Article Text

Abstract
Background The effectiveness of salt restriction to lower blood pressure (BP) in Bangladeshi patients with chronic kidney disease (CKD) is uncertain.
Objective To test the hypothesis that a tailored intervention intended to reduce salt intake in addition to standard care will achieve a greater reduction in BP in UK Bangladeshi patients with CKD than standard care alone.
Design A randomised parallel-group controlled trial conducted over a 6 month period.
Setting A tertiary renal unit based in acute care hospital in East London.
Participants 56 adult participants of Bangladeshi origin with CKD and BP >130/80 mm Hg or on antihypertensive medication.
Intervention Participants were randomly allocated to receive a tailored low-salt diet or the standard low-salt advice. BP medication, physical activity and weight were monitored.
Main outcome measures The primary outcome was change in ambulatory BP. Adherence to dietary advice was assessed by measurement of 24 h urinary salt excretion.
Results Of 56 participants randomised, six withdrew at the start of the study. During the study, one intervention group participant died, one control group participant moved to Bangladesh. Data were available for the primary endpoint on 48 participants. Compared with control group the intervention urinary sodium excretion fell from 260 mmol/d to 103 mmol/d (−131 to −76, p<0.001) at 6 months and resulted in mean (95% CI) falls in 24 h systolic/diastolic BP of −8 mm Hg (−11 to −5)/2 (−4 to −2) both p<0.001.
Conclusions A tailored intervention can achieve moderate salt restriction in patients with CKD, resulting in clinically meaningful falls in BP independent of hypertensive medication.
Trial Registration ClinicalTrials.gov NCT00702312.
- Renal Disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Chronic kidney disease (CKD) prevalence is three to five times higher in the Bangladeshi population compared with other ethnic groups in the UK.1 Hypertension is the cause and consequence of CKD2 and extracellular volume expansion is an important factor in the development and maintenance of hypertension in patients with CKD.3 The British Bangladeshi population has an unusually high salt intake, twice that of the general population, which might contribute to CKD and hypertension.4 An intake of less than 6 g salt/d (∼100 mmol Na/d)5 is advised in the UK and Europe based on the association of salt intake with blood pressure (BP) and cardiovascular disease rather than the much lower intake required to prevent sodium deficiency. However, even greater restrictions to below 60 mmol Na/d have been proposed in NICE guidelines. Nevertheless, a recent systematic review suggested an adverse effect of intakes as low as 3.5 g/d.6 Meta-analyses of salt restriction studies show a greater BP lowering effect of salt restriction in hypertensive compared with normotensive subjects; under optimal conditions reductions in systolic/diastolic BP of 7/4 mm Hg7 can be obtained with salt intake reduced to 100 mmol/d. Patients with resistant hypertension, defined as BP that remains above target despite the use of three or more antihypertensive medications,8 are thought to be salt sensitive.9 However, adherence to dietary advice is often poor resulting in smaller changes (<1mm Hg) in BP of dubious clinical value. In previous work we investigated barriers to dietary salt restriction in Bangladeshi patients with CKD in East London10 and developed a strategy intended to reduce salt intake in these patients. This present study set out to test the hypothesis that a low-salt educational intervention tailored to meet the needs, customs and practices of this population in addition to standard hypertension medication management would result in greater BP reduction than standard care alone: a first such intervention with this population group.
Methods
A parallel-group randomised trial design was selected, and conducted between June 2008 and July 2009. Ethical approval was obtained from the relevant research ethics committee.
Participants were patients with established moderate–severe CKD of Bangladeshi origin residing in East London, UK. Inclusion criteria were estimated glomerular filtration rate (eGFR) <60 mL/min and mean BP >130/80 mm Hg on at least two clinic visits or taking antihypertensive medication. Patients on dialysis, those with a body mass index <20 or >35 kg/m2, urinary incontinence, or cognitive impairment or mental problems impairing their ability to participate were excluded.
Participants were recruited at the predialysis clinic of a tertiary renal unit in London by the researcher. Randomisation to treatment was conducted by the study statistician using computer-generated random blocks with block sizes between four and eight and the group assignment given to the researcher. This was a dietary behaviour intervention, thus, neither participants nor the dietitian administering the intervention could be blinded to treatment allocation. Data analysis was conducted by the study statistician who was blinded to treatment allocation.
Intervention
The intervention group was initially advised by the study dietitian at the hospital clinic followed by practical cooking and educational sessions in the community facilitated by Bengali workers and attended by the researcher (see online supplementary file). Community cooking sessions were delivered in conjunction with Community Kitchen UK.11 In the community sessions, intervention participants cooked two versions of their traditional meals: one followed their usual recipe, the other had salt reduced by 50%. Fortnightly telephone calls from a Bengali worker followed, to reinforce advice and set new targets. The control group received usual care from the renal clinic in the form of a low sodium general dietary advice sheet sent by post with the physician's letter. This had not been specifically adapted for Bangladeshi diets.
Data collection
Data collected at enrolment included age, sex, medication use and comorbidities, including diabetes mellitus. Data collection for the primary outcome was by ambulatory BP measured using TM-2430-13 devices (A&D Medical, Milpitas, California, USA; graded A/A by the British Hypertension Society) and Doctor Pro software, in accordance with recommendations.12 Daytime measurements were taken at 30 min intervals, night-time measurements every 60 min. Height, weight and body composition (total body water) were measured using the Fresenius Medical Care D GmbH Body Composition Monitor; blood samples were obtained for glycosylated haemoglobin (HbA1c). Physical activity levels were recorded using the YamaxDigi-Walker SW-200 (Yamax Corporation, Tokyo, Japan) pedometer, shown to have an overall mean absolute error of 3% for outdoor normal walking.13 The accuracy of the pedometer on each participant was checked by a 20-step test at the outset, with an acceptance criterion of ±2 steps.13 Data were collected at two time points, at baseline and at end of study—6 months later.
Outcomes
The primary outcome was reduction in systolic BP (SBP) determined by 24 h ambulatory monitoring. Secondary outcomes were changes in diastolic BP and reduction in eGFR. Measurement of 24 h urinary sodium, potassium and creatine were undertaken using routine methods at baseline and follow-up as indices of adherence to the intervention and determined by assessors blinded to treatment allocation.
Statistical analysis
Sample size calculations were based on a sample of 25 participants per group giving 80% power to detect a significant reduction in the mean SBP of 8 mm Hg at p<0.05 between the two groups (which was regarded as clinically relevant difference), assuming a SD of 10 mm Hg.14 Sample size was increased to 26 per group to allow for non-compliance or dropout. Analyses were conducted on an intention-to-treat basis. Changes within groups between baseline and follow-up at 6 months were compared using analysis of covariance and results are expressed as mean values with 95% CIs using Stata V.10 (StataCorp LP, Texas, USA).
Results
Participant recruitment and progress through the trial is shown in figure 1. Of the 56 participants recruited six withdrew; three cited the inconvenience of 24 h urine collection, two were unwilling to undergo ambulatory BP monitoring and one was unwilling to attend the community cooking activity. One intervention group participant died; one control group member relocated to Bangladesh. Data were available for 48 participants. Details are shown in table 1; groups were well-matched including for antihypertensive medication, with most receiving ACE inhibitor or angiotensin-receptor blocking medicines and diuretics.
Baseline characteristics for the intervention and control groups

CONSORT flow chart of participant recruitment, allocation and assessment.
Adherence to the dietary intervention
All participants attended the initial briefing session with the study dietitian. Male participants attended with their wives, daughters or sisters while female participants attended with their daughters or daughters-in-law. Participants were split into four groups of six or seven to attend the community cooking sessions; each group was to attend two weekly consecutive sessions. Male participants chose not to attend but sent a female representative; a wife, daughter or sister for single men. The first weekly session was attended by 88% (23/25) of the participants or representatives; the second and final session was attended by 84% (21/25). Overall, all participants attended at least one cooking session.
Adherence to dietary salt recommendations was indicated by urinary sodium excretion. At baseline urinary sodium excretion was approximately 260 mmol/24 h in both groups (figure 2). After 6 months, this had reduced by 122 mmol/24 h (95% CI −140 to −105, p<0.001) in the intervention group, and by 13 mmol/24 h (95% CI −18 to −8, p<0.001) in the control group. At follow-up sodium excretion differed significantly between groups, by 103 mmol (95% CI −131 to −76, p<0.001).

24 h urinary sodium excretion for intervention and control groups is shown as the mean difference with 95% CI in parenthesis. All differences are p<0.001. Control n=23, Intervention n=25.
Primary and secondary outcomes
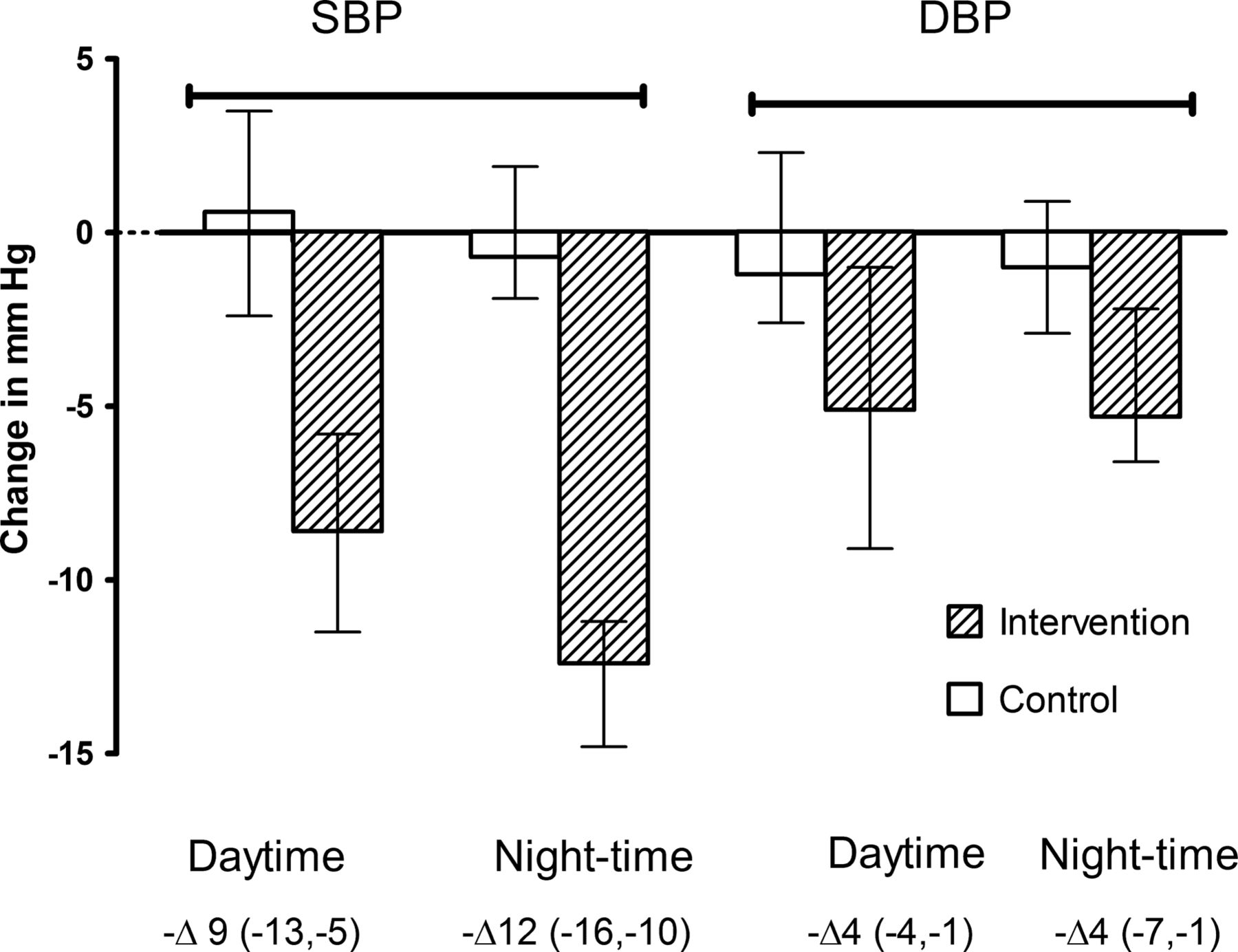
Systolic BP was elevated in both groups at baseline but fell by 8 mm Hg (95% CI 5 to 11, p=0.0003) on tailored intervention compared with the usual care group. Figure 3 shows the significant (p<0.001) falls in daytime and night systolic and diastolic BP in the intervention group compared with the control group. Non-dipping, that is loss of the normal nocturnal reduction in night-time SBP, with a difference >10 mmHg between night-time and daytime SBP, was observed in 60% (15/25) of the intervention group and 56% (13/23) of the control group at baseline. At follow-up this reduced by 40% (6/25; p=0.02) in the intervention group but remained unchanged in the control group.
{kind=link}
{kind=link}
{kind=link}
Changes in daytime and night-time systolic blood pressure (SBP) and diastolic blood pressure (DBP). Mean values and changes with 95% CI. All differences are p<0.001. Control n=23, Intervention n=25.
The observed changes in eGFR from baseline to follow-up were similar for both groups. An eGFR decline of 3.0 (95% CI 0.1 to 6.0) and 3.4 (95% CI 1.0 to 5.7) mL/min per 1.73 m2 were observed in the intervention and control groups respectively.
Covariate findings
Potassium excretion was low (40 mmol/d) in both groups and unchanged at follow-up. Physical activity levels were low in both groups and remained unchanged during the study. Glycosylated haemoglobin concentrations remained elevated at >8.0%, indicating poor but unchanging diabetic control in both groups. Body weight did not change in either group, but there was a modest but statistically significant reduction in mean total body water in the intervention group (0.50 L, p<0.01) compared with no change in the control group (0.26 L, not statistically significant.).
Discussion
Dietary advice to lower salt intake is routinely given to patients with CKD in the form of an information sheet; this study suggests this is ineffective at changing behaviour. By contrast, the dietitian-led intervention which identified the sources of salt in the Bangladeshi diet and developed strategies to lower intake, achieved a reduction in dietary salt intake of over 100 mmol/d. While mean urinary sodium excretion still remained well above the UK target of 100 mmol/day,15 postintervention group results were more similar to those seen in the UK white population. This reduction in salt intake led to a highly significant fall of 8/3 mm Hg in BP; very close to the figure predicted by meta-analyses.7
The dietary approach used has also been shown to be effective in BP reduction with other ethnic groups with high dietary salt intakes.16 Behavioural intervention studies have previously demonstrated that knowledge is a key contributing factor to adherence to low-salt diet14 and that lack of knowledge is a key barrier in dietary modification and adherence.17 ,18 However, knowledge of the need to reduce dietary salt intake is not always enough to ensure dietary modification and adherence. This study shows that knowledge tailored to recipients’ needs and contexts, delivered in a practical and acceptable manner, can effect behavioural change and achieve health benefits.
Our previous studies showed that Bangladeshi patients with CKD have much higher intakes of salt than the general population, with much of the salt being added during home preparation of food rather than during processing, as is the case in the general population. Consequently, routine advice for salt reduction designed for predominantly white European populations was not appropriate for this group of patients, for whom the engagement of family members was crucial. This was particularly relevant for these study participants, who almost exclusively ate home-prepared meals in family groups.
We noted that over half of the Bangladeshi patients with CKD had raised BP throughout the day and night: the ‘non-dipping’ effect. Previously ‘non-dipping’ prevalence has been found to increase with worsening CKD, with 15% of normal subjects affected increasing to 75% in those with stage five CKD.19 Non-dipping has been associated with increased target-organ damage (heart, brain, kidney),20–22 raised frequency of stroke and myocardial infarction,23 and higher cardiovascular mortality.22 Decreased salt intake and urinary sodium excretion led to greater reduction in night-time SBP compared with daytime, and the restoration of the normal physiological night-time dip in BP in many patients. In black salt-sensitive patients with hypertension salt restriction improved the circadian rhythm of BP with a return to dipping pattern.24 Our study confirmed that salt reduction can change the pattern from ‘non-dipper’ to ‘dipper’, and a recent review has concluded that the South Asian population is salt sensitive.25 A return to a ‘dipping’ BP pattern may lead to a significant reduction in the risk of vascular events for this patient group but long-term follow-up is required to demonstrate this.
Comparison with other studies
Data supporting our findings were reported by MacGregor et al,26 who demonstrated that when urinary sodium excretion dropped by 100 mmol/24 h, subjects supine BP declined by 8/5 mm Hg (p<0.01); a sodium reduction of 150 mmol/24 h led to a larger decline of 16/9 mm Hg. Similarly, a modest salt reduction of 50 mmol/24 h (from a much lower baseline than in our participants: an average of 177 mmol/24 h) resulted in 7/3 mm Hg drop in BP in a randomised trial in older people.27 A recent meta-analysis of 17 trials in hypertensive individuals over ≥4 weeks supports the approximate magnitude of this effect.7 A recent study of modest dietary sodium restriction in patients receiving ACE medicines showed 11mm Hg reduction in SBP in non-diabetic nephropathy.28 Our study confirms this magnitude of association between reduction in sodium excretion and BP values. Moreover, our study is the first study to our knowledge of a population with CKD with traditionally high salt intake and hypertension with a follow-up period of 6 months suggestive of sustained benefit in the tailored intervention approach.
Strengths and limitations
The strength of this study is that it delivered an effective salt reduction dietary intervention for this group of patients, and demonstrated participants’ adherence to dietary advice through 24 h urinary sodium excretion. However, only single 24 h urine collections and 24 h ambulatory BP recordings were made. Further, treatment allocation could not be blinded. Therefore, ambulatory BP readings were analysed centrally in the hypertension unit by a statistician who was blinded to the treatment allocation. Hence the results were relatively less likely subject to bias. It remains uncertain whether reducing BP may translate into slowing of disease progression or reduction in cardiovascular events.
Applicability and generalisability
The Bangladeshi population and indeed the South Asian group are known for a high dietary salt intake, are at a high risk of CKD and thus, hypertension development. Dietary salt reduction can safely and usefully be extended to other family members who may in time also be at risk of developing hypertension. Other ethnic groups with a high prevalence of CKD and hypertension, such as black African and Afro-Caribbean populations, may also benefit from tailored dietary interventions to reduce salt intake.
Conclusion
This study demonstrates the importance of tailoring dietary advice to patients’ contexts, cultures and needs, particularly for minority and high-risk groups. Healthcare professionals need education and training in methods to enable them to translate generic principles of healthy living and health promotion in such a way as to successfully deliver education and promote its application in the daily lives of their patients. Policy makers need to recognise the importance of resourcing complementary approaches to medication for effective BP control. An integrated approach, drawing on multiple successful approaches to hypertension reduction, offers the best option for BP management in patients with CKD.
Acknowledgments
This is an original work that has not been published before and is not under consideration in any other journal. IdeB-A would also like to thank Nadia Pendleton, food writer director of community kitchen UK, for the training and support on conducting the practical educational sessions in the community. Finally, this study was funded by Barts and The London Charitable Foundation. IdeB-A, the recipient of this Fellowship award, would like to thank this organisation for their financial support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors IdeB-A, researcher, designed the study and data collection tools, conducted educational intervention, collected data for the whole trial, drafted and revised the paper. MV, statistician, wrote the statistical analysis plan, analysed the data, drafted and revised the paper. MMY, LP, HD, TABS and JET were supervisors. The supervisors contributed to the design of the study and data collection tools, monitored data collection for the whole trial, drafted and revised the paper.
-
Funding This research was funded by a PhD fellowship grant made to IdeB-A from the trustees of Barts and The London Charitable Foundation. The analysis, interpretation of data, generation of the manuscript and decision to submit for publication were carried out independently of the funding body.
-
Competing interests All authors declare that for this submitted work: IdeB-A received salary support from a grant made to Barts and The London NHS Trust by the trustees of Barts and The London Charitable Foundation.
-
Ethics approval East London & The City Research Ethics Committee 3.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The original article was prepared from a database established by the corresponding author and it is accessible to all listed authors. This database remains the intellectual property of Barts and The London NHS Trust, but confidential data sharing agreements may be entered into to address any questions in relation to the trial. All data relevant to this author are presented here.