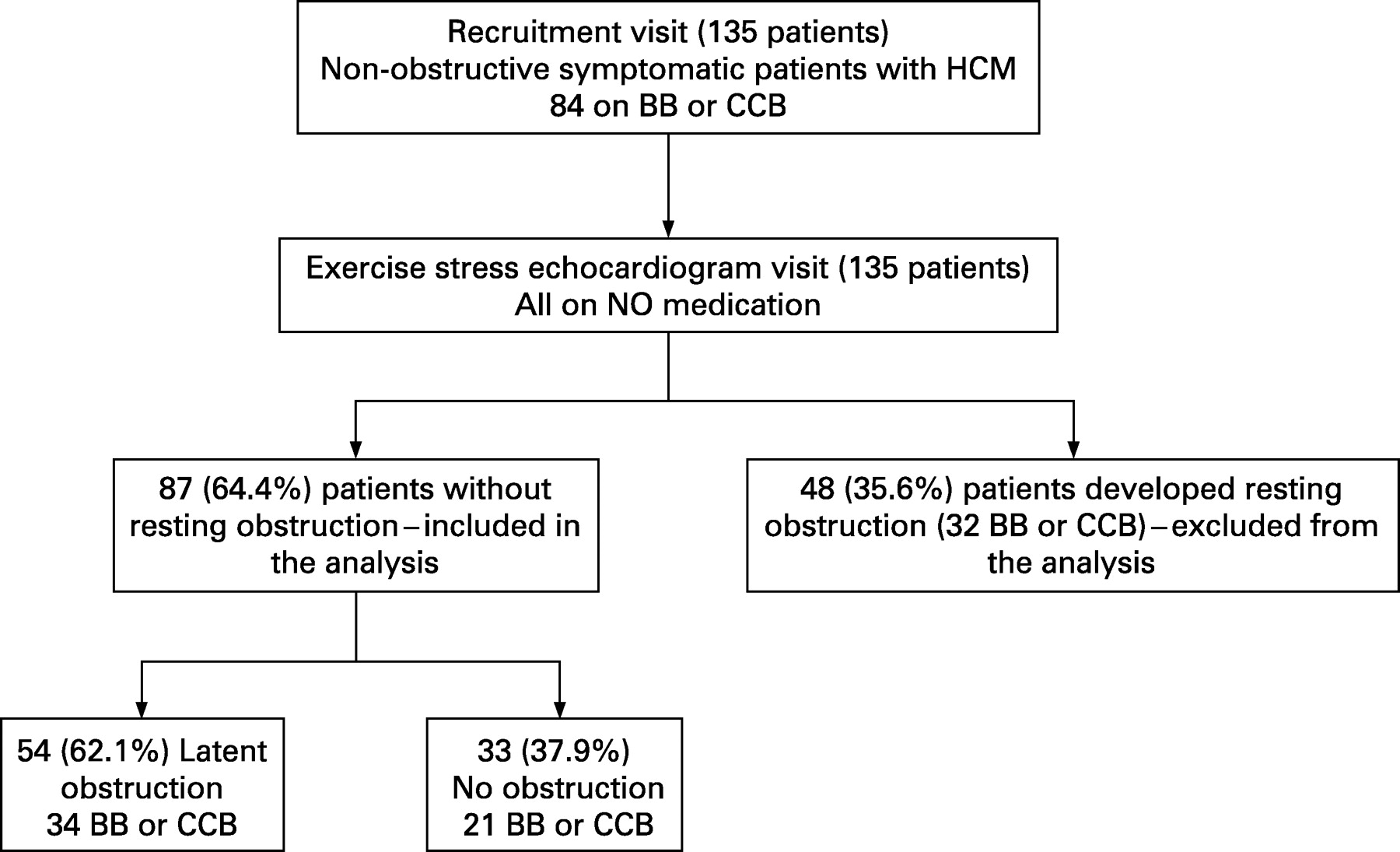
Table 1 shows the baseline clinical data for the initial screening cohort. Fifty-seven (42.2%) of the patients were taking β-blockers, 29 (21.5%) were taking calcium channel blockers (5 patients were taking both a β-blocker and a calcium channel blocker), 18 (13.3%) were taking amiodarone and none was taking disopyramide before exercise testing. On the day of exercise testing (following discontinuation of medical therapy), 44 patients had LVOTO ⩾30 mm Hg on their resting supine echocardiogram; these patients were excluded from the analysis. An additional four patients without resting obstruction in the supine position developed severe symptomatic obstruction (70 mm Hg, 140 mm Hg, 70 mm Hg and 130 mm Hg) in the erect position on the bicycle; these four patients did not exercise and were also excluded from the analysis. All of these patients had evidence of incomplete/complete SAM on their resting echocardiogram. The final study cohort consisted of 87 (64.4%) patients without resting LVOTO (fig 1).

Fifty-four (62.1%; 95% CI 51.5 to 71.6) patients without resting obstruction (seven (13%) of whom were receiving amiodarone) developed obstruction during exercise (latent obstruction); the maximal gradient in nine (16.7%) of these 54 patients was measured 1–3 minutes into the recovery period (mean peak exercise gradient = 20.1 (SD 6.7) mm Hg; range 10–27 mm Hg; mean peak recovery gradient = 39.7 (9.6) mm Hg; 30–58 mm Hg). The mean maximal gradient measured in the latent obstruction cohort was 89.1 (51.2) mm Hg (30–220 mm Hg). Thirty-three (37.9%; 95% CI 28.4 to 48.5; five (15.2%) taking amiodarone) patients had neither resting nor exercise-induced obstruction (mean peak gradient = 15.4 (6.0) mm Hg, 4–27 mm Hg) (non-obstructive).
Table 1 shows the baseline clinical data for the excluded, latent and non-obstructive groups.
Comparisons between latent and non-obstructive groups
There were no differences in the prevalence of exertional chest pain, dyspnoea (NYHA⩾2), presyncope/syncope or palpitations between the non-obstructive and latent obstruction groups. There was a non-significant trend towards more males with latent obstruction compared to females (risk ratio (RR) = 1.9, 95% CI 1.0 to 3.5; p = 0.06). There were no differences in left ventricular wall thickness or cavity dimensions between the two groups. Patients with latent obstruction had smaller left ventricular outflow tract diameters compared to the non-obstructive group (mean difference: 1.5 mm, 95% CI 0.1 to 2.8, p = 0.03) with no difference in the severity of hypertrophy as assessed using the Wigle score (mean difference: 0.5, 95% CI −0.6, p = 0.4). Patients with latent obstruction had a higher prevalence of incomplete or complete SAM on supine echocardiography compared to the non-obstructive group (RR = 2.1, 95% CI 1.2 to 3.8; p = 0.01). The patterns of hypertrophy were similar in both groups. At peak exercise 7/87 (8.1%) patients had a significant increase in mitral regurgitation grade. All of these patients were in the latent obstruction cohort.
Of the patients with latent obstruction, 41 (75.9%) had a peak left ventricular outflow tract gradient of ⩾50 mm Hg. These patients were more likely to be male (RR = 2.7, 95% CI 1.1 to 6.6; p = 0.05) and tended to have a higher prevalence of syncope/presyncope (RR = 1.9, 95% CI 1.1 to 3.3; p = 0.05). There were no other differences in the prevelance of symptoms, echocardiographic or exercise parameters between those patients with a peak left ventricular outflow tract gradient of 30–49 mm Hg and those with a peak left ventricular outflow tract gradient ⩾50 mm Hg.
Table 2 shows the exercise data for patients with and without exercise-induced obstruction. Patients with latent obstruction had a higher percentage predicted peak VO2 compared to those in the non obstructive group (mean difference: 10.3%, 95% CI 2.1 to 18.5, p = 0.02). There were no differences in the peak exercise workload and exercise heart rate achieved or in the respiratory quotient between patients with latent obstruction compared to those with no obstruction (table 2). Patients with latent obstruction had a higher peak exercise systolic blood pressures (mean difference: 15.1 mm Hg, 95% CI 0.7, 29.5, p = 0.04) and a larger Δ blood pressure at peak exercise (mean difference 10.8 mm Hg, 95% CI 0.4 to 21.2, p = 0.04) compared to the non-obstructive group.
Relation between change in outflow gradient, clinical, echocardiographic and exercise data
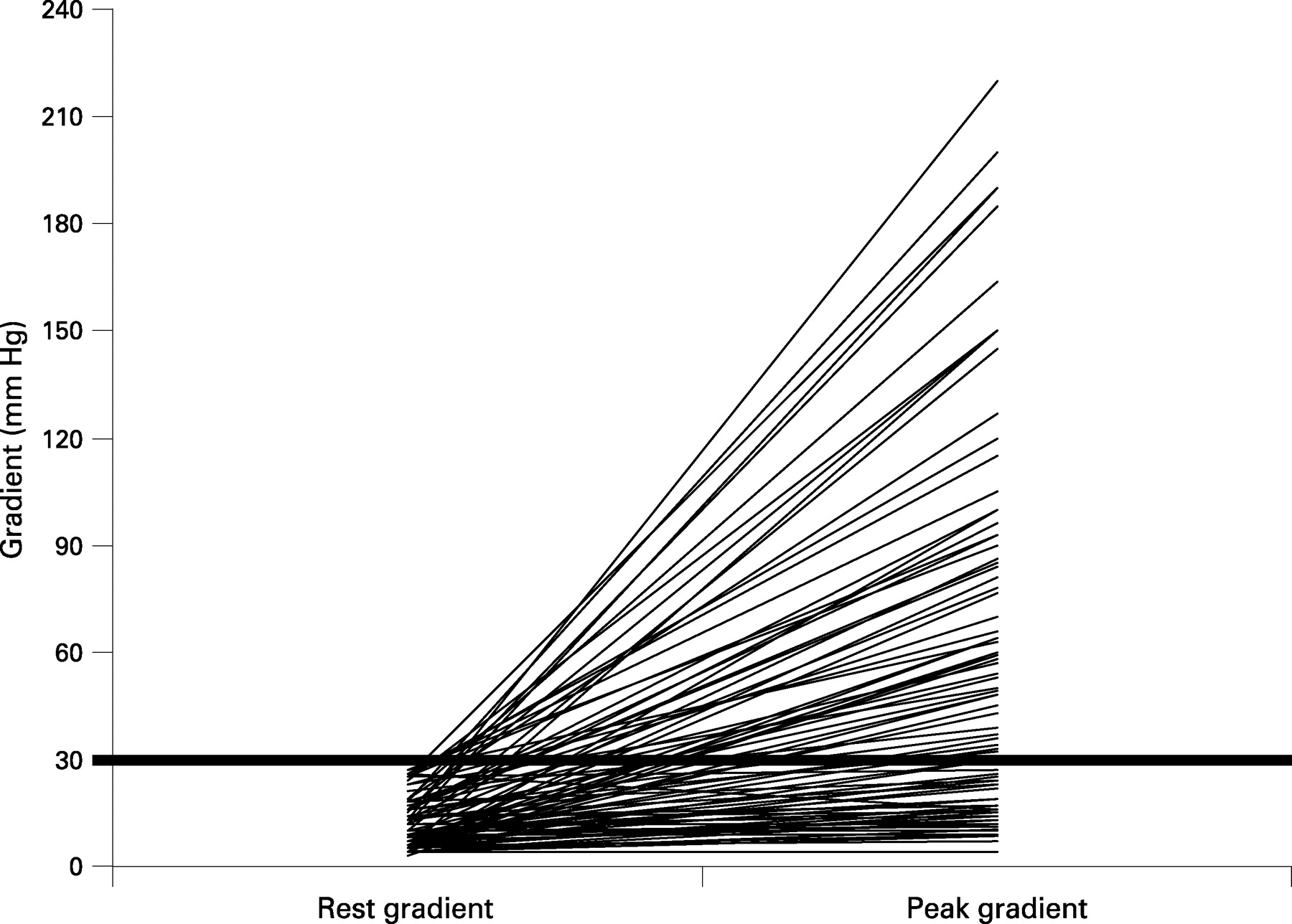
The mean Δ gradient (maximal measured left ventricular outflow tract gradient – resting supine left ventricular outflow tract gradient) for the whole cohort (latent and non-obstructive) was 49.0 (51.2) mm Hg (−10.0–207.0 mm Hg, skewness = 1.2, kurtosis = 1.0). Figure 2 plots the individual data points for left ventricular outflow tract gradients at rest and peak gradient reached. One patient (female, aged 64.0 years with concentric left ventricular hypertrophy and a maximum wall thickness 18 mm) had a fall in gradient. Males tended to have a higher Δ gradient compared to females (22.1 mm Hg, 95% CI 1.0 to 45.1, p = 0.06). There were no differences in Δ gradient in patients with and without dyspnoea, palpitations and exertional chest pain. Patients with a history of presyncope/syncope had a greater Δ gradient compared to those without (mean difference: 33.5 mm Hg, 95% CI 13.0 to 54.0, p = 0.002).
Patients with incomplete or complete SAM on their resting echocardiogram had a greater Δ gradient compared to those without (mean difference: 28.9 mm Hg, 95% CI 6.6 to 51.2, p = 0.01). There was a negative correlation between Δ gradient and Wigle score (r = −0.2, p = 0.03). There was no correlation between Δ gradient and left ventricular outflow tract diameter, maximal left ventricular wall thickness or left ventricular cavity dimensions.
There was a weak correlation between peak exercise VO2 and Δ gradient (r = 0.2, p = 0.04). There were no correlations between Δ gradient and peak exercise systolic blood pressure, Δ blood pressure during exercise and other exercise parameters.
Predictors of change in gradient during exercise
Univariate analysis identified a history of presyncope/syncope, incomplete or complete SAM on the resting echocardiogram, peak exercise VO2 and Wigle score as correlates of Δ gradient (all p<0.05). In a stepwise linear regression analysis model using these variables, only a history of presyncope/syncope, incomplete/complete SAM and Wigle score were independently associated with Δ gradient (β = 29.5, 95% CI 8.7 to 50.2, p = 0.006; β = 25.3, 95% CI 3.7 to 46.9, p = 0.02; β = −4.5, 95% CI −0.1 to −8.8, p = 0.047 respectively; adjusted R2 = 0.2, significance (ANOVA) <0.001).
Clinical follow-up
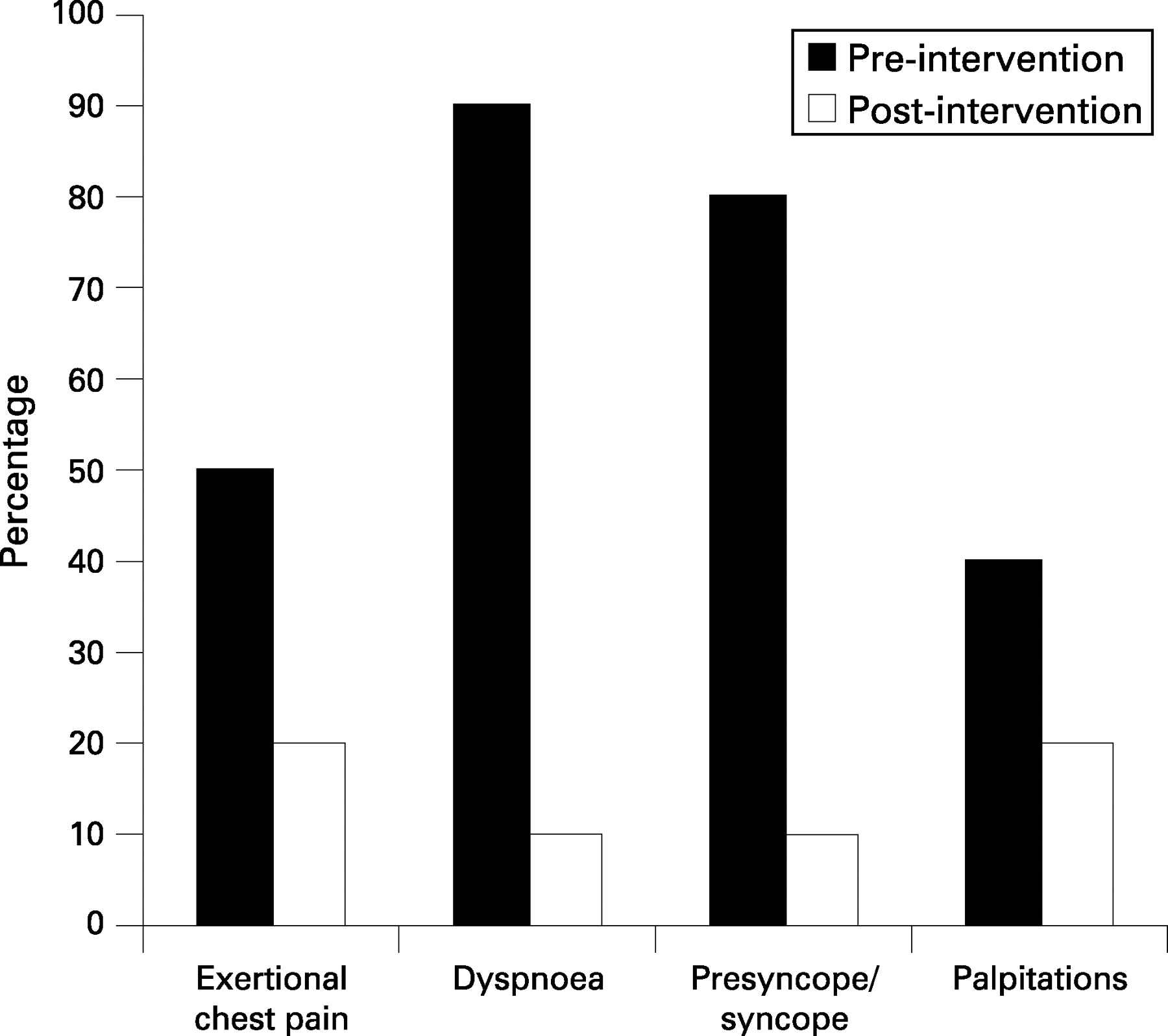
All patients with latent obstruction received treatment with β-blockers, calcium channel blockers or disopyramide. Ten (18.5%) patients (mean age 42.0 (10.1) years (29–62), nine (90.0%) males, mean peak gradient during exercise = 109.4 (40.4) mm Hg) continued to experience severe symptoms in spite of medical treatment. Of these, eight underwent septal myotomy-myectomy (age 37.9 (5.7) years, seven (87.5%) males) and two alcohol septal ablation (age 62 and 55 years; both males). Intervention led to a significant improvement in dyspnoea (p = 0.008) and the frequency of presyncope/syncope (p = 0.02), but no change in palpitations or chest pain at their first follow-up visit after the intervention (fig 3). Nine of the 10 (90%) patients who went on to have septal reduction therapy had a repeat metabolic exercise test (mean 1.0 (0.8) year after septal reduction therapy, range 0.4–2.9 years). There was no difference in the percentage predicted peak VO2 measured before and after their therapy for septal reduction (mean difference = −4.3 (13.4), 95% CI −14.5 to 6.0, p = 0.4). There was no relation between the change in symptoms and the change in percentage predicted peak VO2 measured pre-septal and post-septal reduction therapy.
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
This study demonstrates that up to two-thirds of symptomatic patients with non-obstructive HCM develop obstruction during upright exercise, confirming the findings in a recent study by Maron et al, despite the fact that patients in their study exercised in three different centres using different methodologies.15 The important new findings are that patients with exercise induced obstruction tend to have higher peak oxygen consumption than patients with non-obstructive HCM and the magnitude of gradient change during exercise correlates with a history of syncope/presyncope. These findings have major implications for the evaluation and treatment of patients with HCM, and pose important questions about the relation between LVOTO and cardiac performance.
Mechanisms of obstruction
Previous studies have shown that 25–30% of patients with HCM have a resting pressure gradient across the left ventricular outflow tract caused by systolic anterior motion of the mitral valve leaflets.4–6 The most widely accepted explanation for this phenomenon is that septal hypertrophy and narrowing of the left ventricular outflow tract result in a high velocity zone anterior to the mitral valve that causes its tip to be sucked against the septum by the Venturi effect.2 4–6 However, this hypothesis does not explain a number of features associated with SAM; specifically, the onset of SAM before aortic valve opening; the presence of SAM in patients with primary mitral valve abnormalities and little or no septal hypertrophy; and the predominance of SAM at the centre of the anterior mitral valve leaflet.20 Experimental and observational data suggest that anterior displacement of the papillary muscles and sub-mitral apparatus are necessary to create sufficient leaflet slack to allow anterior movement of the mitral leaflet.21 The effect of enhancing contractility in this model is to increase the drag forces on the mitral leaflet, thereby driving rather than sucking it into the septum.
Labile and latent obstruction
It is well recognised that some patients without outflow obstruction at rest have gradients that can be provoked by physiological and pharmacological interventions that diminish left ventricular end-diastolic volume or augment left ventricular contractility.10 The term labile obstruction has been used to describe the spontaneous appearance and disappearance of obstruction and latent obstruction to describe gradients that only appear with provocation.2 The most commonly used techniques used to provoke obstruction have been inhalation of amyl nitrate,11 the Valsalva manoeuvre12 and intravenous inotropes.13 14 The problem with all such methods is that, unlike upright exercise stress testing, they do not reliably reproduce the physiological circumstances in which latent obstruction is likely to occur1 22; consequently, gradients produced during such manoeuvres correlate poorly with gradients induced during exercise.23
Clinical significance of LVOTO
Although there were no significant differences in the frequency of angina, dyspnoea and syncope in patients with and without obstruction, there was a relation between the change in gradient during exercise and presyncope/syncope, suggesting that large inducible gradients are an important cause of symptoms in HCM. Unexpectedly, lower Wigle scores were independently associated with the changes in left ventricular outflow tract gradient during exercise, suggesting that altered left ventricular geometry and not septal thickness per se is a major determinant of outflow tract obstruction.
The relation between inducible obstruction and peak oxygen consumption was also counterintuitive. Although there was only a weak relation between the change in exercise gradient and peak exercise VO2, peak oxygen consumption was higher in patients with latent obstruction compared to those in the non-obstructive group. This was not explained by more vigorous exercise in the latent cohort as work-rates were similar to those patients with non-obstructive HCM. A more likely explanation for the higher peak VO2 is that, in comparison with patients who have no obstruction, those with latent obstruction have a higher cardiac output at peak exercise (perhaps reflecting more severe diastolic dysfunction in the non-obstructive cohort).12 23 24 This hypothesis is supported by the higher peak exercise blood pressure in the latent obstruction group. One might conclude from this observation that provoked gradients are of little clinical significance, but subsequent invasive management of outflow obstruction in a subset of individuals with large exercise induced gradients markedly improved their symptoms. The major clinical implication of these findings is that peak oxygen consumption alone may not be a useful guide to the requirement for (or success of) interventions that reduce outflow tract obstruction. Further studies are required to prospectively evaluate the short-term and long-term effects of intervention in patients with provocable obstruction.
Limitations
This study is limited by the fact that only symptomatic patients were recruited into the study and the prevalence of latent obstruction in an asymptomatic cohort remains unknown. However, the symptomatic cohort of patients represents a significant clinical challenge and this study suggests that actively investigating patients with symptomatic non-obstructive HCM for latent obstruction is of clinical utility.
The power calculations suggested that the number of patients needed for the study was 97. We expected that a proportion of the recruited patients would have labile obstruction (that is, developing without provocation); however, this was much higher than we expected. Despite this, the differences in prevalence between resting obstruction (25% of patients with hypertrophic cardiomyopathy) and latent obstruction (62.2%) in 87 patients using an α = 0.05 powered the study at 0.99.
CONCLUSIONS
Over 60% of symptomatic patients with apparently non-obstructive hypertrophic cardiomyopathy have obstruction during exercise. A history of presyncope/syncope and the presence of SAM are associated with the greatest changes in exercise-induced gradients. The identification of latent obstruction as a cause of exertional symptoms should prompt more vigorous pharmacological therapy, using combinations of drugs (including disopyramide) that would not be routinely employed in patients with non-obstructive HCM. The use of invasive gradient reduction strategies (alcohol septal ablation and surgical myectomy) in patients with large exercise-induced gradients refractory to medical therapy can substantially improve symptom status, but require further study in prospectively evaluated cohorts. The paradoxical relation between peak oxygen consumption and exercise-induced obstruction is intriguing and warrants further investigation.
REFERENCES
Footnotes
Competing interests: None.