Article Text

Abstract
Objective: To determine the efficacy of statin treatment in atrial fibrillation (AF) prevention in women.
Design: Cohort study using data obtained in the Heart and Estrogen/Progestin Replacement Study (HERS).
Setting: Secondary analysis of a multicentre, randomised controlled clinical trial.
Patients: 2673 Postmenopausal women with coronary disease.
Main outcome measures: AF prevalence at baseline and incident AF over a mean follow-up of 4.1 years.
Results: 88 Women with AF were identified: 29 at baseline and 59 during follow-up. Women with AF were significantly less likely to be taking a statin at study enrolment than those without AF (22% vs 37%, p = 0.003). Baseline statin use was associated with a 65% lower odds of having AF at baseline after controlling for age, race, history of myocardial infarction or revascularisation and history of heart failure (odds ratio 0.35, 95% confidence interval (CI) 0.13 to 0.93, p = 0.04). The risk of developing AF during the study among those free from AF at baseline, adjusted for the same covariates, was 55% less for those receiving statin treatment (hazard ratio 0.45, 95% CI 0.26 to 0.78, p = 0.004).
Conclusions: Statin treatment is associated with a lower prevalence and incidence of AF after adjustment for potential confounders in postmenopausal women with coronary disease.
Statistics from Altmetric.com
Atrial fibrillation (AF) is the most common arrhythmia in the USA, affecting over two million people.1 While women have a lower incidence rate of AF than men, they comprise half of those with the condition, owing to an over-representation of women among the elderly population.2–4 Several studies have demonstrated differences between women and men in the natural history of AF and incidence of its complications, with women experiencing more frequent recurrences of paroxysmal AF and higher rates of thromboembolism and stroke.5–11
Inflammation is increasingly being understood to play an important role in the pathophysiology of AF,12 13 as shown, in part, by increased levels of inflammatory markers in those with AF14–17 and the presence of inflammation on their atrial biopsy specimens.18 This has led to the exploration of non-antiarrhythmic agents for AF prevention, with statins among the most promising. Recent studies have examined the role of statins for AF prevention in multiple settings19–36; however, the vast majority of all study participants were men and none of the studies focused specifically on women.
Given the observed differences between women and men for multiple aspects of AF and the established fact that gender may significantly influence the effect of medicines, the efficacy of statin treatment for AF prevention may not be equivalent between the sexes. The Heart and Estrogen/Progestin Replacement Study (HERS) offers a unique opportunity to examine the role of statin treatment in a large cohort of women with coronary artery disease.
METHODS
The HERS design has been previously described in detail.37 Briefly, 2763 postmenopausal women <80 years of age with known coronary heart disease (CHD) were randomised to receive either 0.625 mg conjugated equine oestrogens plus 2.5 mg medroxyprogesterone acetate in one daily pill (n = 1380) or identical placebo (n = 1383). CHD was documented in the form of myocardial infarction (MI) in 39% of study participants, ⩾50% narrowing of ⩾1 coronary artery in 82%, catheter-based coronary revascularisation in 39% and surgical coronary revascularisation in 37%. The primary outcome was death from CHD or non-fatal MI. Average follow-up duration was 4.1 years.
For this analysis, baseline characteristics were obtained by patient interview at study enrolment. The presence of AF was assessed by standard 12-lead electrocardiograms (ECG) obtained at study enrolment and subsequently at yearly follow-up visits. A total of 2673 (97%) of the 2763 women included in the HERS trial met criteria for study inclusion. Subjects were excluded from the current analysis if they did not have a baseline ECG and at least one follow-up ECG (n = 0). In addition, subjects with atrial flutter (n = 11), wandering atrial pacemaker, supraventricular tachycardia, a paced rhythm, uncertain rhythm classification, or an uncertain detection of P waves were excluded (n = 79 for all other arrhythmias), and a sensitivity analysis was performed to determine if these exclusions meaningfully changed any of the results, which they did not. Study personnel were specifically trained in ECG acquisition and adequate ECG quality was certified at each clinical site. ECG interpretation was performed using NOVACODE software, which produces the classic Minnesota Code Classification.38
Statin use was determined by inspection of prescription bottles and discussion with subjects at the time of study enrolment and at every 4-month follow-up visit thereafter. Start and stop dates of statin use were recorded. Additionally, use of Vaughan Williams class IA, IC and III antiarrhythmic drugs was recorded at study enrolment and every follow-up visit thereafter.
Statistical analysis
The baseline characteristics of participants with either prevalent or incident AF were compared with those of other HERS participants using unpaired t tests, the χ2 test, or Fisher’s exact test as appropriate. Statin use was examined as a predictor of both AF prevalence and incidence. A logistic model was used to estimate the independent association between statin use and prevalent AF at baseline, and a Cox proportional hazards model was used to assess the independent relationship between statin use as a time-dependent covariate and AF detected later in the study. Covariates were selected for the multivariate models based on face validity (ie, race and history of MI or revascularisation) or an association with both the outcome and predictor of interest in univariate analyses with a p value <0.1. Women with AF at baseline were excluded from the analysis of incident AF. Statistical analyses were performed using SAS software V9.1 and were validated by a second, independent analyst.
RESULTS
Of the 2673 women constituting the study cohort, 29 were found to be in AF at the baseline visit, most of whom had AF noted at one or more follow-up visit also; there were 59 incident cases of AF during the study in women who were not in AF at baseline. Compared with those without AF, subjects with AF were older, more likely to have a history of heart failure and reported a higher use of ACE inhibitors at the time of study enrolment (table 1). Patients with AF were significantly less likely to be taking a statin at enrolment (22% vs 37%, p = 0.003).
To examine potential confounders of the relationship between statin use and AF, those taking a statin drug were compared with the study group as a whole. The women taking a statin drug at study enrolment were less likely to be black, have a history of heart failure or myocardial infarction or previous revascularisation, and more likely to report some alcohol use (table 2).
Baseline statin use was associated with an approximate 65% decrease in the odds of having AF at baseline (odds ratio (OR) = 0.36, 95% confidence interval (CI) 0.14 to 0.95, p = 0.04), with nearly identical results after adjusting for age, race, history of MI or revascularisation and history of heart failure (OR = 0.35, 95% CI 0.13 to 0.93, p = 0.04) (fig 1). Inclusion of antiarrhythmic drug use as a marker for AF treatment overall did not alter the results (adjusted OR for baseline statin use 0.35, 95% CI 0.13 to 0.92, p = 0.03). In addition, a sensitivity analysis that included atrial flutter with the outcome of AF did not produce an appreciably different result, nor did limiting the outcome to chronic persistent AF (ie, AF present on every ECG).
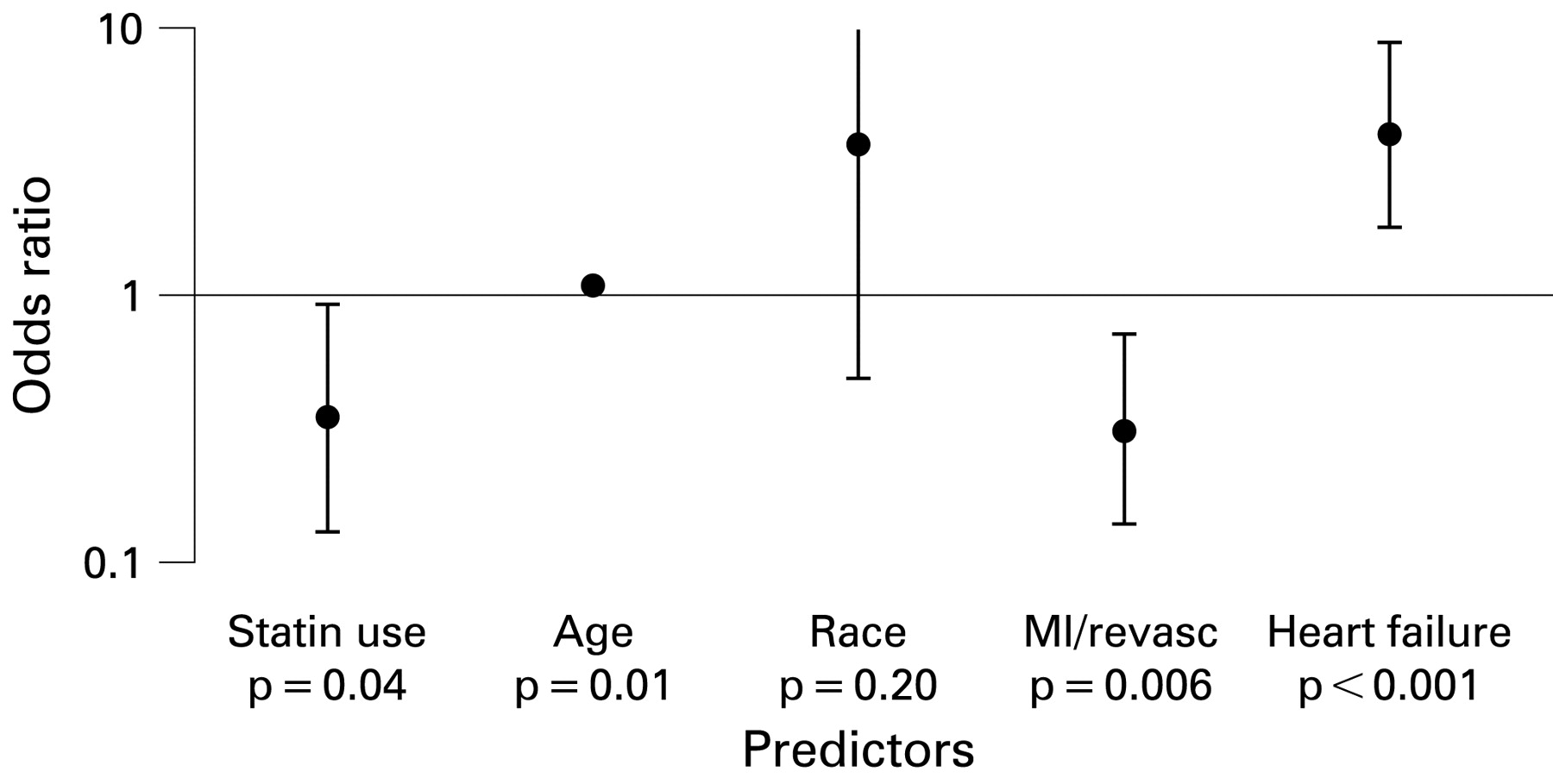
Prevalence of atrial fibrillation at baseline based on the presence of predictors. Points display odds ratios, with adjustment for potential confounders. Bars represent 95% confidence intervals; upper confidence interval for race exceeds the scale. Age, 10-year increase in age; race, Causcasian compared with all others; MI/revasc, history of myocardial infarction or revascularisation.
Statin use was also associated with a lower incidence of AF. The risk of developing AF during the study among those free of AF at baseline was approximately 55% lower for those receiving statin treatment (hazard ratio (HR) = 0.43, 95% CI 0.25 to 0.74, p = 0.002), again with nearly identical results after adjustment for age, race, history of MI or revascularisation, and history of heart failure (HR = 0.45, 95% CI 0.26 to 0.78, p = 0.004) (fig 2). History of heart failure and age were also positively associated with development of AF, with a 7% higher incidence of AF for every additional year of age (HR = 1.07, 95% CI 1.02 to 1.11, p = 0.003). There was no association between randomised treatment assignment (equine oestrogens plus medroxyprogesterone acetate versus placebo) and AF incidence.

{kind=link}
{kind=link}
Incidence of atrial fibrillation at follow-up based on presence of predictors. Points display hazard ratios, with adjustment for potential confounders. Bars represent 95% confidence intervals. Age, 10-year increase in age; race, Causcasian compared with all others; MI/revasc, history of myocardial infarction or revascularisation.
DISCUSSION
As far as we know, this study is the first to extend the exploration of statin treatment in AF prevention to women, a group generally under-represented in the study of both statins and AF. Among the large cohort of postmenopausal women with coronary disease included in the HERS trial, those taking statins had a 65% lower prevalence at baseline and a 55% lower incidence of AF during the study after adjustment for potential confounders.
Statins may prevent AF through multiple pathways, but their effects on inflammation and oxidative stress are probably paramount.12 Evidence linking inflammation with AF includes data from atrial biopsies, inflammatory markers and measurements of atrial voltage among other sources.16–18 39 40 Statins may combat this process by inhibiting leukocyte–endothelium interaction and attenuating leukocyte infiltration,41 as well as by antagonising oxidant pathways,42 thereby protecting atrial tissue from damage and resultant structural remodelling. Statins increase nitric oxide synthesis,43 potentially protecting the atrial myocardium during ischaemia.44 It has also been postulated that they prevent electrical remodelling and alter the electrophysiological milieu through antisympathetic activity, and have direct electrophysiological effects on ion channels and potential indirect effects via the angiotensin II-dependent pathway.45 Finally, they may simply guard against development of a ready substrate for AF by decreasing cardiovascular ischaemic events and thereby preventing structural heart disease.46
After animal studies demonstrated that statins prevent atrial remodelling and AF promotion in the canine atrial tachycardia and sterile pericarditis models,47 human studies began to explore the possibility of statin treatment for AF prevention.28 29 32 A variety of settings have been employed, including the postoperative period after cardiac and thoracic surgery,19–24 the post-pacemaker setting,25 in patients with AF undergoing ablation and cardioversion procedures,26–31 among people with coronary artery disease and depressed left ventricular function32–35 and in those with paroxysmal AF.36 A meta-analysis and five randomised trials have been published examining the effect of statin treatment for AF prevention.20 21 29 30 36 48 Both the meta-analysis and four of the five trials found that statins decreased AF occurrence.20 21 30 36 48 Importantly, as these trials were limited to subjects already with AF or the postoperative setting, none examined prevention of spontaneous AF, as was studied here. In addition, only one of the trials performed a subgroup analysis of the effect of statin treatment on AF in women, finding a reduction in postoperative AF occurrence in the 21 women included in the treatment group20; the meta-analysis did not examine the effect of statins in women. Among the observational studies, results have been mixed, with many finding an inverse association between statin use and AF,17 20–22 26 29 30 32 33 and others not23–25 29 31 probably, to a large extent, because of the heterogeneity of statin treatments, study designs and subjects.
All these studies included, on average, four men for each woman, and none focused specifically on women. Thus whether the promise of statins in preventing AF would apply to women has remained uncertain until now. This is an important question because AF affects women differently than men. Women have higher heart rates when in AF5 6 and more frequent recurrences of paroxysmal AF.6 7 They sustain more thromboembolisms when not receiving warfarin,8 and may be at increased risk of stroke.9–11 Additionally, data regarding the pathophysiology of AF in women are generally unknown, particularly for inflammation as a potential cause of AF. The sex-based differences described in studies of other cardiovascular disease processes49–52 call for the specific examination of disease pathophysiology and pharmacology in women.
As expected, heart failure and older age were each significantly associated with both a higher prevalence and incidence of AF. Use of ACE inhibitors was higher in the AF group, apparently in contradiction to previous data, which demonstrated a protective effect of ACE inhibitors against AF53; this probably represents confounding by indication (as subjects with heart failure are more likely to be treated with ACE inhibitors and to have AF). Use of ACE inhibitors was not significantly associated with statin use in the univariate model (p = 0.26), making it unlikely to confound the association between statin use and AF, and therefore it was not included in the multivariate model. As those with more cardiovascular disease and hence a higher risk of AF may be more likely to receive statins than not, confounding by indication is probably not responsible for our findings related to statins and AF (which would make statins appear to be associated with more AF). Of note, the low overall use of statin treatment among this population of women with CHD is probably owing to the less aggressive guidelines in place before 1998 when the follow-up for the HERS trial was completed, as well as imperfect compliance with guidelines in general.
Our study has several limitations. ECG diagnoses of AF were made with the aid of computer software as opposed to solely by human adjudicators. While the NOVACODE program has been well validated and extensively used in major clinical trials, its performance in the diagnosis of arrhythmias has not been formally tested. Imperfect sensitivity and specificity in diagnosing AF may have resulted, but as statin exposure is unlikely to affect ECG interpretation, any misclassification of the presence of AF would have been non-differential—that is, occurring to the same extent in those with and without statin use. As a result, bias due to the use of this algorithm would be expected to drive our findings towards the null hypothesis, a type II error, suggesting that the magnitude and significance level of the observed associations somewhat understate the true associations.
An additional limitation of the study is the relatively infrequent (yearly) capture of ECGs and lack of additional mechanisms of AF diagnosis, such as patient questionnaire. However, these also would probably have affected both exposure groups equally, and therefore may have limited our ability to see a difference between groups, but should not have created a spurious association.
While we cannot confirm that women receiving statin treatment were not also being treated more aggressively for AF, such as with more cardioversions, adjustment for antiarrhythmic drug use did not alter our results, suggesting that this is probably not the case.
Finally, we cannot rule out the possibility that healthcare providers were less likely to use statin treatment in women with AF—for example, owing to concern about drug–drug interaction with simvastatin and warfarin. New occurrence of AF in our study was not associated with increased likelihood of cessation of statin treatment, nor was presence of AF associated with decreased likelihood of initiating statin treatment, suggesting that this was not a common concern of study healthcare providers.
CONCLUSIONS
For the first time, we have shown that statin treatment is associated with both a reduced incidence and prevalence of AF in a cohort of women. Specifically, in postmenopausal women with coronary heart disease, AF prevalence was 65% lower and AF incidence was 55% lower in those receiving statin treatment both before and after adjustment for multiple potential confounders. Women with AF may therefore be excellent candidates for new antiarrhythmic treatments aimed at the underlying atrial substrate.
REFERENCES
Supplementary materials
Web only appendices 95;9:704-708
Files in this Data Supplement:
Footnotes
Funding: This work was made possible by a fellowship grant from the American Heart Association Western States Affiliate (CNP), grant number KL2 RR024130 from the National Center for Research Resources, a component of the NIH (GMM), and an American Heart Association Beginning Grant-in-Aid Award (GMM).
Competing interests: None.
Ethics approval: Ethics committee approval obtained.