Article Text

Abstract
Introduction Microvascular obstruction (MVO) is associated with large acute myocardial infarction (AMI) and lower left ventricular (LV) ejection fraction, and predicts greater remodelling, but whether this effect is abolished by contemporary anti-remodelling therapies is subject to debate. We examined the influence of several infarct characteristics, including MVO, on LV remodelling in an optimally-treated post-AMI cohort enrolled in a clinical trial investigating the potential anti-remodelling effects of eplerenone, using contrast-enhanced cardiac magnetic resonance (ceCMR).
Methods Hundred patients (mean age 58.9±12 years, 77% male) admitted with AMI in the previous 1-14 days underwent ceCMR at baseline (∼4 days), 12 and 24 weeks. The effects on LV remodelling (ie, change in LV end-systolic volume index (▵LVESVI)) of infarct site, transmurality, endocardial extent, and the presence of early and late MVO were analysed. Tests for interaction between MVO persistence and eplerenone therapy were also performed.
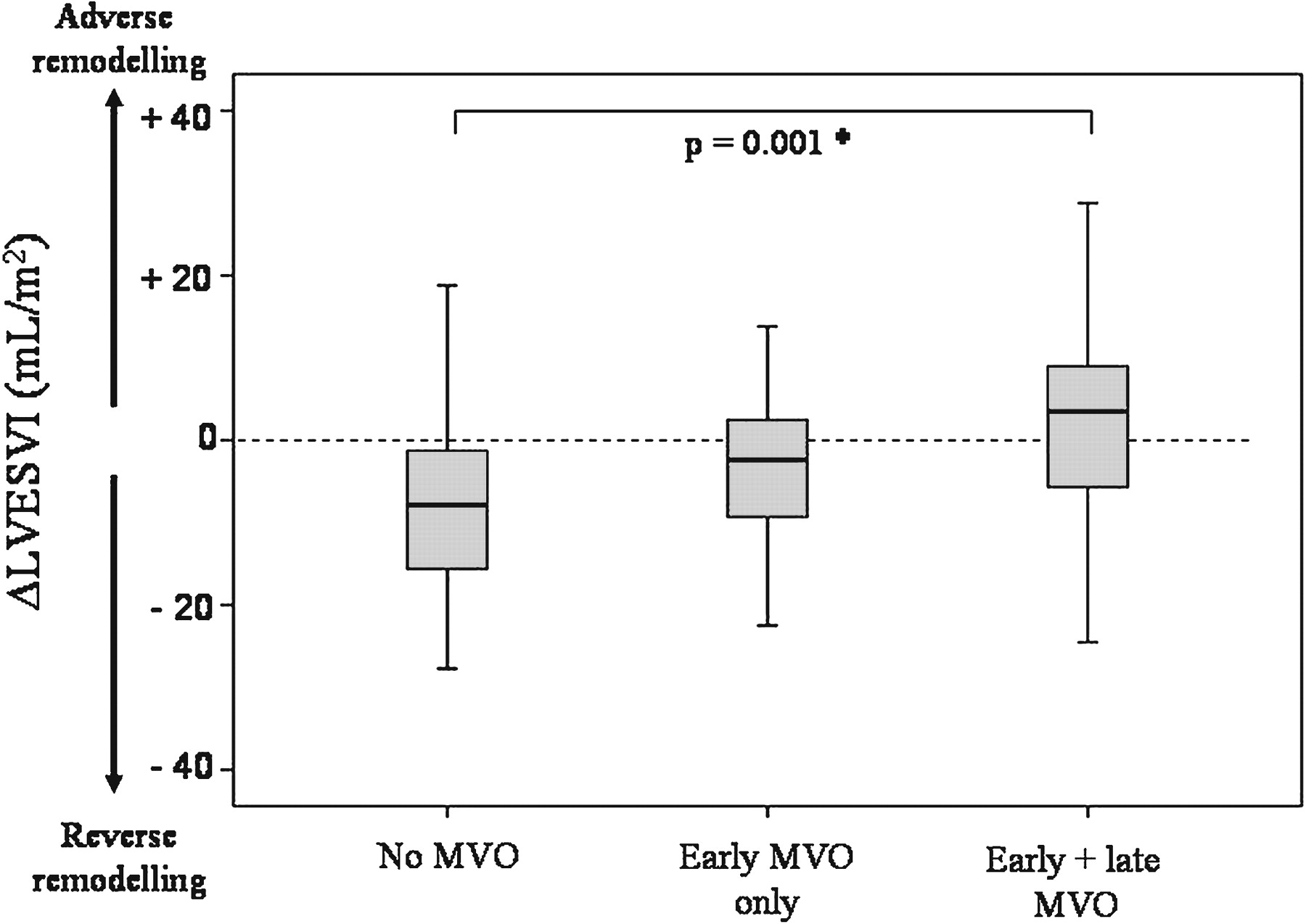
Results Mean baseline infarct volume index decreased from 34.0 (21.2) ml/m2 to 20.9 (12.9) ml/m2 at 24 weeks (p<0.001). Infarct site had no influence on remodelling, but greater baseline infarct transmurality (r=0.47, p<0.001) and endocardial extent (r=0.26, p<0.01) were associated with higher ▵LVESVI. Early MVO was seen in 69 (69%) of patients and persisted, as late MVO, in 56 (56%). Patients with late MVO underwent significantly greater remodelling than those without MVO (▵LVESVI +4.1 (13.4) vs −7.0 (12.7) ml/m2 respectively, p=0.001); those with early MVO only displayed an intermediate ▵LVESVI (−4.9 (13.0) ml/m2)— Abstract 121 Figure 1. Coronary angiography was undertaken in 85/100 (85%) of the cohort; TIMI 3 flow within the infarct-related artery was seen in 42/56 (87.5%) of patients with late MVO and in 32/44 (86.5%) of those without late MVO (p=ns), thus late MVO was seen frequently despite optimal coronary blood flow having been restored at angiography. Interestingly, the presence of (late) MVO was associated with significantly less remodelling in eplerenone- than in placebo-treated patients (▵LVESVI 0.8 (11.0) ml/m2 vs 8.1 (15.2) ml/m2 respectively, p<0.001).

{kind=link}
Conclusions Late MVO on pre-discharge ceCMR remains an ominous predictor of adverse LV remodelling despite powerful anti-remodelling therapy, and may be useful in the risk-stratification of survivors of AMI. Eplerenone may attenuate remodelling more powerfully in patients at the highest risk of remodelling, that is, those with persistent MVO.
- microvascular obstruction
- myocardial infarction
- cardiac magnetic resonance