Article Text

Abstract
Background Few reports described outcomes of complete compared with infarct-related artery (IRA)-only revascularisation in patients with ST-elevation myocardial infarction (STEMI) and multivessel coronary artery disease (CAD). Moreover, no studies have compared the simultaneous treatment of non-IRA with the IRA treatment followed by an elective procedure for the other lesions (staged revascularisation).
Methods The outcomes of 214 consecutive patients with STEMI and multivessel CAD undergoing primary angioplasty were studied. Before the first angioplasty patients were randomly assigned to three different strategies: culprit vessel angioplasty-only (COR group); staged revascularisation (SR group) and simultaneous treatment of non-IRA (CR group).
Results During a mean follow-up of 2.5 years, 42 (50.0%) patients in the COR group experienced at least one major adverse cardiac event (MACE), 13 (20.0%) in the SR group and 15 (23.1%) in the CR group, p<0.001. Inhospital death, repeat revascularisation and re-hospitalisation occurred more frequently in the COR group (all p<0.05), whereas there was no significant difference in re-infarction among the three groups. Survival free of MACE was significantly reduced in the COR group but was similar in the CR and SR groups.
Conclusions Culprit vessel-only angioplasty was associated with the highest rate of long-term MACE compared with multivessel treatment. Patients scheduled for staged revascularisation experienced a similar rate of MACE to patients undergoing complete simultaneous treatment of non-IRA.
- Coronary angioplasty (percutaneous coronary intervention)
- ST-elevation myocardial infarction
Statistics from Altmetric.com
Primary percutaneous coronary intervention (PCI) is currently the treatment of choice in patients with acute ST-segment elevation myocardial infarction (STEMI). Coronary artery disease (CAD) is a diffuse process and patients presenting with a coronary syndrome in 20–40% of cases have multiple significant coronary lesions, which confer a substantially increased risk of cardiovascular morbidity and mortality.1–3
Contemporary guidelines recommend dilating only the infarct-related artery (IRA) during the urgent procedure, leaving the other stenosed vessels untreated (culprit-only revascularisation) or to dilate during a second elective procedure (staged revascularisation). Simultaneous treatment of IRA and non-IRA is recommended only in patients with cardiogenic shock.4 5 However, these guidelines are based on the results of earlier studies. With advancing technology and newer antiplatelet drugs, outcomes have improved even in patients undergoing multivessel and higher-risk elective procedures.6 Yet, few reports have described outcomes of multivessel compared with IRA-only revascularisation in patients undergoing urgent mechanical reperfusion for STEMI,7 8 and none have distinguished simultaneous treatment of non-IRA from the staged approach. Therefore, the optimal management of patients with multivessel disease in this setting remains still unclear.
The aim of this study was to compare long-term outcomes of three different strategies during primary PCI in patients with STEMI and multivessel CAD: culprit vessel-only angioplasty; angioplasty of IRA followed by an elective procedure for the treatment of other lesions and simultaneous treatment of IRA and non-IRA.
Methods
Study population
We examined patients with STEMI and multivessel CAD undergoing primary PCI. Between January 2003 and December 2007 in our 24 h catheterisation laboratory we performed 779 primary PCI, among which we identified 263 consecutive patients (33.7%) with multivessel CAD (defined as >70% diameter stenosis of two or more epicardial coronary arteries or their major branches by visual estimation).
Included were patients with the presence of prolonged (more than 30 minutes) chest pain, started less than 12 h before hospital arrival and ST elevation of at least 1 mm in two or more contiguous limb electrocardiographic leads or 2 mm in precordial leads.
Patients with cardiogenic shock at presentation (systolic blood pressure ≤90 mm Hg despite drug therapy), left main coronary disease (≥50% diameter stenosis), previous coronary artery bypass grafting (CABG) surgery, severe valvular heart disease and unsuccessful procedures were excluded from the study. Procedure success was defined as the achievement of an angiographic residual stenosis of less than 30% and a thrombolysis in myocardial infarction (TIMI) flow grade III after treatment of the culprit lesion. Two hundred and fourteen patients were eligible and thus represent the study population.
Before the procedure patients were treated with aspirin, unfractioned heparin and abciximab bolus followed by 12 h infusion. In addition, the protocol included a bolus of N-acetylcysteine 1200 mg and hydration with saline for 12 h after contrast exposure at an infusion rate of 1 ml/kg per hour. Iodixanol (Visipaque) was used as contrast media in all patients. Post-PCI medical oral treatment included aspirin, statins and clopidogrel, unless contraindicated, which was recommended for 30 days in case of bare metal stent implantation and for 12 months in case of drug-eluting stents. Signed informed consent for primary PCI and for the study was obtained from all patients before the procedure.
Soon after every diagnostic angiography, the eligible patients were randomly allocated to three different strategies:
Culprit-only revascularisation (COR): the IRA only was dilated and the other arteries were left untreated.
Staged revascularisation (SR): the IRA only was treated during the primary intervention while the complete revascularisation was planned in a second procedure.
Complete revascularisation (CR): the IRA was opened followed by dilatation of other significantly narrowed arteries during the same procedure.
Before the angioplasty, dedicate software generated a number (1 for the COR group, 2 for the SR group and 3 for the CR group), which allowed the operator to allocate each patient in a specific strategy group. Data were then analysed as intention-to-treat.
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the institution's human research committee.
Definitions and endpoints
Clinical and procedural data were collected by reviewing hospital records and angiographic runs stored in DICOM CDs. Left ventricular ejection fraction (LVEF) was measured by transthoracic echocardiography in all patients soon before the primary PCI in the catheterisation laboratory by one of the interventional cardiologists and at discharge by one of the clinical physicians. The angiographic TIMI flow grade of the infarct artery was estimated before and after completion of coronary balloon angioplasty according to four grades of flow, as previously described.9
We recorded the length of hospitalisation and the occurrence of contrast-induced nephropathy (CIN) in all patients. CIN was defined as an absolute increase in serum creatinine values of 0.5 mg/dl or greater or a 25% or greater relative increase from baseline within 72 h following both primary and elective PCI.10 Chronic renal failure was defined as baseline estimated creatinine clearance of less than 60 ml/minute (according to the Cockroft–Gault formula).11
The primary endpoint of the study was the incidence of major adverse cardiac events (MACE) defined as cardiac or non-cardiac death, inhospital death, re-infarction, re-hospitalisation for acute coronary syndrome and repeat coronary revascularisation. For repeat revascularisation we included all PCI or CABG occurring after the baseline procedure and justified by recurrent symptoms, re-infarction or objective evidence of significant ischaemia on provocative testing.12 Among repeat PCI we excluded staged procedures already scheduled. In the staged group we classified as repeat revascularisation only unplanned procedures. Follow-up was obtained by outpatient visits and phone interviews.
Sample size calculation
The sample size has been calculated on the basis of the primary endpoint (MACE). Given an expected rate of MACE of 17% for the groups undergoing complete revascularisation (both simultaneous and staged) versus 50% for the culprit-only group,13 aiming for a 0.05 α and 0.90 power, a total of 123 patients needed to be enrolled (41 patients per group).14 This has been increased in order to take into account potential losses to follow-up and to power the study.
Statistical analysis
Continuous variables are presented as mean±SD, categorical variables as percentages. Categorical variables were compared among groups using the χ2 test or Fisher's exact test when appropriate, whereas continuous variables were compared with the analysis of variance test. Kaplan–Meier curves were used to represent survival and cumulative incidence of events to the follow-up. For the endpoint ‘death’ patients were censored at death or 20 December 2008 if alive. For MACE patients were censored at the date of first MACE or at the end of follow-up. Follow-up was 100% complete. Cox regression analyses were used to investigate the univariate and multivariable predictors of events during the follow-up. Multivariable models for MACE in follow-up included age, gender and the variables that had p<0.1 at univariate analysis. Data are presented as hazard ratios and 95% CI. All tests were two-sided, a p value less than 0.05 was considered statistically significant. All analyses were performed using SPSS software, version 15.0 for Windows.
Results
Baseline characteristics
Among the 263 patients with STEMI and multivessel disease, we excluded 47 for the following reasons: 21 presented in cardiogenic shock; six had left main coronary disease; nine had previous CABG surgery; seven had severe valvular heart disease. The four patients who experienced an unsuccessful procedure were included in the randomisation process but not in the follow-up analysis. We thus included in the follow-up 214 patients with STEMI and multivessel CAD meeting the inclusion criteria. The mean age was 65.2±12.2 years, 166 (77.5%) were men. The COR group included 84 (39.2%) patients, the SR group 65 (30.4%) patients and the CR group 65 (30.4%) patients. The elective procedure in the SR group was performed on average 56.8±12.9 days after the primary PCI.
Table 1 shows the distribution of baseline characteristics among the three groups. For therapy at discharge we excluded patients who died during hospitalisation. The three groups were similar for age, gender, risk factors, LVEF, enzymatic infarct size, location of the STEMI, TIMI flow grade, use of drug-eluting stents and renal disease, whereas there was a difference in the frequency of three-vessel coronary disease (more represented in the SR group). Nitrate therapy was more frequent in the COR group, whereas the three groups were similar for the other therapies. The incidence of CIN ranged from 1.5% in the CR group to 3.6% in the COR group without a significant difference among groups (p=0.748). The length of hospital stay was similar in the three groups (p=0.348).
Baseline characteristics
Events
After a mean follow-up of 2.5±1.4 years, 23 (10.7%) patients died, 16 (7.4%) from cardiac causes. Throughout the follow-up, 70 (32.7%) patients experienced at least one MACE, 42 (50.0%) in the COR group, 13 (20.0%) in the SR group and 15 (23.1%) in the CR group, p<0.001. The incidence of inhospital death, repeat revascularisation and re-hospitalisation was significantly higher in the COR group (all p<0.05), whereas there was no significant difference in re-infarction among the three groups. Two patients (one in the SR group and one in the CR group) received both a re-PCI and a subsequent CABG. Mortality was more frequent in the COR group although it did not reach statistical significance (table 2).
Rate of outcomes in the three groups
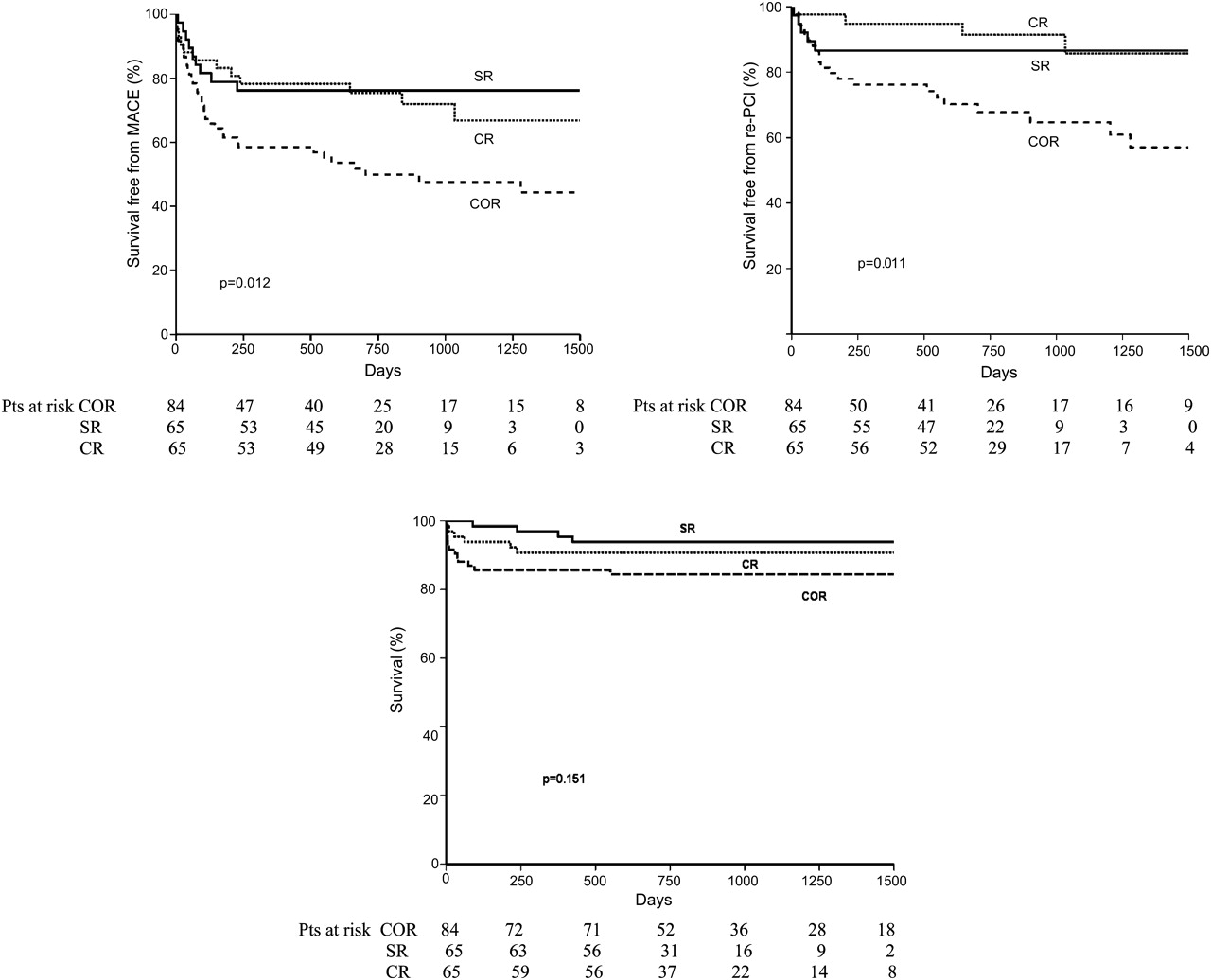
Kaplan–Meier analysis showed a significant difference among the three groups for survival free of MACE and re-PCI (figure 1). Survival free of MACE was worse in the COR group compared with both the CR group (p=0.002) and the SR group (p=0.001), whereas it was similar between the CR and SR groups (p=0.815). Similarly, survival free of re-PCI was worse in the COR group compared with both the CR group (p<0.001) and the SR group (p=0.005), whereas it was similar between the CR and SR groups (p=0.467). In the SR group seven (10.8%) patients had symptoms or evidence of ischaemia requiring unplanned re-PCI, six of these before the scheduled procedure. The mean time between the first and the unplanned procedure was 42.3±22.8 days.

{kind=link}
Kaplan–Meier curves describing survival free of major adverse cardiac events (MACE; upper panel), survival free of re-percutaneous coronary intervention (PCI; middle panel) and overall survival (bottom panel) among the three groups. A solid line indicates the staged revascularisation (SR) group, a dotted line indicates the complete revascularisation (CR) group, a dashed line indicates the culprit-only revascularisation (COR) group.
The COR group showed a tendency for a worse overall survival compared with the other two groups, without reaching statistical significance (p=0.151).
Univariate predictors of MACE
Compared with patients who underwent COR treatment, the other two strategies had a significantly reduced risk of MACE, with a 63% lower risk in the SR group (p=0.003) and a 60% lower risk in the CR group (p=0.002) (table 3).
Univariate predictors of MACE
Other significant univariate predictors of MACE were diabetes mellitus, Killip class, chronic renal failure and CIN.
Multivariable predictors of MACE
The reduced risk of MACE in the SR and CR groups was maintained even after multivariable adjustment for age, gender, diabetes mellitus, LVEF before PCI, Killip class, chronic renal failure and CIN. At multivariable analysis, independent predictors of MACE were COR, chronic renal failure and Killip class (table 4).
Multivariable determinants of MACE
Discussion
The main finding of the present study is that after a mean follow-up of 2.5 years, in patients with multiple coronary lesions treated with primary PCI, multivessel revascularisation had a better outcome than treatment of IRA only. Both the simultaneous treatment of non-IRA vessels and the staged approach resulted in a lower risk of MACE compared with the culprit-only procedure. In particular, patients in the COR group had a higher risk of repeat unplanned revascularisation, re-hospitalisation and inhospital death.
According to current guidelines, PCI should be performed only in IRA, at least in patients without cardiogenic shock.5 This recommendation is based on the hypothesis that single-vessel PCI has a more favourable benefit-to-risk ratio and better financial implications. Some studies suggest that the more conservative strategy of treating only the IRA could avoid the complications arising from longer procedures, such as the larger use of contrast medium with a potentially increased risk of CIN, the increased administration or radiation, as well as the danger of ischaemia in non-infarcted myocardial regions.7 15
In recent years, with the development of new advanced devices and the use of platelet glycoprotein IIb/IIIa inhibitors, the outcome of multivessel PCI has markedly improved.16 17 Some reports have indicated that the multivessel approach as safe and cost-effective. Brener et al18 retrospectively examined more than 100 000 patients with acute coronary syndromes and demonstrated a similar incidence of inhospital events between patients receiving single and multivessel treatment. Ijsselmuiden et al6 randomly assigned 219 patients with acute coronary syndromes to culprit-only versus multivessel revascularisation, and they found that the multivessel approach had better outcomes by decreasing the need for further interventions.
To the best of our knowledge the present study is the first that compares throughout a long follow-up the three most common strategies during primary PCI in patients with multivessel disease: culprit vessel-only (COR group); culprit vessel in an urgent procedure with completion of revascularisation in another elective procedure (SR group) and complete revascularisation during the same procedure (CR group). The three groups were similar for most baseline characteristics and this strengthens our results. We found that, compared with the single-vessel approach, multivessel revascularisation is safe and is associated with a lower risk of MACE at a mean follow-up of 2.5 years. In particular, patients in the SR group had a 63% lower risk of MACE and patients in the CR group had a 60% lower risk. This result is attributable mainly to the lower incidence of inhospital death, re-PCI and re-hospitalisation both in the SR and CR groups compared with the COR group. Furthermore, we found that COR was a significant and strong predictor of MACE even after multivariable adjustment for age, gender, diabetes mellitus, LVEF before PCI, Killip class, CIN and chronic renal failure.
Our findings differ from the HELP AMI study,8 in which in 69 STEMI patients treated with primary PCI the 1-year incidence of repeat revascularisation was similar in single and multivessel strategies. Conversely, the present study is in line with a more recent report by Qarawani et al,13 which observed in a population of 120 patients undergoing primary PCI a lower incidence of re-PCI among those receiving complete revascularisation during a 1-year follow-up. In addition, our data extend to the primary PCI setting the results Kalarus et al,19 which showed the negative effect of incomplete revascularisation in more than 700 patients with myocardial infarction undergoing non-emergent PCI. A possible explanation for the protective effect of multivessel PCI is that it allows a more complete treatment of other potentially unstable plaques. Indeed, the inflammatory reaction arising during acute coronary syndromes and responsible for plaque instability is not limited to the culprit lesion, but involves the entire coronary tree.3
We observed a low incidence of CIN that was similar in the three groups analysed. Marenzi et al20 reported a higher rate of CIN (19%) in 208 patients with STEMI undergoing primary PCI. The authors attributed this increased risk to the generally longer procedural time and larger amount of contrast medium used in urgent procedures. In the present study we used the same criteria to define CIN, but we implemented new preventive measures for CIN (isosmolar contrast media, periprocedural hydration with N-acetylcysteine infusion), which have been shown to reduce the risk of renal complications even in longer and more complex procedures.21 22
Previous studies acknowledge as a potential disadvantage of early complete revascularisation the longer hospital stay with an increase of costs. In the present study the length of hospitalisation was similar in the three groups.
Whereas the outcome in the COR group was significantly worse than in the multivessel approach, we did not find differences in the CR versus the SR group in terms of MACE or re-PCI throughout the follow-up.
Our results suggest that the multivessel approach (either with early complete revascularisation or with a staged procedure) is safe and possibly less expensive than an incomplete approach by reducing the probability of further unplanned procedures and without affecting the length of hospitalisation. We suppose that multivessel revascularisation could decrease the risks and discomfort for patients associated with new unscheduled procedures.
Strengths and limitations
To the best of our knowledge, this is the largest study comparing the three available strategies during primary PCI for patients with STEMI and multivessel CAD. Given the relatively recent enrolment time, all PCI were performed using contemporary devices and therapies, thus this study provides an up-to-date picture of the current practice in STEMI. Moreover, the three groups were fairly homogeneous for most characteristics and this could strengthen our results.
Possible limitations of the study are the imbalance in the number of patients in the three groups and the difference in the presence of three-vessel disease, but these are features of blind and unrestricted randomisation.
Conclusions
In a contemporary homogeneous cohort of patients with STEMI and multivessel CAD treated with primary PCI, COR angioplasty was associated with the highest rate of MACE compared with multivessel treatment. Patients scheduled for staged revascularisation experienced a similar rate of MACE to patients undergoing complete simultaneous treatment of non-IRA. This novel finding of our study should promote further research in order to provide strong enough evidence that may eventually update the current recommendations for patients with multivessel CAD and STEMI.
Acknowledgments
The authors would like to thank all the laboratory nurses and technicians: Chiara Venturelli, Cristina Leonelli, Enrica Melodi, Lina Rosati, Olinda Rombolà, Rebecca Simonetti, Rosa Miccoli and Tiziana Damante. Their work has been fundamental for the realisation of this study.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the Ethics Commitee of Policlinico Hospital, Modena, Italy.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.