Article Text

Abstract
Objective To assess the cost-effectiveness of dabigatran etexilate, a new oral anticoagulant, versus warfarin and other alternatives for the prevention of stroke and systemic embolism in UK patients with atrial fibrillation (AF).
Methods A Markov model estimated the cost-effectiveness of dabigatran etexilate versus warfarin, aspirin or no therapy. Two patient cohorts with AF (starting age of <80 and ≥80 years) were considered separately, in line with the UK labelled indication. Modelled outcomes over a lifetime horizon included clinical events, quality-adjusted life years (QALYs), total costs and incremental cost-effectiveness ratios (ICERs).
Results Patients treated with dabigatran etexilate experienced fewer ischaemic strokes (3.74 dabigatran etexilate vs 3.97 warfarin) and fewer combined intracranial haemorrhages and haemorrhagic strokes (0.43 dabigatran etexilate vs 0.99 warfarin) per 100 patient-years. Larger differences were observed comparing dabigatran etexilate with aspirin or no therapy. For patients initiating treatment at ages <80 and ≥80 years, the ICERs for dabigatran etexilate were £4831 and £7090/QALY gained versus warfarin with a probability of cost-effectiveness at £20 000/QALY gained of 98% and 63%, respectively. For the patient cohort starting treatment at ages <80 years, the ICER versus aspirin was £3457/QALY gained and dabigatran etexilate was dominant (ie, was less costly and more effective) compared with no therapy. These results were robust in sensitivity analyses.
Conclusions This economic evaluation suggests that the use of dabigatran etexilate as a first-line treatment for the prevention of stroke and systemic embolism is likely to be cost-effective in eligible UK patients with AF.
- Anticoagulation
- Dabigatran etexilate
- warfarin
- stroke
- cost-effectiveness
- atrial fibrillation
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF), the most common clinically significant cardiac arrhythmia, has an estimated diagnosed prevalence of about 1.4% in the UK and is rising.1 2 Patients with AF have a fivefold increased risk of stroke compared with those in sinus rhythm.3 Stroke events result in substantial management and follow-up care, and the incurred costs tend to be higher in stroke patients with AF than those without.3 4 Additionally, AF is associated with an increased risk of non-cranial systemic embolism (SE).5 Despite the substantial clinical risks and economic costs, many patients with AF receive inadequate stroke prevention treatment resulting in a rising burden of stroke in patients with AF in the UK.2 3
One of the principal aims of AF treatment is to avoid thromboembolic events by instituting antithrombotic therapy.3 Vitamin K antagonists such as warfarin may prevent up to 64% of strokes in patients with non-valvular AF.6 However, warfarin treatment is complex; it has many important interactions with food and drugs, requires frequent laboratory monitoring of the international normalised ratio (INR), and has potential to cause serious haemorrhagic events that can be catastrophic.7 8 Due to these concerns, many patients in the UK are under-treated with aspirin or remain untreated. There is a need, therefore, for safer, more efficacious and less complex stroke prevention therapy.3 9
Dabigatran etexilate (dabigatran) is the first new oral anticoagulant to become available for the prevention of stroke and SE in patients with AF in over 50 years.10 It is a reversible direct thrombin inhibitor with stable pharmacokinetic and pharmacodynamic properties and a wide therapeutic margin.11 Unlike warfarin, it does not require INR monitoring or frequent dose adjustments. In the Randomised Evaluation of Long-Term Anticoagulation Therapy (RE-LY) comparative trial, the 150 mg twice daily dose of dabigatran was superior to warfarin in preventing stroke and SE, and the 110 mg twice daily dose was non-inferior (RR vs warfarin 0.65, 95% CI 0.52 to 0.81 for dabigatran 150 mg twice daily; RR 0.90, 95% CI 0.74 to 1.10 for dabigatran 110 mg twice daily). Similar rates of major bleeding occurred with dabigatran 150 mg twice daily and warfarin (RR vs warfarin 0.93, 95% CI 0.81 to 1.07), but the 110 mg twice daily dose had fewer major bleeds (RR vs warfarin 0.80, 95% CI 0.70 to 0.93). The most important haemorrhagic complications associated with anticoagulation therapy (intracranial haemorrhage (ICH) and haemorrhagic stroke) were significantly less likely with both doses of dabigatran compared with warfarin.12 13 Based on the benefits of dabigatran demonstrated in the RE-LY trial, clinical guidelines in Europe and North America now include dabigatran as an alternative to warfarin for stroke prevention in patients with AF.8 10 14
Besides an assessment of relative efficacy and safety, adoption of new treatments is also influenced by cost-effectiveness; the decision whether the added value is worth the added cost. The present study used an economic model to systematically assess the costs and consequences of dabigatran treatment used per its European indication, in which the 150 mg dose is recommended for patients under age 80 and the 110 mg dose for those aged 80 and over. The analyses compare dabigatran with warfarin (with trial-like INR control), aspirin and no treatment. The overall cost-effectiveness of dabigatran was quantified as incremental cost incurred per quality-adjusted year of life (QALY) gained with dabigatran treatment.
Methods
Overview
A Markov model was developed to estimate the cost-effectiveness of dabigatran in eligible patients with AF, which has been described in detail previously.15 16 In brief, the model assumed that patients received dabigatran 150 mg twice daily until age 80 and 110 mg twice daily thereafter (‘sequential dabigatran’), which reflects the intended clinical use of dabigatran based on the approved European label.17 Comparators relevant for the UK setting and evaluated in the model were warfarin treatment, aspirin monotherapy, and no treatment. Patients receiving warfarin were assumed to maintain a level of INR control consistent with that observed in RE-LY (mean of 64% time in therapeutic range), which compares favourably with that observed in routine UK practice.18 19 Therefore it can be regarded that dabigatran was compared to trial-like warfarin in the UK setting.
Model structure
The model followed patients with AF through the natural course of disease in 3-month cycles, included all relevant clinical outcomes and incorporated health states stratified by treatment history, stroke history and disability level.16 Major clinical events included in the model were primary and recurrent strokes (ischaemic (IS) and haemorrhagic (HS)), SE, transient ischaemic attack (TIA), acute myocardial infarction (AMI), ICH excluding HS, major extracranial haemorrhage (ECH), minor bleeding and death. Each event was defined in accordance with clinical definitions from the RE-LY trial.12 13 IS, HS and ICH could be disabling or non-disabling, with disabling events resulting in permanent functional deficits characterised by modified Rankin Score (mRS) for IS, and by Glasgow Outcomes Scale (GOS) for ICH and HS. All haemorrhagic events could result in discontinuation of current treatment. Patients could also discontinue for other, possibly non-clinical, reasons. When patients discontinued anticoagulant therapy, they switched to aspirin. Patients who discontinued aspirin received no further antithrombotic therapy. A model structure outline is presented in figure 1.
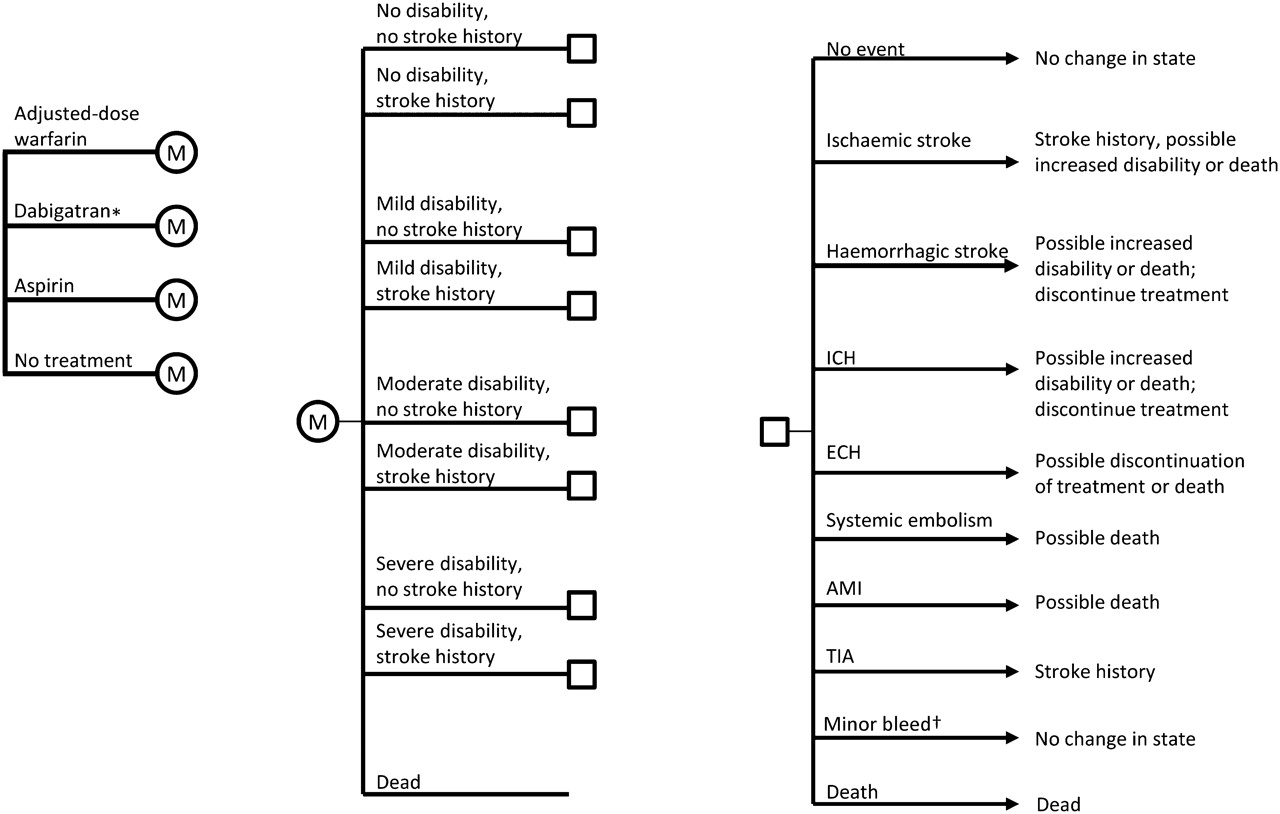
Schematic diagram of the model structure. Patients in each of the four treatment groups in the left figure proceed through the Markov process designated by ‘M’. Patients can be in any of the health states defined by disability and stroke history (illustrated in the middle figure) and by treatment line (not depicted). Patients begin with no disability, but some may have prior history of stroke. All surviving patients can have any of the events noted by the square (right diagram) occurring in a given model cycle, including no event. Based on these events, patients may change their health state (eg, developing stroke history or greater disability) and treatment regimen. Note that ‘stroke history’ refers to history of those events that increase the risk of subsequent stroke as per the CHADS2 score (ie, ischaemic stroke or TIA). *150 mg twice daily for patients <80 years; 110 mg twice daily for patients ≥80 years. †Minor bleeds can occur in any cycle. AMI, acute myocardial infarction; ECH, extracranial haemorrhage; ICH, intracranial haemorrhage; TIA, transient ischaemic attack.
Model outcomes included number of clinical events normalised to 100 patient-years, QALYs, total and disaggregated costs (drug, clinical event and follow-up costs) and incremental cost per QALY gained. QALYs are computed by multiplying the time a patient survives by a weight representing their quality of life during that time, with weights ranging from 1 (perfect health) to 0 (death). Because the consequences of stroke and haemorrhage could be life long, the model assumed a lifetime horizon (up to 100 years of age) in the base case. The model assumed patients not discontinuing remain adherent to antithrombotic treatment, and the relative treatment effect remained constant over time. Patients discontinuing treatment received no further clinical benefit. Future costs and outcomes were discounted at 3.5% per annum.
The intention was that all aspects of the analysis were conducted in line with the principles of the National Institute for Health and Clinical Excellence (NICE) Reference Case wherever possible.20 The model implementation used Microsoft Excel.
Data sources
The primary source of clinical input data was the RE-LY trial,12 13 and an adaptation of a published mixed treatment comparison based on a network meta-analysis to synthesise efficacy and safety data of treatments frequently used in prevention of stroke and SE in patients with AF.21
Baseline characteristics of the patient population in the model matched those randomised to the RE-LY trial. Patients were diagnosed with AF plus at least one additional risk factor for stroke or SE, as defined by the CHADS2 risk stratification scheme, or impaired left ventricular ejection fraction. Patients had CHADS2 scores ranging from 0 to 6. The mean CHADS2 score in RE-LY was 2.1, with roughly two-thirds of patients having a CHADS2 score of 2 or higher. At baseline, approximately 20% of patients had a history of previous stroke or TIA. As a result, the stroke risk profile of included patients aligns with that expected to be observed in UK practice.
Patients were assumed not to be receiving any concomitant anticoagulation medication. The RE-LY population was stratified into those aged <80 years and those aged ≥80 years using a post-hoc subgroup analysis. A sensitivity analysis using the full RE-LY dataset for each dose was also performed.
Utility values for each disability level and utility decrements due to clinical events were taken from published literature.22 23 These parameters have been described in detail previously and are summarised in the online appendix.16
Table 1 summarises drug, event and follow-up costs used in this analysis. Drug costs for warfarin and aspirin were £0.04 and £0.09 per day, respectively, while dabigatran costs were £2.52 per day.24 The average annual cost of INR monitoring for warfarin patients was based on an analysis undertaken by NICE25 in the base case, with a plausible range tested in sensitivity analysis due to regional variation within the UK. Acute management costs following SE, AMI, TIA and ECH were assessed based on National Health Service reference costs.26 Costs for management of minor bleeds were based on the NICE clinical guideline for AF.25 Acute management costs for all other events (IS, ICH and HS) were calculated from a recent study of AF patient data from a UK stroke registry, as were costs for long-term management of disability resulting from IS, ICH or HS.27 All cost inputs were inflated to 2010 when necessary.28
Major cost parameters (2010 prices in £)
Analysis
The base-case analysis compared ‘sequential’ dabigatran to trial-like warfarin, that is, in patients initiating treatment before 80 years of age, who may receive the full treatment sequence, and in patients starting at or after 80 years of age, who receive only the 110 mg twice daily dabigatran dose. Scenario analyses were performed comparing dabigatran with aspirin and with no treatment. Deterministic sensitivity analyses were used to identify key determinants of cost effectiveness by varying parameters individually. Finally, probabilistic sensitivity analyses (PSAs) assessed the uncertainty associated with the cost-effectiveness results by performing 5000 simulations for each comparison in which clinical, cost and utility parameters were simultaneously varied randomly within their statistical distributions, based on their means and 95% CIs. When 95% CIs were not available, standard errors were assumed to be 20% of the mean. For the PSAs, baseline risks of clinical events were assumed to have beta distributions, while RRs were assumed to be log-normally distributed. Event costs and utilities were assumed to have gamma and beta distributions, respectively.
Results
Base-case analyses
Compared with warfarin, patients treated sequentially over their remaining lifetime with dabigatran experienced fewer total ICH and HS (0.43 vs 0.99) and IS (3.74 vs 3.97) events per 100 patient-years, but more ECH (3.88 vs 3.57) and AMI (1.27 vs 1.06) events per 100 patient-years. Predicted number of fatal ICH and HS events was also lower with dabigatran (0.18 vs 0.47), whereas the number of fatal IS events was similar (1.40 vs 1.43). Clinical event differences were found to be somewhat smaller for IS and larger for ICH and HS in patients initiating treatment at age 80 or above. In this population, the dabigatran and warfarin groups experienced similar numbers of IS (4.19 vs 4.13) but total ICH and HS events were more than halved in the dabigatran-treated group (0.58 vs 1.32).
These differences in clinical event rates resulted in an increase in QALYs for dabigatran-treated patients versus warfarin (8.06 vs 7.82). This was accompanied by higher lifetime cost per patient for disease management with dabigatran (£19 645 vs £18 474), due to the higher drug costs (35% of total dabigatran costs vs 17% of total warfarin costs, including INR monitoring). In both treatment groups, follow-up costs represented the largest share of costs (47% for dabigatran vs 61% for warfarin), with the remaining fraction attributed to acute event management. In the scenario analyses, aspirin and no treatment provided fewer QALYs (7.59 and 7.12, respectively) than dabigatran. Aspirin resulted in lower overall costs than dabigatran, but the higher event rate in the no treatment group resulted in higher total management costs, despite the absence of drug costs (£18 561 for aspirin and £20 475 for no treatment). Note that aspirin and no treatment were compared with dabigatran without a second-line treatment (7.99 QALYs and £19 961 management costs). In the population initiating treatment at age 80 or above, total QALYs and costs were reduced (4.11 QALYs and £10 424 management costs for dabigatran vs 4.04 QALYs and £9919 management costs for warfarin). Costs had a similar breakdown of drug, acute event and follow-up costs as the population initiating treatment before age 80.
In the population initiating treatment before age 80, the incremental cost-effectiveness ratio (ICER) was £4831/QALY gained, while in the population initiating treatment at 80 the ICER was £7090/QALY gained. In the scenario analyses which compared initiating dabigatran before age 80 with treatment with aspirin, the ICER was found to be £3457/QALY gained, while dabigatran dominated receiving no thrombophylaxis (ie, more effective and less costly).
Deterministic sensitivity analyses
Deterministic sensitivity analyses for the base-case model showed cost-effectiveness of dabigatran versus warfarin was robust to variations in the majority of parameters, including changes in underlying clinical event rates, costs, utilities and discounting. Key parameters that affected the cost-effectiveness were the degree of INR control attained by patients on warfarin, the RR and overall rates of IS, ICH and HS for dabigatran versus warfarin, the cost of long-term follow-up care for patients with disability, and time horizon analysed (figure 2). Significant differences in the cost of INR monitoring while on warfarin also had an effect on the ICER. To reach a willingness-to-pay threshold of £20 000 and £30 000/QALY gained required an average time in therapeutic range for the whole cohort of approximately 91% and 97% for the population starting therapy at age <80 years, and 80% and 83% in the population starting therapy at age ≥80 years, respectively.

Deterministic sensitivity analysis showing the effect of varying key parameters over a plausible range on incremental cost-effectiveness ratios (ICERs) of dabigatran initiated prior to age 80 versus warfarin. The black bar shows the results with the first parameter variation indicated in the parentheses (eg, the upper CI limit for RR of ischaemic stroke with dabigatran yields an ICER of £13 353/quality-adjusted life year (QALY)), while the grey bar shows the results using the second variation in the parentheses (eg, the lower CI limit for RR of ischaemic stroke with dabigatran yields an ICER of £2124/QALY). The base case ICER is £4831/QALY.
Over a time horizon of only 10 years, the mean survival of the modelled patient population, the ICER was £11 898/QALY gained. Using the upper limit of the 95% CI for the RR of IS, ICH or HS for dabigatran versus warfarin increased the ICERs to £13 353, £10 013 and £8420/QALY gained, respectively. Using full RE-LY clinical results instead of age-stratified results yielded an ICER of £4985/QALY and £13 645/QALY in the <80 and ≥80 populations, respectively.
Probabilistic sensitivity analyses
PSA simulation of dabigatran versus warfarin treatment for patients initiating treatment at age 80 or above showed that dabigatran increased QALYs in all simulation runs, with most, but not all, showing increased costs. Similarly, dabigatran resulted in an increase in QALYs in simulations versus aspirin or no treatment when patients initiated treatment before age 80, and in 82% of simulations versus warfarin when patients initiated treatment at age 80 or above. Figure 3 shows the cost-effectiveness acceptability curves for each scenario analysed. These curves show the fraction of simulations that resulted in cost-effectiveness below a specific willingness-to-pay (WTP) threshold. For example, the probability that dabigatran is cost effective for patients under the age of 80 years at the commonly cited WTP threshold of £20 000/QALY gained was 98% against warfarin, and 100% against aspirin and no treatment. In patients initiating treatment at age 80, the probability of cost-effectiveness versus warfarin was 63% at the same WTP threshold.

{kind=link}
{kind=link}
{kind=link}
Cost-effectiveness acceptability curves showing the fraction of probability sensitivity analysis simulations that yield incremental cost-effectiveness ratios below a specified threshold for dabigatran initiated prior to age 80 versus warfarin (solid black), aspirin (dashed grey), and no treatment (dashed black). Dabigatran initiated after age 80 is also compared with warfarin (solid grey). QALY, quality-adjusted life year.
Discussion
This economic evaluation estimated the cost-effectiveness of dabigatran compared with warfarin, aspirin and no treatment for prevention of stroke and SE in patients with AF. The modelled evaluation estimated that use of dabigatran was likely to be cost effective in all comparisons and analyses conducted. That is, for all comparisons, the ICERs for dabigatran were well below the benchmark WTP threshold of £20 000/QALY gained. The low ICERs for patients receiving dabigatran reflect the significant reduction in catastrophic events (IS, ICH and HS) and the substantial savings that were achieved through the reduction in long-term disability as a consequence. Cost effectiveness for dabigatran treatment versus warfarin was demonstrated for patients initiating treatment at age 80 years despite similar clinical benefit for warfarin and dabigatran treatment in terms of IS. In this population, which receives only the 110 mg twice daily dose of dabigatran, cost-effectiveness is driven specifically by the reduction in ICH and HS and associated reductions in mortality and disability. Deterministic and probabilistic sensitivity analyses showed that these ICERs were robust to uncertainty and variability in the model parameters. It was demonstrated that average population warfarin control would need to be raised to levels not observed in routine practice for £20 000/QALY gained to be exceeded. These consistent cost-effectiveness results are in line with the improved efficacy and safety outcomes demonstrated in RE-LY.
These results are also consistent with analyses in the US29 30 and Canadian settings,16 though, using a higher US dabigatran price, Shah and Gage found low risk subpopulations in which dabigatran was less cost effective. None of the prior analyses presented cost-effectiveness results versus remaining untreated.
Limitations
As with any economic model, results rest on important assumptions. The key modelling assumption is that of continued benefit with ongoing anticoagulation treatment. The decision to anticoagulate patients with AF should be life long; therefore, it was appropriate to model costs and outcomes over the lifetime without arbitrarily truncating the model time horizon, especially as post-stroke disability continues over patients' remaining life. To be conservative (given the higher discontinuation rate with dabigatran versus warfarin), the model included clinical event risks based on the intent-to-treat population, while also explicitly including discontinuation of treatment.
A major driver in the model is cost of long-term disability management. As systematic follow-up of patients in RE-LY suffering an event was limited to 3–6 months, there were limited data available. However, it was possible to stratify stroke outcomes by patient-level data (mRS), and thereby, assign different cost estimates for different disability levels. This should have resulted in more accurate estimates of total costs than assigning overall stroke follow-up costs.31
This model and evaluation offer a number of strengths. Foremost is the use of clinical parameters estimated directly from individual patient-level data in the RE-LY study. Second, the main comparator, warfarin as studied in the RE-LY trial, can be considered as conservative because the INR control observed in routine UK practice is likely to be inferior in comparison. Third, the model allowed the approved stratification of the two dabigatran doses to be reflected in the correct populations. Fourth, it provided the flexibility to investigate the cost effectiveness of dabigatran compared with other treatment strategies provided to UK patients. Finally, the model has been populated with UK-relevant data, and the stroke risk profiles of the patient populations are representative of those that would be expected in UK patients.
Conclusion
In conclusion, treatment with dabigatran reduced the risk of stroke and intracranial haemorrhage compared with warfarin, aspirin and those patients remaining untreated. These clinical benefits offset a substantial portion of the additional drug cost associated with dabigatran, yielding favourable cost-effectiveness ratios well below standard WTP thresholds. Overall, this economic evaluation supports the use of dabigatran as a cost-effective first-line treatment for the prevention of stroke and SE in eligible UK patients with AF.
Key messages
Using data from the Randomised Evaluation of Long-Term Anticoagulation Therapy (RE-LY) trial, and relevant UK costs and resource use, this analysis suggests that the use of dabigatran as a first-line treatment for the prevention of stroke and systemic embolism is likely to be cost-effective in eligible UK patients with atrial fibrillation compared with well controlled warfarin, and ‘dominant’ (less costly and more effective) compared with no therapy.
Acknowledgments
The authors would like to thank Brigitta Monz, Boehringer Ingelheim, for her contribution in drafting and reviewing the manuscript and providing comments, and Siyang Peng, United BioSource Corporation, for assistance in building the model and performing analyses. The authors would like to further acknowledge Greg Y Lip for providing recommendations on the adaptation of the model to the UK setting.
References
Footnotes
Funding Boehringer Ingelheim provided the funding for the health economists to perform the analyses required.
Competing interests This project was funded by Boehringer Ingelheim International GmbH (BI). AK, SS and FP were paid consultants to BI for this project. MC reports receiving a consultancy fee from BI. RG and PR are employees of BI UK Ltd at the time of the study. JP was an employee of BI GmbH.
Ethics approval Health economic modeling based on data from the RE-LY trial (which was ethics committee approved) and data from published UK resources.
Provenance and peer review Not commissioned; externally peer reviewed.