Article Text

Abstract
Background: Diastolic dysfunction (DD) is highly prevalent and associated with increased morbidity and mortality, but its natural history remains poorly defined.
Objective: This cohort study sought to characterise the influence of clinical features, medical therapy and echocardiographic parameters on the progression of DD.
Methods: We identified 926 consecutive patients (aged 62 (14) years, 221 women) with DD and preserved systolic function. A repeat echocardiogram was performed in 199 patients ⩾1 year after the baseline study (average 3.6 (1.4) years). Follow-up for 4.8 (2.5) years was 97% complete for the major endpoint of all-cause mortality. Cox regression analyses were performed to identify the associations of mortality.
Results: Over follow-up, 142 patients died and 22 were admitted with heart failure. The independent predictors of death were age, hyperlipidaemia, co-morbid disease and restrictive filling. The degree of diastolic dysfunction remained stable in 52%, deteriorated in 27% and improved in 21%. There was a greater use of medical therapy in those with stable or worsening diastolic function; when the protective effects of these agents were taken into account in a multivariate model, improvement in diastolic dysfunction was associated with a survival benefit.
Conclusion: DD is associated with all-cause mortality, independent of the presence of a major co-morbidity. The degree of DD remains stable in about 50% of patients, the population whose diastolic function improves over time has a more favourable outcome.
Statistics from Altmetric.com
Diastolic dysfunction (DD) is a commonly recognised echocardiographic finding, irrespective of the presence or absence of clinical features of heart failure.1 2 Although this abnormality may be identified regardless of the level of systolic function, it is commonly of interest in the presence of normal or near-normal systolic function. The prevalence of this problem increases with age3-6 and is also associated with hypertension, coronary artery disease (CAD), obesity, diabetes and systolic dysfunction.3 6 7 DD is believed to be at least part of the pathophysiological cause of diastolic heart failure8–10—a condition associated with significant morbidity and mortality.7 9 11–14
Three classes of DD are identified on the basis of transmitral inflow patterns. Delayed relaxation (class 1) is common with increasing age, may be associated with disturbed left ventricular (LV) loading and is associated with adverse outcome.3 15 Pseudonormal filling (class 2) and restrictive filling (class 3) are characterised by evidence of raised left atrial (LA) pressure3 16–18 and have a worse prognosis. These “stages” of diastolic dysfunction suggest that there is a passage from one stage to the next and indeed this seems plausible based on the described physiology of increasing LA pressure and decreasing LV compliance. However, the evolution of DD and its association with outcome have not been observed. In this study, we sought to determine the natural history and stability of DD using serial echocardiograms, and to determine the clinical outcomes of DD with the primary endpoint of all-cause mortality.
METHODS
Study design
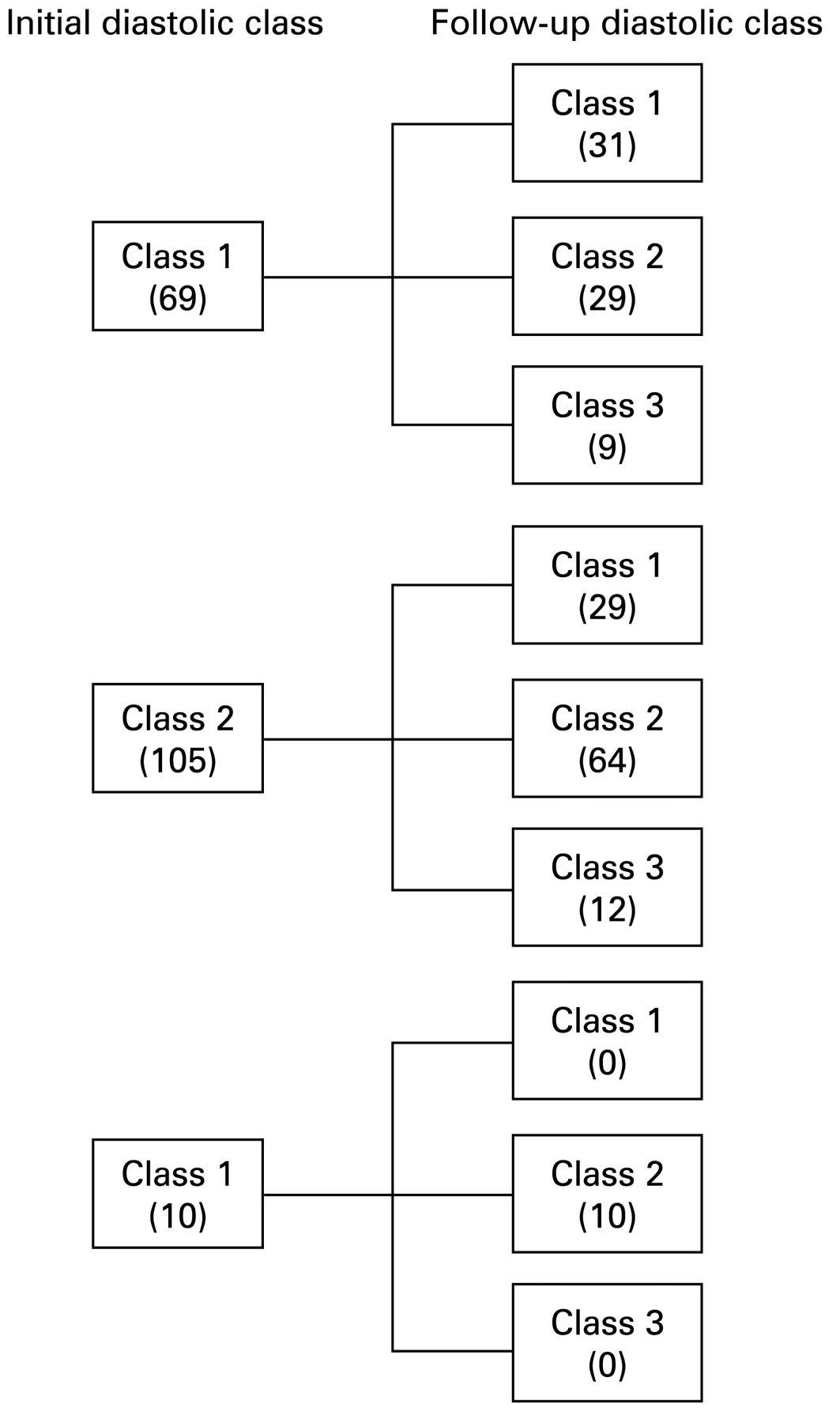
We performed a cohort study derived from a consecutive group of 926 patients (62 (14) years, 221 women) undergoing echocardiograms in the years 2000 and 2001 showing DD with preserved systolic function (ejection fraction (EF) ⩾45%). Patients who had a history of valvular surgery or heart transplant were excluded. Patients were followed over 4.8 (2.5) years for death and hospital admissions, and a follow-up scan was performed in a subgroup of 199 patients after 3.6 (1.4) years (fig 1).

Progression of diastolic class in patients undergoing follow-up echocardiography.
Clinical evaluation
Baseline data were collected regarding body-mass index (BMI), hypertension (HTN; blood pressure ⩾140/90 mm Hg or on treatment); hyperlipidaemia (total cholesterol >6 mmol/l and/or LDL >4 mmol/l or on treatment); diabetes mellitus (random blood sugar level (BSL) >11.1 mmol/l, fasting BSL >7.0 mmol/l or on treatment), family history of premature coronary heart disease (CHD) (onset <60 years old), current or previous smoking or a history of CHD. The presence of serious co-morbidities (organ failure or terminal malignancy) was noted. The clinical diagnosis of heart failure was determined using Framingham criteria. End-stage kidney disease was defined as class V or dialysis-dependent kidney disease. Respiratory failure was determined as type I or II respiratory failure or supplemental-oxygen dependency. Liver failure was defined as the presence of liver disease with clinical evidence of decompensation. Terminal malignancy was defined as a serious malignancy (with or without the presence of metastases) that was not amenable to curative treatment and/or treatment with palliative intent.
Echocardiography
Echocardiograms were obtained using a standard protocol and using standard commercial equipment. LA size was measured by planimetry in the apical four-chamber view. Transmitral flow was measured using pulsed-wave Doppler at the leaflet tips, aligned with the direction of LV filling.17 Diastolic dysfunction was diagnosed on the basis of increased LA size in the absence of atrial fibrillation (AF) and mitral valve disease, with and without abnormal transmitral flow.
Of the 926 patients identified, 191 were excluded for technical reasons. Two patients had concurrent disease that could influence the assessment of diastolic function (LA mass, pericardial effusion). Seventy-nine patients had incomplete clinical data (missing or incomplete chart information). The remaining 110 patients were excluded as the E or A ratio or deceleration time could not be measured because of merging of the passive (E) and active (A) filling waves, poor imaging or other technical difficulties with the scan. In the remaining 735 patients, the class of diastolic dysfunction was determined using the age-predicted normal range for E wave deceleration time19 as: class Ib, delayed relaxation in the presence of LA enlargement; class II, pseudonormal filling (normal deceleration time for age in the presence of LA enlargement); and class III, restrictive filling (short deceleration time).
Follow-up
In a subgroup of 199 patients, a follow-up echocardiogram was performed at least 1 year after the initial scan (mean 3.6 (1.4) years). Of these, 15 patients were excluded on the basis of AF on the repeat echocardiogram (fig 1). Follow-up data were sought for blood pressures (obtained at outpatient visits or during hospitalisation), and correlated with changes in diastolic function. Medications were sought at the time of each echocardiogram. In order to compare doses of different agents, these were expressed as the percentage of recommended dose for each, and analysed by class. The diastolic class was assessed on the follow-up echocardiogram, which enabled the assessment of the change in diastolic class over time. Three groups were identified as improved, stable and deteriorated diastolic function.
Patients were followed for mortality over 4.8 (2.5) years, based on clinic attendance, chart review and standardised telephone call. The primary clinical endpoint was all-cause mortality.
Statistical analysis
An initial statistical comparison was made between the total patient population and the group lost to follow-up to determine if baseline characteristics were similar between the two populations. χ2 Tests were performed on categorical variables and t tests or ANOVA on continuous variables. Cox regression analyses were performed to determine the univariate associations of death. The factors examined were characteristics of the patient population, cardiovascular risk factors, medications and echocardiographic parameters. Multivariate Cox models were generated to examine the independent predictors of mortality. We also sought to determine whether the stability of diastolic function over time correlated with mortality.
RESULTS
Baseline characteristics
The clinical status of patients at baseline is summarised in table 1. Most patients were male, had cardiac risk factors, were taking inhibitors of the renin-aldosterone axis and over one-third had CAD. Table 1 also lists the indications for echocardiography; most tests were performed for the assessment of LV function. Most of the studies demonstrated diastolic dysfunction without other abnormalities.
Clinical follow-up
Follow-up information was obtained in 716 patients (97%). Patients lost to follow-up had a higher prevalence of obesity, and a lower usage of nitrates, vasodilators and drugs acting against the renin-angiotensin-aldosterone axis (table 1). However, the indications and findings on echocardiography did not differ between groups (table 1). In the course of follow-up, there were 142 deaths.
Correlates of events
The independent correlates of mortality were age (β = 1.04; 95% CI 1.03 to 1.06; p<0.001), hyperlipidaemia (β = 0.56; 95% CI 0.37 to 0.83; p = 0.004), co-morbid disease (β = 10.06; 95% CI 6.76 to 14.97; p<0.001) and restrictive filling (β = 2.11; 95% CI 1.00 to 4.42; p = 0.05). Other univariate associations of death that were not independent included baseline heart failure, increased body mass index) and baseline diuretic therapy.
Progression of diastolic dysfunction
Follow-up echocardiograms were performed in sinus rhythm and at least 1 year after the initial echocardiogram in 184 patients. Figure 1 illustrates the progression of diastolic class. Overall, this remained stable in 95 patients (52%). Of the 50 patients (27%) showing deterioration, 29 deteriorated from delayed relaxation to pseudonormal filling and nine to restrictive filling, and 12 changed from pseudonormal to restrictive filling. Of the 39 with improved function, 29 changed from pseudonormal to delayed relaxation and 10 from restrictive filling to pseudonormal. Analysis of variance demonstrated a significant association between worsening diastolic class and worsening EF (p = 0.03), with a reduction of EF in the patients who showed a deterioration in diastolic class (−8% (13%)), a minor change in those with stable diastolic class (−1% (9%)) and no change (0% (7%)) in those whose diastolic class improved.
In the subgroup of 67 patients with three or more echocardiograms performed during the study period, while the degree of diastolic dysfunction fluctuated over time, most patients showed a trend in the evolution of their DD. Twenty-two of these patients (33%) had variable diastolic function with 77% of these fluctuating between two diastolic classes. The remaining 45 patients with three or more studies showed a linear trend in their diastolic function—13 (19%) patients improved, 19 (28%) patients remained stable and 13 (19%) patients deteriorated. Of the patients whose DD improved, 69% showed improvement early during the follow up period (within 2 years). However, deterioration in diastolic function occurred later in the study period (62% deteriorating after 4 years of follow-up).
Clinical correlates of alteration of diastolic function
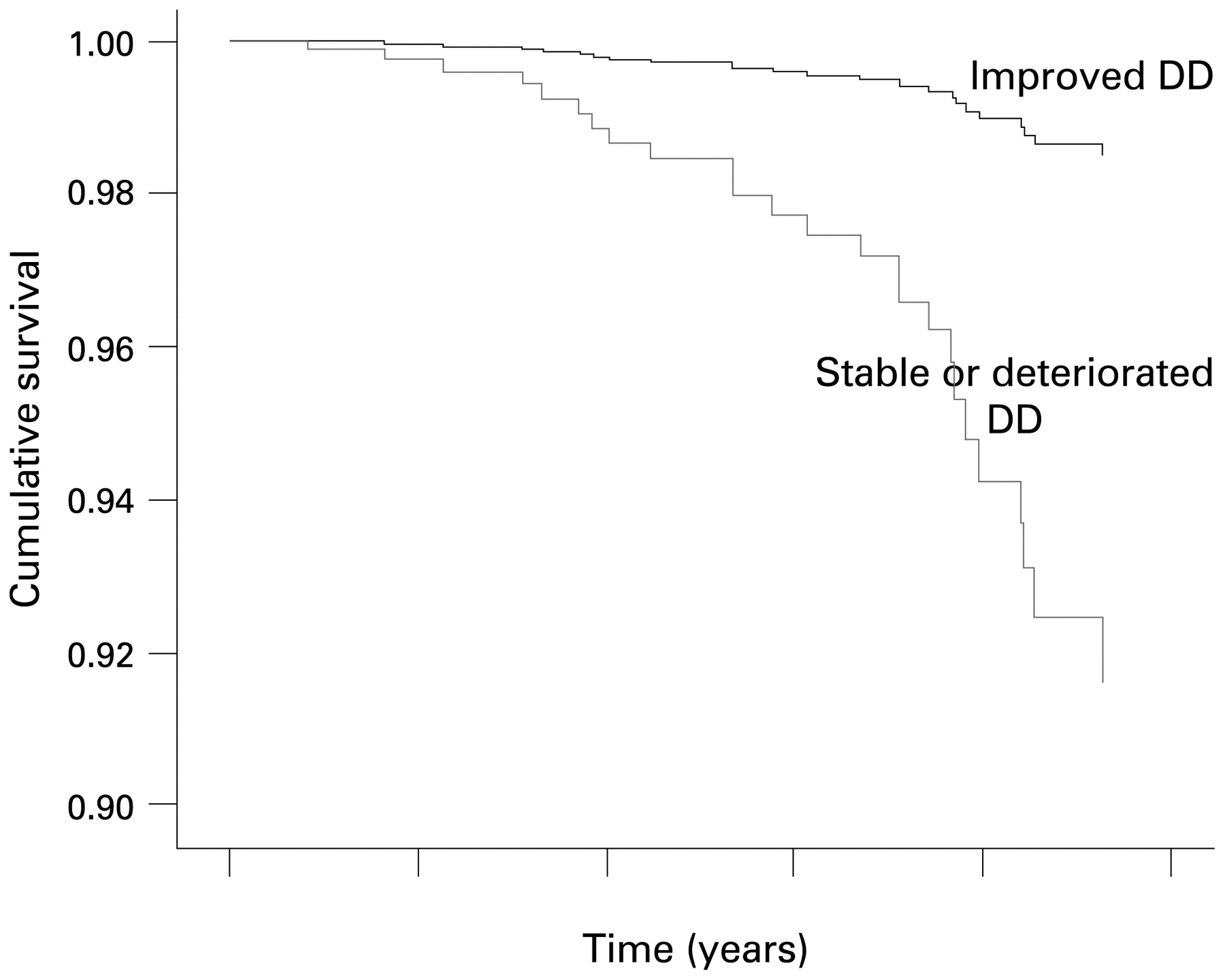
Deterioration of diastolic class was associated with presence of renal impairment. Improvement of diastolic class was associated with lesser requirement for medical therapy (inhibitors/antagonists of the renin-aldosterone axis and statins), probably because of a lower prevalence of hypertension. Of those that survived to have a follow-up echocardiogram, the independent correlates of outcomes in the subgroup undergoing sequential echocardiography were age (β = 1.08; 95% CI 1.04 to 1.13; p = 0.004), baseline heart failure (β = 6.28; 95% CI 1.33 to 29.56; p = 0.02) and LA size (β = 1.14; 95% CI 0.98 to 1.34; p = 0.01), co-morbidity (β = 12.56; 95% CI 4.02 to 39.17; p<0.0001), diuretic use (β = 0.43; 95% CI 0.15 to 1.29; p = 0.04) (table 2). When the protective effects of these agents were taken into account in a multivariate model, improvement in diastolic dysfunction was associated with a reduction in mortality (β = 0.17; 95% CI 0.03 to 0.89; p = 0.05) (fig 2).

{kind=link}
{kind=link}
Survival curve comparing improved diastolic dysfunction with stable or deteriorated diastolic dysfunction (DD).
The effects of changes in blood pressure were studied in a subgroup of 74 patients who had blood pressure recorded at the time of their follow-up echocardiograms. In this subgroup, the change in BP in those improving was a reduction of 9 (16) mm Hg, compared to an increment of 2.6 (22) mm Hg in those with stable and 1 (16) mm Hg in those with deteriorating function (p = 0.14). In the patients who had medication changes recorded, those with improved diastolic function had a greater increment in ACE/ARB dose than the remainder (46% vs 18%) but this was not significant (p = 0.22). Similar findings were recorded for β-blockers (19% vs 2%, p = 0.38).
DISCUSSION
The results of this cohort study confirm the association of diastolic function with all-cause mortality that has been demonstrated in previous studies. Baseline diastolic class was an independent predictor of death, irrespective of the presence of a major co-morbidity. In addition, the study shows progression of diastolic dysfunction in a substantial proportion of patients over 5 years, and demonstrates that worsening or ongoing DD is associated with mortality.
Outcome of diastolic dysfunction
Isolated LV DD is present in 35% of hospital-based patients with CCF, who were more likely to be female and hypertensive.20 Survival and 6-month readmission rate are similar in patients presenting with CCF attributable to systolic or diastolic dysfunction.21 Further, increasing severity of DD correlates with a greater degree of structural abnormality and lower EF in a hospital-based setting.22 Evidence of diastolic dysfunction is also associated with reduced quality of life and was an independent risk factor for heart failure and death from cardiac causes.15 Use of diuretics alone has recently been shown to improve quality of life and symptoms of heart failure and when combined with an inhibitor of the renin-aldosterone axis, resulted in minor improvements in ventricular function.22 This study showed a trend to lower systolic BP in those who improved diastolic status, as well as greater increments in anti-hypertensive therapy—although the latter did not reach significance.
The relation between worse levels of diastolic dysfunction and mortality replicates the findings of community-based studies.3 Further, regardless of the class of diastolic dysfunction and when corrected for age, sex and EF, any degree of diastolic impairment was predictive of all-cause mortality. In this study, age, hyperlipidaemia and the presence of a major co-morbidity were also predictive of death.
The association between heart failure and HTN in the context of diastolic dysfunction that was demonstrated in this study is in keeping with previous studies demonstrating that an antecedent history of hypertension is common in patients presenting with diastolic heart failure.4 7 9 12 13 23 24 This relation may be due to myocardial fibrosis, which is important in hypertensive heart disease but has also been shown to correlate with severity of diastolic dysfunction.25
Co-morbid illness
Previous studies have considered the influence of selected co-morbid illnesses. Redfield et al3 considered the influence of vascular risk factors, while Bursi et al26 found no difference in the prevalence of chronic obstructive pulmonary disease and renal impairment in patients with systolic as opposed to diastolic heart failure. These two factors were found to be independent predictors of heart failure admissions and all-cause mortality in a hospital-based cohort study by Berry et al.27 However, other major co-morbidities (for example, terminal malignancy or organ failure) and their potential contribution to mortality in diastolic dysfunction (not heart failure) had not previously been investigated. This is an important point, as many of these patients are elderly and the relation between worsening diastolic function and mortality could potentially have been in part attributable to other co-morbid illness. In the current study, however, we have demonstrated that although the presence of a major co-morbid illness is a predictor of mortality, diastolic class is also independently predictive of outcome.
Progression of DD
The division of diastolic dysfunction into three classes implies progression from one class to the next. However, to our knowledge, no previous studies have shown such progression to occur and the factors that influence this progression. In the current study, over 3.6 years, diastolic function remained stable in approximately half of the study population. Of the remainder, diastolic function deteriorated in 27% and improved in 21%. This suggests that in about half of these patients, diastolic function does not progress with time and the division into stages or classes of severity may erroneously suggest that progression naturally occurs from one stage to the next. From the multivariate model of the predictors of all-cause mortality, progression of diastolic dysfunction, age, clinical evidence of heart failure at the time of echocardiogram, the presence of a major co-morbidity, transmitral flow and diuretic use were each independently associated with outcome. Importantly, the subgroup of patients in whom the degree of diastolic function improved with time showed a statistically significant mortality benefit compared to those whose diastolic function remained stable or deteriorated over time. This is of interest as all patients with initial class III DD who had serial echocardiograms improved to class II on follow up echocardiography. However, only a small proportion of patients (13%) initially identified as class III had serial echocardiograms and of those whose diastolic function improved, only 25% had baseline class III DD. Further, given that the echocardiograms (at baseline and follow-up) were performed in a hospital echocardiography laboratory, it is possible that some of the change in diastolic function was attributable to changes in loading. Load dependent diastolic dysfunction has been shown to occur in normal hearts (animal and human studies) in the context of increased afterload as well as in those with heart disease despite normal haemodynamic measurements.28 29 This may pertain, in particular, to the subgroup of patients with renal failure due to fluid retention.
Limitations
First, regarding acquisition of data, baseline echocardiograms were performed in 2000–1 when measurement of E′ was not routine. Further, technical limitations of the scan necessitated the exclusion of approximately 10% of patients initially identified predominantly because mitral inflow velocities could not be measured. Patients excluded because of the presence of AF (which prohibited the analysis of transmitral flow) may also have had DD, which was not assessed. Second, information on medication use is derived from prescriptions and compliance with medications was not assessed. Similarly, BP measurements were predominantly recorded in hospital or at outpatient appointments—only a minority of patients had ambulatory 24-hour BP monitoring and therefore, the degree of control was difficult to assess.
Conclusions
DD is associated with all-cause mortality, which is independent of other major co-morbidities—a potential contributing factor with only limited consideration in previous studies. In a subgroup of patients we have also tracked the natural history of diastolic dysfunction which, to our knowledge, has not been done previously. The degree of diastolic function remained stable in only half of the patients, with a mortality benefit being seen in those whose diastolic function improved.
REFERENCES
Footnotes
Funding: Funded in part by a project grant (456139) from the National Health and Medical Research Foundation, Canberra, Australia.
Competing interests: None.