Article Text

Abstract
Background: In recent large paediatric cardiomyopathy population studies from North America and Australia, vitamin D deficiency was not identified as a cause of infant heart failure. However, rickets is resurgent in developed countries.
Objective: To review the prevalence of this cardiomyopathy in paediatric cardiology units of southeast England and determine the prognosis.
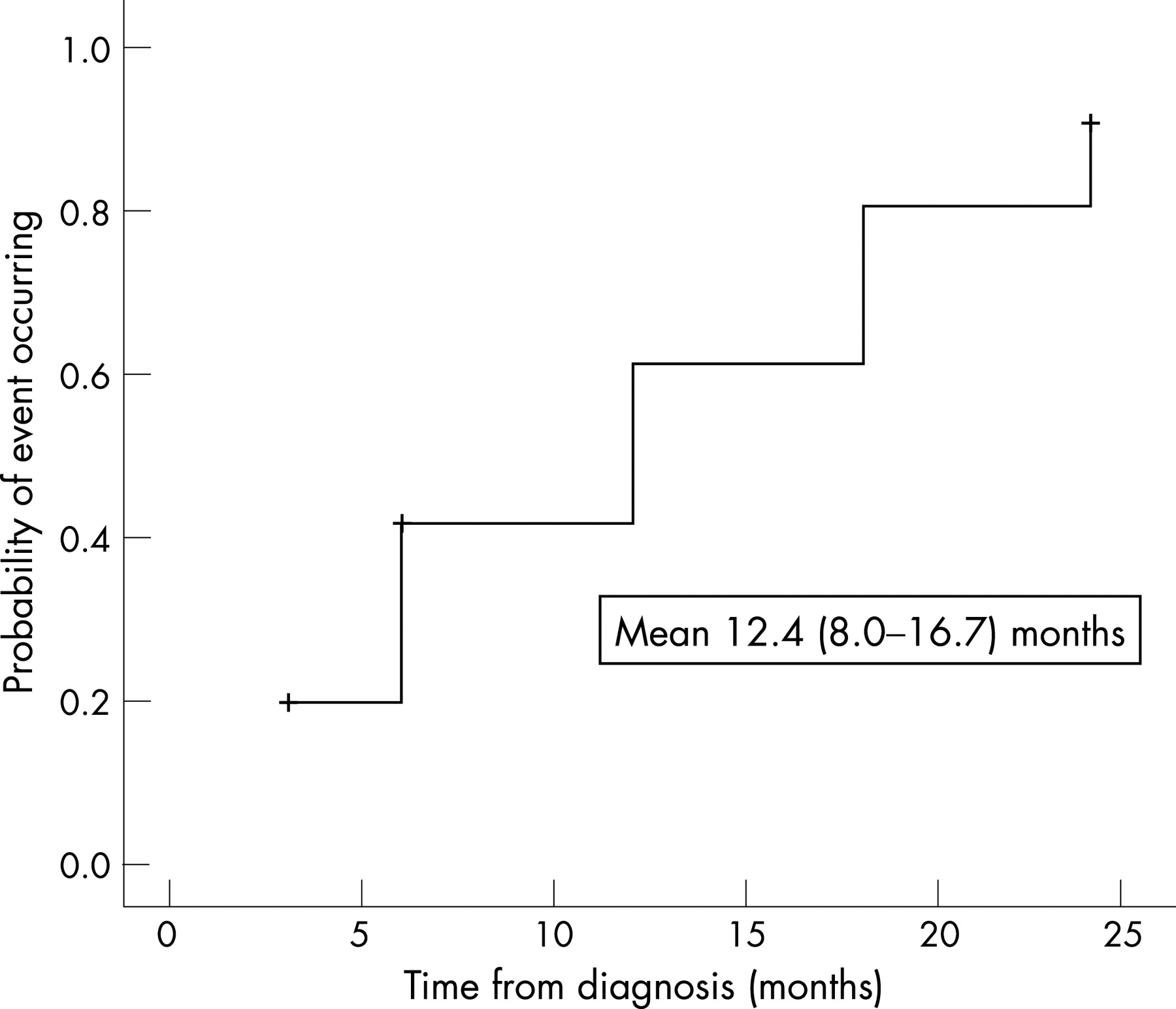
Methods and results: A retrospective review from 2000 to 2006 in southeast England. Sixteen infants (6 Indian subcontinent, 10 black ethnicity) were identified: median (range) age at presentation was 5.3 months (3 weeks–8 months). All had been breast fed. Ten presented at the end of the British winter (February–May). Median shortening fraction was 10% (range 5–18%) and median left ventricular end diastolic dimension z score was 4.1 (range 3.1–7.0). Six had a cardiac arrest; three infants died. Eight were ventilated, two required mechanical circulatory support and 12 required intravenous inotropic support. Two were referred for cardiac transplantation. Median (range) of biochemical values on admission was: total calcium 1.5 (1.07–1.74) mmol/l; alkaline phosphatase 646 (340–1057) IU/l; 25-hydroxyvitamin D 18.5 (0–46) nmol/l (normal range >35) and parathyroid hormone 34.3 (8.9–102) pmol/l (normal range <6.1). The clinical markers and echocardiographic indices of all survivors have improved. The mean time from diagnosis to achieve normal fractional shortening was 12.4 months.
Conclusions: Vitamin D deficiency and consequent hypocalcaemia are seen in association with severe and life-threatening infant heart failure. That no infant or mother was receiving the recommended vitamin supplementation highlights the need for adequate provision of vitamin D to ethnic minority populations.
Statistics from Altmetric.com
Rickets has been recognised in England for over 350 years.1 As the cause became better understood it virtually disappeared in developed countries. Unfortunately, there have been reports of a resurgence of nutritional rickets in ethnic minority populations in Europe2–8 and North America.9–15 A few case reports of cardiomyopathy associated with rickets have been published.16–19 The first reported case of rickets cardiomyopathy in the United States was published in 2003 as an “unusual cause of paediatric cardiomyopathy”.19 Recently, extensive population studies have been published with over 1500 cases of paediatric dilated cardiomyopathy reported, but no cases of vitamin D deficiency were identified.20–22 The recognition of this diagnosis in a number of infants in cardiac intensive care units in London prompted our study. We report the presentation, and clinical outcome in the first substantial case series of this problem.
PATIENTS AND METHODS
We reviewed the records of all known patients who presented with dilated cardiomyopathy associated with vitamin D deficiency between January 2000 and December 2006 to four cardiology referral centres—Great Ormond Street Hospital, Royal Brompton Hospital, Guy’s and St Thomas’ Hospital, all in London, and John Radcliffe Hospital, Oxford. These centres receive all paediatric cardiology referrals from southeast England, a metropolitan area with a total population of about 18 million. Sixteen infants were identified. The median (range) of age at presentation was 5.3 months (3 weeks to 8 months). All were initially transferred from their local hospital. Patients were investigated according to the local cardiomyopathy protocol, which meant that there was some variation in laboratory evaluation. Barth syndrome was not specifically looked for, but no infant had neutropenia and six were female. Available demographic information, including age, gender and racial/ethnic background, was identified and details of presentation, feeding habits, maternal supplementation and clinical signs were collected.
Calcium, ionised calcium, inorganic phosphate and alkaline phosphatase were measured by standard automated techniques. Vitamin D (as 25-hydroxyvitamin D (25-OHD)) was measured by radioimmunoassay. Parathyroid hormone (PTH) was measured using a two-site assay that measures “intact” hormone.
Only infants admitted as emergency inpatients to high-dependency or intensive care units were included. Low cardiac output heart failure was defined as hypotension, poor perfusion and breathlessness. Dilated cardiomyopathy was defined as a left ventricular end diastolic dimension of over 2 z values with impaired systolic function. Because this was a retrospective study using only data that had been collected for clinical purposes, prospective ethical committee approval was not sought.
RESULTS
All infants had clinical heart failure, most requiring ventilatory and inotropic support (table 1).
Six infants were resuscitated from an episode of cardiopulmonary arrest within 24 hours of admission. Another infant could not be resuscitated and died. Extracorporeal membrane oxygenation support for low cardiac output was needed in two cases for 7 and 13 days. One of the children mechanically supported had neurological damage and ventilatory support was withdrawn 6 weeks after presentation. Two infants were assessed for cardiac transplantation, one of whom was listed for transplant, but was withdrawn from the transplant waiting list because of clinical improvement. There was one late sudden death 8 months after presentation in an infant who had improved clinically, although echocardiographic parameters remained abnormal.
Electrocardiograms showed sinus rhythm in all and there was no evidence of QTc prolongation. Echocardiograms showed very dilated left ventricles in each case, with accompanying poor systolic function (table 2).
All of the infants belonged to dark-skinned ethnic minority groups. Most (10/16) presented at the end of the British winter. Twelve of them were exclusively breast fed; four others were initially breast fed and were being weaned onto solids. None of the infants or mothers had received vitamin D or calcium supplementation prenatally or postnatally.
Table 2 presents the biochemical values. All infants were profoundly hypocalcaemic. Alkaline phosphatase was raised in all except one. The PTH level was raised in all patients. 25-OHD levels were available in 14 patients before the start of treatment. Vitamin D levels probably need to be >50 nmol/l in order to maintain physiological suppression of PTH,23 but a level lower than about 35 nmol/l marks the point at which vitamin D deficiency usually becomes manifest. In our cases the median level of vitamin D was <20 nmol/l, but we have included one case aged 3 weeks at presentation who had a level of 43 nmol/l. However, in all cases PTH values were uniformly raised and initial calcium/ionised calcium uniformly low.
Ten patients had radiological evidence of rickets. Maternal biochemistry was available for all of them, and all mothers had normal calcium, phosphate and alkaline phosphatase levels. Unfortunately PTH and 25-OHD levels were measured in only five of them as the local laboratories did not consider these investigations to be indicated in the other mothers in view of their normal biochemistry. Of these five women, three had raised PTH and low 25-OHD levels and the remaining two had normal values. Once vitamin D deficiency was diagnosed or suspected, replacement therapy was started. Nine infants received cholecalciferol, three had ergocalciferol and the rest alfacalcidol. All received calcium supplements. Appropriate dietary advice was given to parents. Mothers found to have vitamin D deficiency or who decided to continue breast feeding also received vitamin D and calcium supplements. Calcium supplements in the infants were generally stopped at 2–3 months, but vitamin D supplements were continued for at least 6 months. All had normal calcium levels after 1 month of treatment.
A postmortem examination was performed in one of the infants who died. There was a large pericardial effusion. The heart was enlarged and weighed 62 g (expected weight 34 g). The left ventricle was dilated and showed concentric hypertrophy with mild fibrous thickening of the endocardium The myocardial fibres were hypertrophied without disarray (fig 1). Their nuclei were enlarged and hyperchromatic and many myofibres were stretched and thinned. There was a mild increase in interstitial fibrous tissue, particularly in the subendocardial regions. The endocardium was thickened by fibroelastic tissue. The vessels were normal. There was no inflammatory cell infiltrate and apoptosis was not evident in the myocytes. The costochondral junctions were swollen and ovoid.

Surviving infants were reviewed regularly. Figure 2 shows a Kaplan–Meier curve demonstrating the return to normal fractional shortening using data from echocardiography reviews at 6-monthly intervals. Recovery of left ventricular fractional shortening to the normal range occurred at a mean of 12.4 months from presentation.
{kind=link}
{kind=link}
DISCUSSION
Recently, large population studies of paediatric cardiomyopathy have been published. In one paper 1426 cases of dilated cardiomyopathy were described, the largest series ever reported.20 A population-based study of 184 cases from Australia was also recently published.21 In a further report the aetiology of over 900 cases of paediatric cardiomyopathy was recorded.22 However, in these large series, no cases were attributed to vitamin D deficiency. The incidence of heart failure (excluding those cases associated with congenital heart disease) in infants and children in the UK and Ireland has recently been shown to be 106 cases a year. About 40% of these were infants (data presented at the 4th World Congress of Paediatric Cardiology, Argentina, 2005). This report of 16 cases of rickets-associated heart failure in infants seen over a period of 6 years (2.7 a year) in the southeast of England alone, suggests that many cases of infant heart failure may be linked to rickets in the UK in the present era. It should be emphasised that the infants in this series had overt and severe clinical heart failure, and it seems very likely that many infants from these ethnic groups would have had undetected subclinical, but potentially important, cardiac abnormality during the same era.
All the infants we have reported on were from dark-skinned ethnic minorities, were breast fed and 10/16 presented at the end of the British winter (February–May). Lack of sunlight exposure is important, as the main source of vitamin D is from ultraviolet radiation of the skin; there is no radiation of the appropriate wavelength (290–310 nm) in Britain from the end of October to the end of March.6 Darker-skinned people require more exposure to sunlight than lighter-skinned people to manufacture vitamin D.6 23 Measurement of vitamin D concentration in the non-pregnant adult population in Birmingham, UK showed that in winter 85% of Asian people, compared with 3.3% of non-Asian subjects, had a vitamin D concentration of <8 ng/ml.6 In the infants we have reported on, breast feeding is also likely to have been an important factor as little vitamin D is present in breast milk. Fetal levels may be maintained by initial passage of 25-OHD across the placenta, provided that the maternal vitamin D status is adequate.
Possibly, the finding of vitamin D deficiency was coincidental and the infants we have presented may have had cardiomyopathy from other causes. However, all infants were profoundly hypocalcaemic, PTH values were uniformly raised and initial calcium/ionised calcium levels uniformly low. Calcium levels are checked routinely in children admitted with heart failure, yet hypocalcaemia was not a feature of the large series of paediatric cardiomyopathies.20–22 None of the centres in our study saw any cases of hypocalcaemia and cardiomyopathy in white infants during the study period, although cardiomyopathy with normal calcium was seen in this latter group. Cases of cardiomyopathy were also seen in dark-skinned infants who did not have hypocalcaemia during this period. Only infants with hypocalcaemia were investigated and the PTH level determined; if this was abnormal the vitamin D level was also obtained. All infants with hypocalcaemia and cardiomyopathy during this period are included in this report. In adults, hypocalcaemia alone is sufficient to induce dilated cardiomyopathy.24–28 Children have also been reported to develop heart failure in hypoparathyroidism.29 Treatment with antifailure drugs and calcium alone was sufficient to enable recovery.30 31 Recovery was not always rapid in these cases, which is consistent with the slow improvement period in our patients. Slow recovery of function in infants with severe heart failure from myocarditis is also well known.32
The severity of the heart failure associated with vitamin D deficiency in the infants we have described is surprising and, as far as we know, has not been documented previously. Nevertheless, the outcome is good in survivors. The time course of recovery we have documented may be of help to physicians and families of infants with this problem and would suggest cardiac transplantation is rarely needed for this diagnosis. It is of concern that none of the mothers or infants were receiving the recommended vitamin D supplementation.
CONCLUSIONS
We have reported the first case series of infants with cardiomyopathy seen in association with vitamin D deficiency and hypocalcaemia. This series highlights inadequacies in the provision of vitamin D supplementation to the ethnic minority community in the UK.
REFERENCES
Footnotes
-
Funding: This study was not funded externally.
-
Competing interests: None.