Article Text

Abstract
Background Myeloperoxidase (MPO) is a leucocyte enzyme that catalyses the formation of a number of reactive oxidant species.
Objective The purpose of this study is to evaluate the relationship between angiographic coronary plaque morphology in patients with unstable angina pectoris (UAP) or stable angina pectoris (SAP) and MPO levels.
Patients and design Plasma MPO levels on admission were measured in 236 patients with UAP, 146 with SAP and 85 control subjects using an ELISA kit. The angiographic morphology of the culprit lesion was classified into two types, simple or complex, based on the Ambrose classification. In addition, 61 atherectomy specimens obtained from a different cohort of patients with UAP and SAP were studied immunohistochemically for MPO.
Results Median (IQR) plasma MPO levels in patients with UAP with a complex lesion were significantly higher than in patients with a simple lesion (41.9 (21.7–73.7) ng/ml vs 20.5 (15.9–27.9) ng/ml, p<0.0001), but there was no significant difference between the two groups in patients with SAP. On multivariate analysis, raised plasma MPO levels and Braunwald class III were independent factors for angiographically-detected complex lesions (adjusted OR 12.49, 95% CI 3.24 to 48.17, p=0.0002). In the atherectomy specimens the number of MPO-positive cells in patients with UAP with complex lesions was significantly higher (p<0.0005) than in patients with simple lesions. Moreover, in this cohort, plasma MPO levels were positively correlated with the number of MPO-positive cells in atherectomy specimens (R=0.42, p=0.024).
Conclusions This study shows that increased expression and plasma MPO levels are closely related to the presence of angiographically-detected complex lesion morphology in patients with UAP.
- Atherosclerosis
- coronary artery disease
- angina-unstable
- myeloperoxidase
Statistics from Altmetric.com
Coronary vascular inflammation plays a pivotal role in most cases of acute coronary syndromes. As previously demonstrated by us and others, macrophages, T lymphocytes and neutrophils are the dominant types of inflammatory cells in human coronary unstable, eroded or ruptured plaques.1 2
Unstable angina pectoris (UAP) is a clinical heterogeneous condition in which the severity of symptoms and the risk of progression to infarction or of sudden death vary widely between reported clinical series.3 4 Previous clinical studies have reported that angiographic findings of culprit lesions in patients with UAP frequently appear to be irregular and contain filling defects likely to represent plaque disruption and/or thrombus.5–8 Pathological studies showed that these angiographic appearances were caused by plaque disruption in which a mass of thrombus projected into the lumen but antegrade flow still remained.9 Moreover, in a previous immunohistochemical study, atherectomy specimens from patients with UAP with angiographic complex lesions had a greater percentage of macrophages than those from patients with angiographic simple lesions.10
Myeloperoxidase (MPO) is an abundant haemoprotein released mainly by activated neutrophils and present in some tissue macrophages such as those in vascular lesions.11–13 MPO has been linked to the development of lipid-rich soft plaque,14 the activation of protease cascades affecting the stability and thrombogenicity of plaque.15 Moreover, MPO levels have been shown to predict the risk of clinical events in subjects presenting with chest pain or acute coronary syndromes.16–23
In the present study we measured plasma MPO levels in patients with UAP and those with stable angina pectoris (SAP) and investigated whether there is a relationship between plasma MPO levels and angiographic coronary lesion morphology. Additionally, in a second group of patients with UAP and SAP we examined immunohistochemically the presence of MPO-positive cells using specimens obtained by directional coronary atherectomy (DCA) and evaluated the association between the angiographic plaque morphology of the culprit lesion and the infiltration of MPO-positive cells in these atherectomy specimens. We also investigated the association between the number of MPO-positive cells in atherectomy specimens and plasma MPO levels.
Methods
The present study comprised two distinct groups: group I consisted of 382 patients from whom plasma MPO levels were obtained and group II consisted of 61 different patients from whom atherectomy specimens were obtained. In the group II cohort we were able to obtain plasma MPO levels from 28 patients with UAP.
Group I (plasma MPO)
Patients
This cohort consisted of 236 consecutive patients with UAP who underwent coronary angiography within 3 days of hospital admission and had angiographically documented narrowing of at least 70% of the luminal diameter of a major coronary artery6 between April 2006 and December 2008. Patients with variant angina, concomitant inflammatory diseases, renal failure or neoplastic diseases were not entered in the study. The patients with UAP were further divided into class I (n=84), class II (n=22) and class III (n=130) according to Braunwald's criteria.4 All patients had primary UAP, as defined by subclass ‘B’ of the Braunwald classification. After being admitted, all patients received aspirin, with 75% of the patients receiving antianginal treatment (β blockers, nitrates or calcium-channel alone or in combination). High-risk patients were also treated with intravenous heparin or intravenous nitroglycerin. Before admission, lipid-lowering agents were administered to 33 patients but none used antioxidant drugs. In addition, plasma MPO levels were measured in 146 patients with SAP and in 85 normal subjects. SAP was defined as chest pain typical of cardiac ischaemia on exertion. All patients with SAP had undergone coronary angiography and had angiographically documented narrowing of at least 70% of the luminal diameter of a major coronary artery. Normal subjects comprised 85 age- and gender-matched healthy volunteer blood donors (53 men and 32 women; mean±SD age 63±9 years). The following measurements were performed: serum levels of total cholesterol, high density lipoprotein (HDL) cholesterol and LDL cholesterol, triglycerides, serum high sensitivity C-reactive protein (hs-CRP) levels, leucocyte count, neutrophil count and plasma MPO levels.
Biochemical analysis
Venous blood samples from all patients were obtained on admission to the hospital, prior to heparin administration. Serum hs-CRP levels were assayed with the use of latex-enhanced immunonephelometric assays on a BN II analyser (Dade Behring, Newark, Delaware, USA). Plasma MPO levels were measured with an ELISA method (Oxis) according to procedures previously reported.17
Group II (MPO expression in atherectomy specimens and plasma MPO)
Patients
Coronary atherectomy specimens were obtained by DCA performed between December 2005 and December 2007 from the culprit lesions in 61 patients who presented with either SAP (n=28) or UAP (n=33). Fifteen of the patients have been reported in another study.24 25 The patients with UAP consisted of 13 patients in Braunwald class I, 2 in class II and 18 in class III. The culprit lesion was identified using clinical, ECG and angiographic data. The time interval between diagnostic coronary angiography and DCA ranged from 0 to 3 days. Immediately after DCA, the tissue specimens were carefully orientated along their longest axis, snap frozen, stored at –80°C and then serially sectioned at 6 μm thickness and fixed in acetone. Every first section was stained with haematoxylin-eosin and the other sections were used for immunohistochemical staining. In addition, venous blood samples from 28 of the 33 patients with UAP were obtained prior to heparin administration, and plasma MPO levels and serum hs-CRP levels in these 28 patients were also measured according to procedures previously reported.17
Immunohistochemistry
The cellular components were analysed using monoclonal antibodies against smooth muscle cell (SMC) actin (1A4, DAKO, Glostrup, Denmark), macrophages (EBM11, DAKO), neutrophils (CD66b, Beckman Coulter, Fullerton, California, USA) and MPO (MPO-7, DAKO). In addition, platelets were detected with a monoclonal antibody against GPIIb/IIIa (CD41, DAKO). Non-immune mouse IgG serum (DAKO) served as a negative control. Sections were incubated at 4°C overnight or 1 h at room temperature and then subjected to a three-step staining procedure using the streptavidin-biotin complex method (SABC) for detection. Peroxidase activity was visualised with 3-amino-9-ethyl-carbazole (10 min, room temperature) and the sections were faintly counterstained with haematoxylin. Simultaneous identification of SMCs and macrophages was carried out using two primary antibodies to different IgG subclass proteins (1A4/CD68), as reported previously.26 To identify cell types that stained positive for MPO, immunodouble staining with neutrophils (CD66b) or macrophages (CD68) and MPO were also performed according to the method previously reported with minor procedural modifications.26
Quantitative methods
The tissue area occupied by immunostained macrophages, SMCs and GPIIb/IIIa was quantified using computer-aided planimetry and expressed as a percentage of the total surface area of the tissue sections. The numbers of MPO-positive cells and CD66b-positive neutrophils were counted in the entire tissue sections and expressed as the number of cells per mm2 of tissue. MPO-positive cells and CD66b-positive neutrophils within thrombi or tissue-attached blood clots were excluded. Morphometric analysis was performed by a single investigator blinded to the patients' characteristics and histological classifications.
Coronary angiography analysis
Angiography was performed so that each lesion could be viewed from at least two angles. The coronary lesion was identified as the ‘culprit lesion’ based on clinical and ECG findings. In all patients, offline quantitative coronary angiography (QCA) was conducted with the view revealing the highest degree of stenosis. Pre-intervention angiographic morphology was evaluated by two independent observers who were unaware of the patient's clinical status or Braunwald classification. In cases of disagreement, consensus was reached by further joint reading. Angiographic morphology was divided into two types as either simple or complex based on the Ambrose classification.5 In our analysis, total occlusions and intracoronary thrombus were considered complex lesions and were not classified as separate angiographic variables.6 The interobserver agreement for angiographic morphology was 91% and intraobserver agreement was 92%. Left ventriculography was performed on admission and left ventricular ejection fraction (LVEF) was calculated.
Statistical analyses
Results for normally distributed continuous variables are expressed as mean±SD and continuous variables with non-normal distribution are presented as median (interquartile range). The two groups were compared with an unpaired Student t test or Mann–Whitney U test when the variance was heterogeneous. Statistical comparisons between more than three groups were performed by one-way analysis of variance (ANOVA) and post hoc multiple comparison by the Scheffe test. Levels of MPO and hs-CRP did not distribute normally so logarithmically-transformed values of MPO and hs-CRP were used as variables for statistical analyses. Categorical variables were compared with the χ2 test. Multivariate logistic regression analysis was performed to identify independent factors associated with angiographically-detected complex lesions. Pearson correlation coefficients were calculated to assess the relationship between log-transformed MPO or hs-CRP levels and diameter stenosis (DS), minimal lumen diameter (MLD) or the number of MPO-positive cells. Values of p<0.05 were considered significant.
Results
Group I
Plasma MPO levels and clinical severity
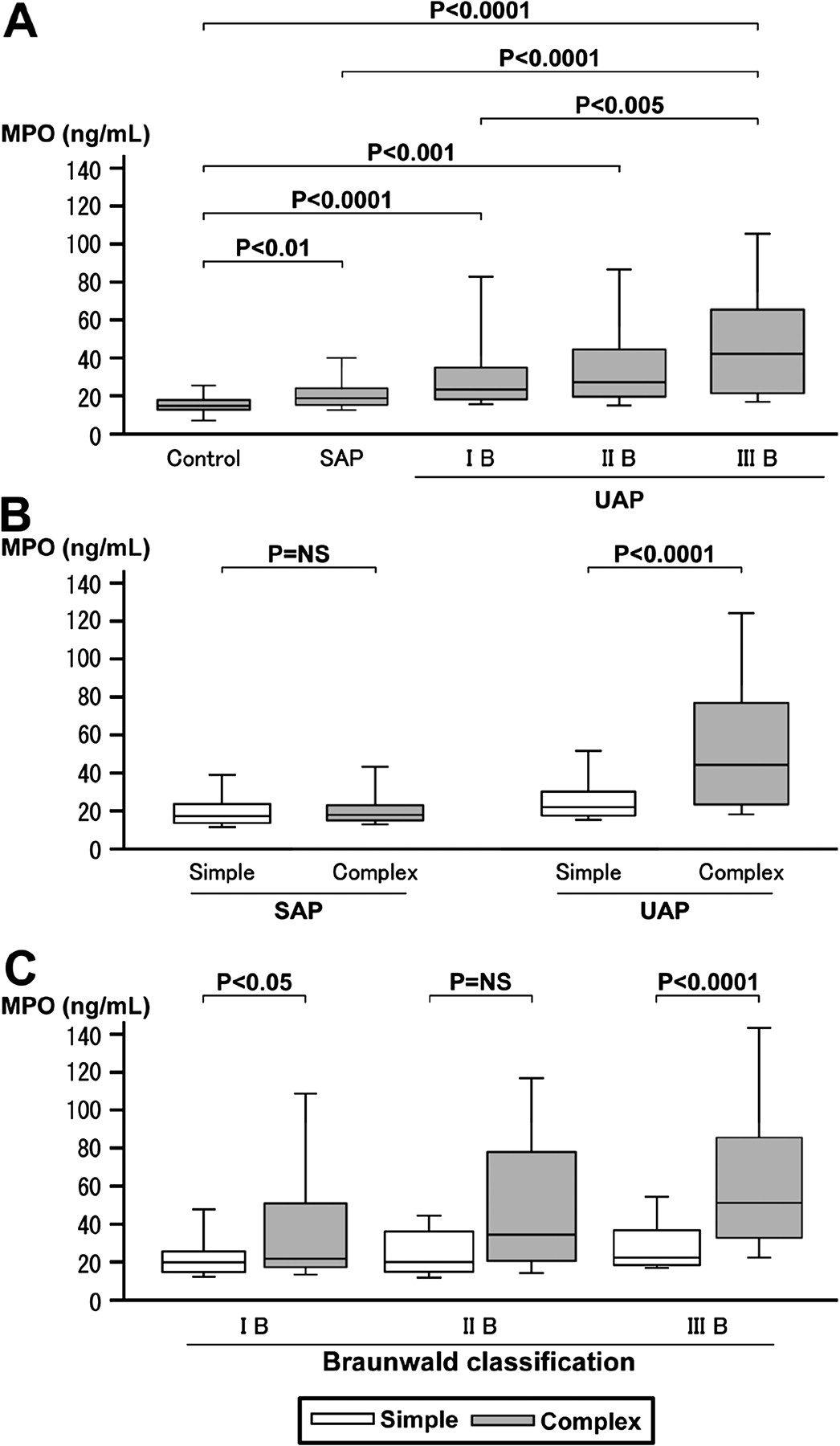
As shown in figure 1A, plasma MPO levels in patients with class III UAP were significantly higher than in patients with class I UAP (p<0.005), patients with SAP (p<0.0001) or in control subjects (p<0.0001) (class III UAP: 39.9 (19.7–62.5) ng/ml; class II UAP: 25.3 (18.6–42.3) ng/ml; class I UAP: 21.6 (17.0–31.9) ng/ml; SAP: 18.7 (15.4–24.1) ng/ml; controls: 15.6 (13.9–18.8) ng/ml). The plasma levels of MPO in patients with SAP and those with class I UAP or class II UAP were also significantly higher than those in control subjects (SAP vs control, p<0.01; UAP class I vs control, p<0.0001; UAP class II vs control, p<0.001).
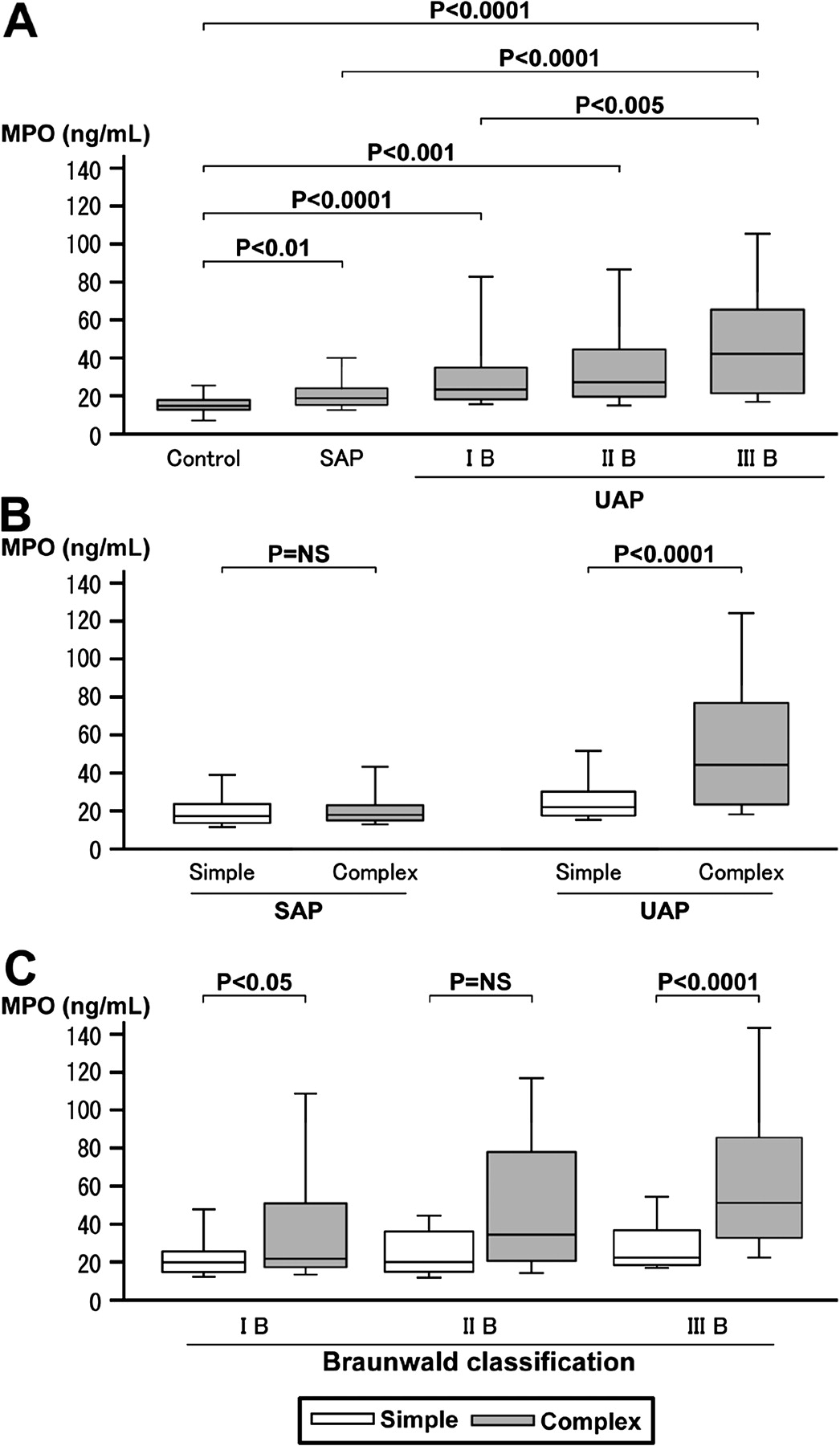
(A) Plasma myeloperoxidase (MPO) levels in patients with unstable angina pectoris (UAP) with Braunwald classes I, II and III, patients with stable angina pectoris (SAP) and control subjects. (B) Relationship between plasma MPO levels and coronary angiographic morphology (simple or complex) in patients with SAP and UAP. (C) Relationship between plasma MPO levels and coronary angiographic morphology (simple or complex) in patients according to Braunwald classification.
Plasma MPO levels and coronary angiographic morphology
There was no significant correlation between plasma MPO levels and DS or MLD of the culprit lesion in patients with SAP or UAP (SAP: MPO vs DS, p=0.96; MPO vs MLD, p=0.50; UAP: MPO vs DS, p=0.59; MPO vs MLD, p=0.58). In this group I cohort, 52 of the 146 culprit lesions in patients with SAP and 139 of the 236 culprit lesions in patients with UAP showed angiographic evidence of a complex lesion. Table 1 shows the characteristics of patients with angiographically-detected simple and complex lesions. In patients with UAP with a complex lesion, Braunwald class III was more frequent than in those with a simple lesion (62% vs 45%, p=0.01). In the QCA analysis, pre-procedure MLD and DS in patients with a complex lesion were significantly higher than in those with a simple lesion (SAP: MLD, p<0.001; DS, p<0.001; UAP: MLD, p=0.04; DS, p=0.02). As shown in figure 1B, plasma MPO levels in patients with UAP with a complex lesion were significantly higher than in those with a simple lesion (41.9 (21.7–73.7) ng/ml vs 20.5 (15.9–27.9) ng/ml; p<0.0001); however, there was no significant difference between those with complex and those with simple lesions in patients with SAP (19.3 (16.3–24.0) ng/ml vs 18.2 (14.8–24.7) ng/ml).
Clinical and angiographic characteristics of patients with SAP and UAP in whom MPO was quantified between angiographically-detected simple versus complex lesion groups
Moreover, as shown in figure 1C, plasma MPO levels in patients with a complex lesion were significantly higher than those in patients with a simple lesion in each of Braunwald class I and class III (class I: simple 20.7 (15.9–26.0) ng/ml, complex 27.6 (18.1–50.4) ng/ml, p<0.05; class II: simple 21.5 (17.1–37.1) ng/ml, complex 35.5 (21.7–73.7) ng/ml; p=NS; class III: simple 19.5 (16.1–32.0) ng/ml, complex 47.5 (29.9–81.0) ng/ml, p<0.0001).
To identify independent factors associated with angiographically-detected complex lesions in patients with UAP, a multivariate logistic regression analysis was performed using age, gender, risk factors, Braunwald class III, prevalence of elevated levels of troponin T, HDL cholesterol and LDL cholesterol, pre-procedure MLD, LVEF, neutrophil counts, serum hs-CRP levels and plasma MPO levels. Multivariate analysis showed that plasma MPO levels and Braunwald class III were independent factors associated with angiographically-detected complex lesions (MPO: adjusted OR 12.49, 95% CI 3.24 to 48.17, p=0.0002; Braunwald class III: adjusted OR 2.80, 95% CI 1.32 to 5.94, p=0.0073). In addition, multivariate analysis in patients with Braunwald class III showed that the plasma MPO level was only an independent factor associated with angiographically-detected complex lesions (MPO: adjusted OR 11.22, 95% CI 3.18 to 39.56, p=0.0007).
Group II (MPO expression in atherectomy specimens and plasma MPO)
Immunohistochemical quantification in atherectomy specimens
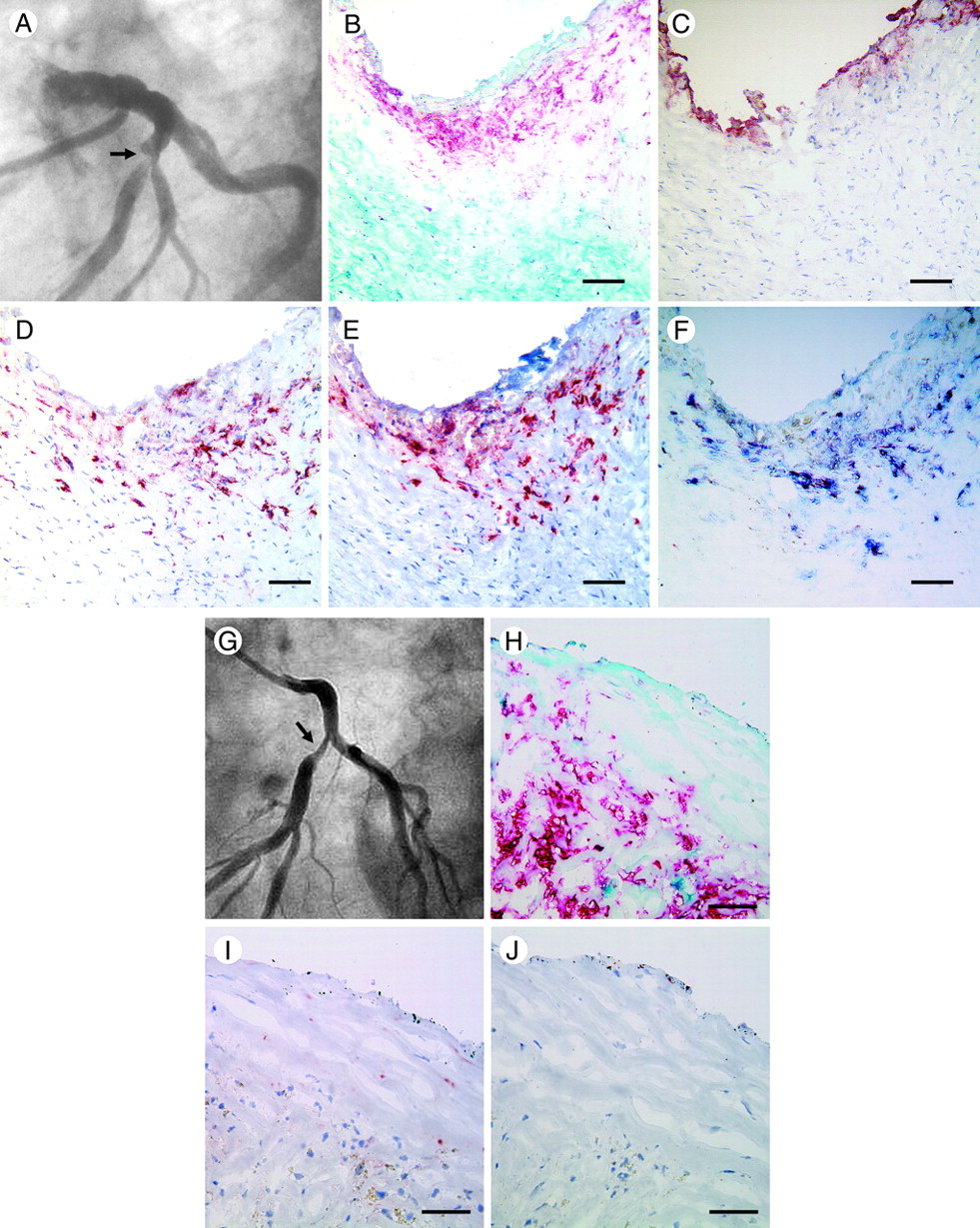
In this group II cohort, 21 of the 33 culprit lesions of patients with UAP and 3 of the 28 culprit lesions of patients with SAP showed angiographic evidence of a complex lesion. Regarding age, male gender and coronary risk factors, there were no statistically significant differences between simple and complex lesions in patients with SAP or UAP. In the 18 patients with UAP with Braunwald class III, angiographic complex lesions were observed in 15 patients (83%) and angiographic simple lesions were found in 3 patients (17%) while, in the 15 patients with Braunwald class I and II, angiographic complex lesions were observed in 6 patients (40%). In the culprit lesions of patients with SAP, 12 of the 28 lesions (43%) contained foci of macrophages and only 1 of the 28 lesions (4%) contained neutrophils. In contrast, all 33 lesions in patients with UAP contained macrophages and SMCs and 22 (67%) showed distinct neutrophil infiltration. In atherectomy specimens from complex lesions in patients with UAP, MPO-positive cell infiltration was frequently found at areas with mural platelet thrombus overlying the site of plaque injury (figure 2A–E). Double immunostaining for MPO and neutrophils or macrophages showed that most of the MPO-positive cells were neutrophils (figure 2F). In contrast, MPO-positive cells were only occasionally found in atherectomy specimens from simple lesions (figure 2G–J). Quantitative analysis showed that the number of CD66-positive neutrophils and MPO-positive cells and the percentage of macrophage-positive area in patients with UAP were significantly higher (CD66b-positive neutrophils, p<0.0001; MPO-positive cells, p<0.0001; macrophages, p<0.0005) than in patients with SAP (figure 3A). In patients with UAP the number of CD66-positive neutrophils and MPO-positive cells was significantly higher in complex lesions than in simple lesions (CD66b-positive neutrophils, p<0.0001; MPO-positive cells, p<0.0005). In addition, the percentage of GP IIb/IIIa-positive area was significantly (p<0.0005) higher in complex lesions than in simple lesions. However, there was no significant difference in the percentage of macrophage-positive or SMC-positive areas between the two groups (figure 3B). With regard to the relationship between MPO-positive cells and the Braunwald classification, the number of MPO-positive cells in Braunwald class III patients was significantly higher (p<0.05) than in Braunwald class I and II patients. Moreover, in both groups the number of MPO-positive cells was significantly higher in complex lesions than in simple lesions (Braunwald class I and II: simple 9.4±8.7 mm2, complex 32.2±18.2 mm2, p<0.05; Braunwald class III: simple 11.8±5.9 mm2, complex 43.9±23.6 mm2, p<0.05, figure 3C). In the group II cohort, plasma MPO levels were positively correlated with the number of MPO-positive cells in atherectomy specimens (R=0.42, p=0.024, figure 3D). In contrast, there was no significant correlation between serum hs-CRP levels and the number of MPO-positive cells in these patients with UAP.
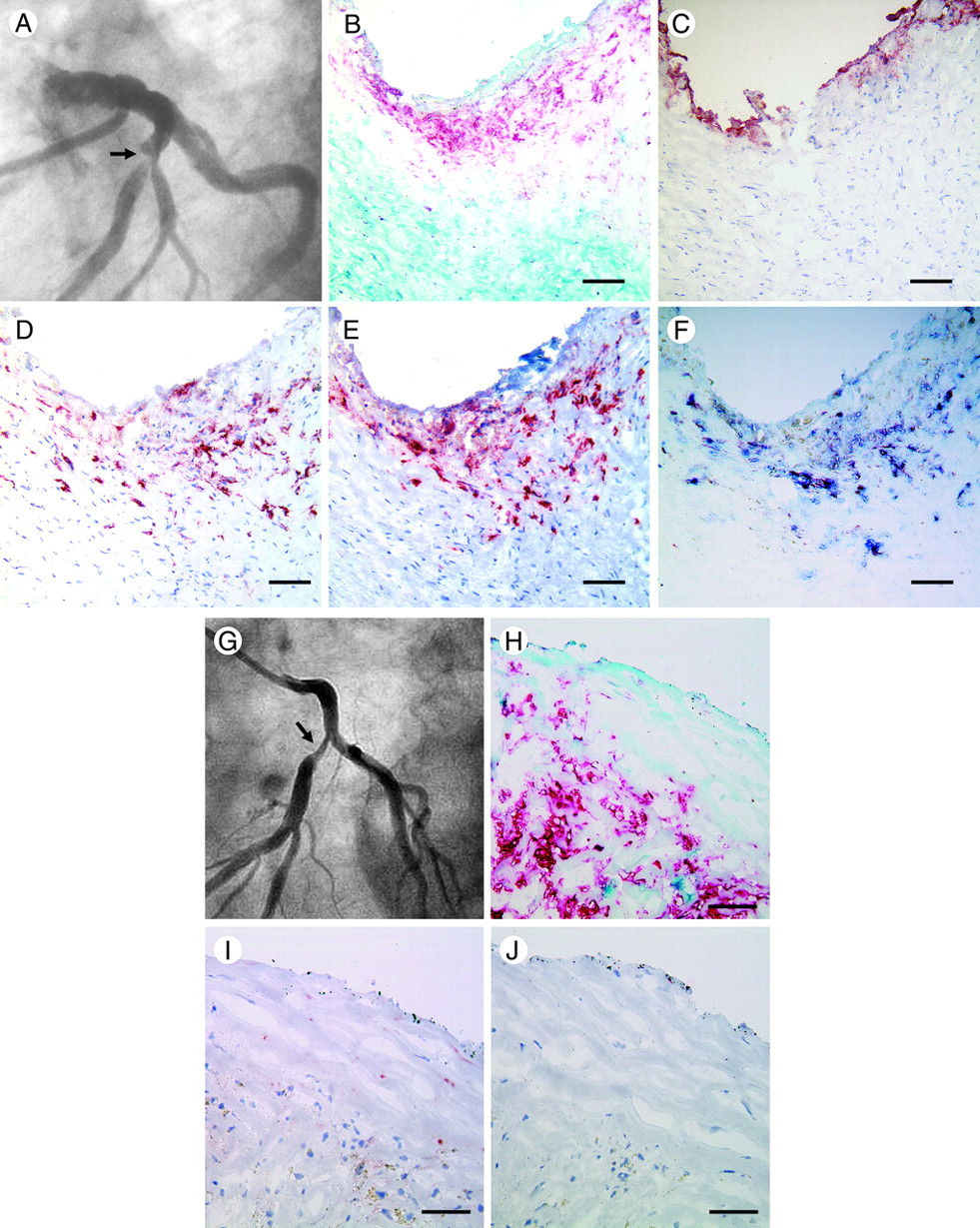
(A) Angiographic image showing a complex lesion (arrow). (B–F) Micrographs of an atherectomy specimen obtained from a complex culprit lesion. (B) Double immunostaining for SMC (turquoise) and macrophage (red). (C) Immunostaining for platelets (GP IIb/IIIa). (D) Immunostaining for neutrophils (CD66b). (E) Immunostaining for MPO (MPO-7). (F) Double immunostaining for MPO-7 (blue) and CD66b (red) shows that most cells show double staining (purple), indicating that most MPO-7-positive cells are neutrophils. Bar: 100 mm (B–F). (G) Angiographic image showing a simple lesion (arrow). (H–J) Micrographs of an atherectomy specimen obtained from a simple culprit lesion. (H) Double immunostaining for SMC (turquoise) and macrophage (red). (I) Immunostaining for CD66b. (J) Immunostaining for MPO. Bar: 100 mm (H–J). MPO, myeloperoxidase; SMC, smooth muscle cell.

{kind=link}
{kind=link}
{kind=link}
(A) Macrophage-positive areas expressed as a percentage of the total surface area and the number of CD66b-positive and myeloperoxidase (MPO)-positive cells/mm2 in atherectomy specimens obtained from the culprit lesion in patients with stable angina pectoris (SAP) and unstable angina pectoris (UAP). (B) Macrophage- and GPIIb/IIIa-positive areas and numbers of neutrophils and MPO-positive cells in patients with UAP with angiographic simple and complex culprit lesions. (C) Relationship between MPO-positive cells and coronary angiographic morphology (simple or complex) in patients according to Braunwald class. (D) Relationship between plasma MPO levels and number of MPO-positive cells in atherectomy specimens.
Discussion
Angiographic complex coronary plaque morphology is the angiographic hallmark of acute coronary syndromes and correlates with pathologic plaque rupture and thrombosis.5–9 Maehara et al, using coronary intravascular ultrasound, showed that complex lesions represent atherogenic vulnerable plaques prone to disruption or actually disrupted plaques.7 To the best of our knowledge, this is the first study to show that increased plasma levels of MPO are related to the presence of angiographically-detected complex lesion morphology. In addition, we have demonstrated the relationship between angiographic coronary lesion morphology and the magnitude of MPO-positive cell infiltration in patients with UAP using coronary atherectomy specimens. Double immunostaining for MPO and neutrophils or macrophages further showed that the majority of MPO-positive cells at the site of angiographic complex lesions were neutrophils. These observations provide strong support for the concept of a direct relationship between the magnitude of MPO-positive neutrophil infiltration and angiographically-detected complex lesions. In addition, in the present study there were no significant correlations between plasma MPO levels and DS or MLD of the culprit lesion in patients with SAP or UAP. Recent studies reported that there were no significant differences between the low-MPO group and the high-MPO group with regard to DS or MLD of the culprit lesion in patients with SAP or acute myocardial infarction.22 23 These previous data are consistent with our results.
Several studies have shown the relationship between biomarkers and plaque instability. Inokubo et al27 demonstrated that the difference in plasma matrix metalloproteinase 9 (MMP-9) and tissue inhibitor of metalloproteinase 1 (TIMP-1) between the great cardiac vein and the aortic root was significantly higher in patients with UAP than in control subjects, which may indicate the release of MMP-9 or TIMP-1 from the site of unstable plaques in patients with UAP. What causes the increased levels of plasma MPO in patients with UAP? A previous study by Biasucci et al showed that circulating neutrophils in patients with acute myocardial infarction and UAP have a low MPO content, indicative of a significant release of MPO from neutrophils related to their activation.12 In addition, Buffon et al reported that, in patients with UAP, widespread neutrophil activation assessed by measuring the neutrophil MPO content occurred across the coronary vascular bed.13 In the present study, plasma MPO levels were positively correlated with the number of MPO-positive cells in atherectomy specimens. These data raise the possibility that the release of MPO from activated neutrophils present at the site of unstable or ruptured plaques may contribute to the increase in MPO in the plasma. However, we could not rule out the possibility that circulating neutrophils become activated by interacting with the surface of unstable plaques and release MPO in patients with UAP. Therefore, one could hypothesise that an increase in MPO levels in the blood may be related to the release of MPO from activated neutrophils present at the site of unstable or ruptured plaques and from circulating neutrophils activated by interaction with the surface of unstable plaques in patients with UAP.
Several studies have reported that plasma MPO levels independently predict future cardiac events in patients with acute coronary syndrome.21 23 We recently demonstrated that increased plasma levels of MPO on admission are associated with impaired myocardial microcirculation following stenting in patients with acute myocardial infarction.23 These findings suggest that plasma MPO levels on admission in patients with acute coronary syndrome can be considered an important biomarker in the management and risk stratification of these patients.
Limitations
This study lacked a contemporary assessment of plaque morphology by ultrasound or optical coherence tomography. Serrano et al have shown that the angiographic characteristics of the culprit lesion correlate poorly with the intensity of the inflammatory response induced by coronary stent implantation in patients with SAP.28 However, in patients w ith UAP, several studies have reported that angiographically complex lesions are strongly associated with disrupted plaques and/or thrombus formation as assessed by ultrasound7 and by angioscopy.8 This is an important observation and lends support to our use of angiographic assessment of plaque complexity. Future studies should confirm an association between plasma MPO levels and plaque morphology as assessed by ultrasound or optical coherence tomography.
Conclusions
This study shows that increased expression and plasma levels of MPO are closely related to the presence of angiographically-detected complex lesion morphology and can be considered an important biomarker in the management and risk stratification of patients with UAP.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Osaka City General Hospital ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Correction