Article Text

Abstract
Introduction Cardiac resynchronisation therapy (CRT) reduces mortality and morbidity in heart failure patients, however up to 30% of patients do not derive symptomatic benefit. Higher proportions do not remodel. Multi-centre trials have shown echocardiographic techniques are poor at improving response rates. We hypothesised that the degree of acute haemodynamic response (AHR) at implant can predict which patients remodel. We evaluated the relationship between AHR and reverse remodelling (RR) in CRT. Methods 33 patients undergoing CRT (21 dilated & 12 ischaemic cardiomyopathy) were studied. Left ventricular (LV) volumes were assessed pre and post CRT. AHR (LV-dP/dtmax) was assessed at implant using a pressure wire in the LV cavity. The LV lead was placed in potential target veins and the largest percentage rise in LV-dP/dtmax from baseline (AAI or RV pacing with atrial fibrillation) to DDDLV was used to determine optimal LV lead position. RR was defined as reduction in LV end systolic volume (ESV) ≥15% at 6 months.
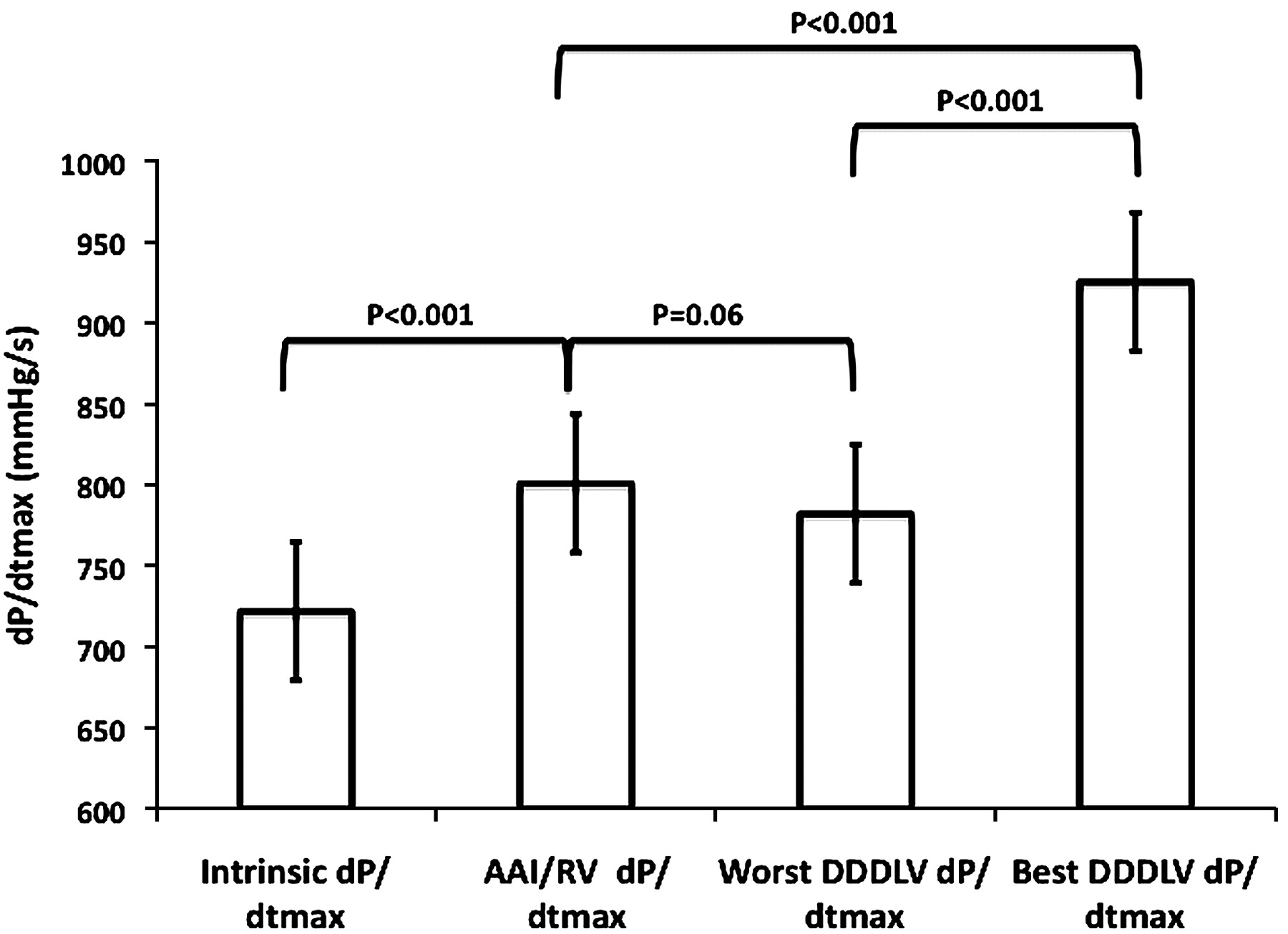
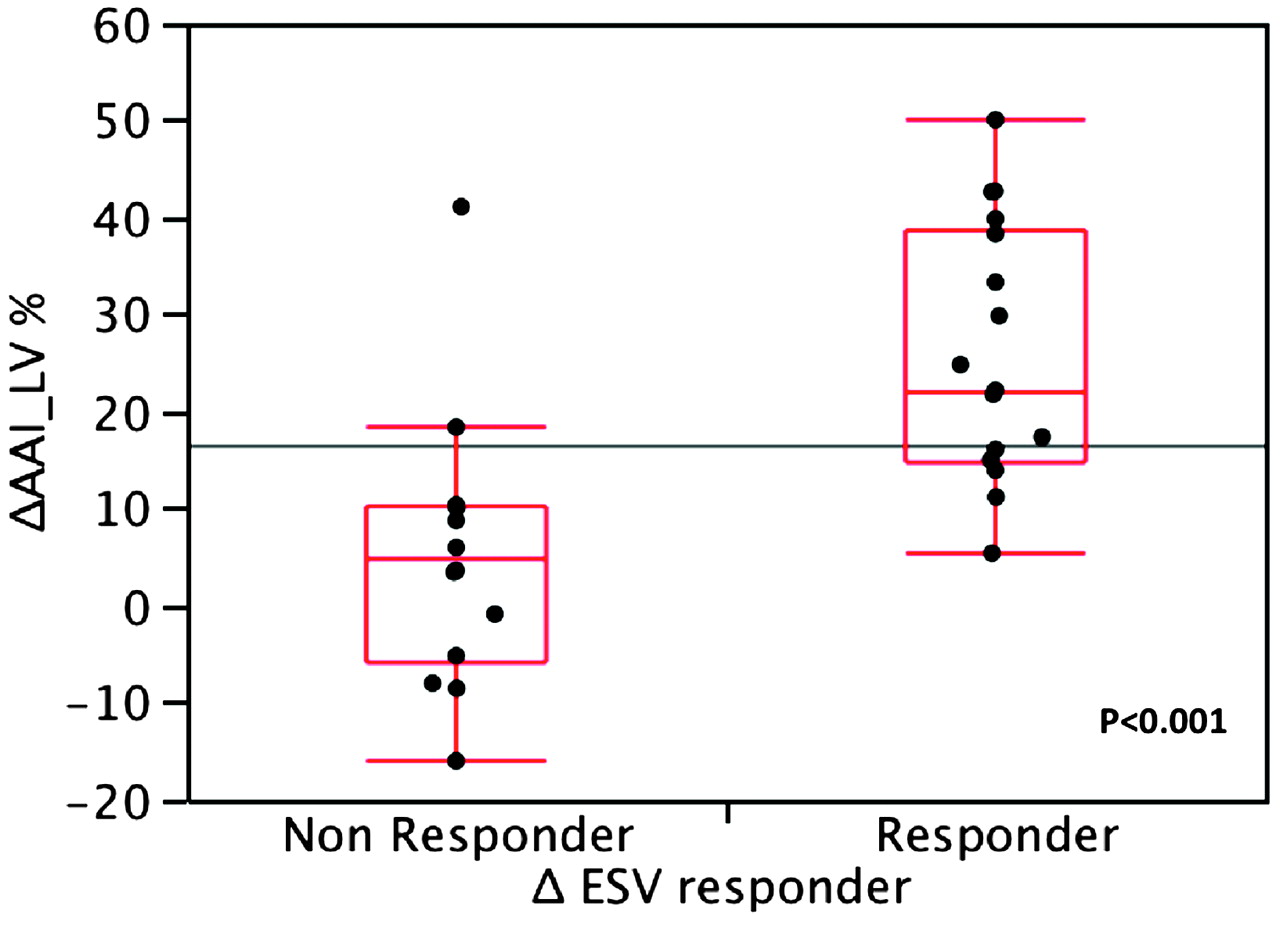
Results LV-dP/dtmax increased significantly from baseline (801±194 mm Hg/s to 924±203 mm Hg/s (p<0.001)) with DDDLV pacing for the optimal LV lead position. There was a significant difference in the percentage rise in LV-dP/dtmax between the best and worst LV lead position (Abstract 90 figure 1). LVESV decreased from 186±68 ml to 157±68 ml (p<0.001). 18 (56%) patients exhibited RR. There was a significant relationship between percentage rise in LV-dP/dtmax and RR for DDDLV pacing (p<0.001) (Abstract 90 figure 2). A similar relationship for AHR and RR in DCM and ICM (p=0.01 & p=0.006) was seen.

{kind=link}
{kind=link}
Conclusions Acute haemodynamic response to LV pacing is useful for predicting which patients are likely to remodel in response to CRT both for DCM and ICM. There is much variation in the rise in LV-dP/dtmax depending on LV lead position. Using acute haemodynamic response measured with a pressure wire during CRT implant has the potential to guide LV lead positioning and improve response rates in the future.
- Cardiac resynchronisation therapy
- acute haemodynamic response
- reverse remodelling