Article Text

Abstract
Africa has one of the highest prevalence of heart diseases in children and young adults, including congenital heart disease (CHD) and rheumatic heart disease (RHD). We present here an extensive review of recent data from the African continent highlighting key studies and information regarding progress in CHD and RHD since 2005. Main findings include evidence that the CHD burden is underestimated mainly due to the poor outcome of African children with CHD. The interest in primary prevention for RHD has been recently re-emphasised, and new data are available regarding echocardiographic screening for subclinical RHD and initiation of secondary prevention. There is an urgent need for comprehensive service frameworks to improve access and level of care and services for patients, educational programmes to reinforce the importance of prevention and early diagnosis and a relevant research agenda focusing on the African context.
- CONGENITAL HEART DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
The epidemiological patterns of heart disease differ greatly between developed nations and sub-Saharan countries, where rheumatic heart disease (RHD) remains a public health issue while congenital heart disease (CHD) bears a poor prognosis. The huge strides made in the developed regions of the world in diagnostic options, and surgical and interventional management of complex CHD have not been replicated in Africa.1 ,2 Yet a number of important centres and collaborations have evolved over the past decade in order to address these disparities and renewed attention has been focused on early detection and management of CHD while encouraging innovative approaches and training centres of excellence.1–5
In Africa, RHD has demonstrated a particular prevalence in the younger African population.6 Since 2006, efforts from affected nations in Africa have resulted in the launch of control and prevention initiatives such as the Drakensberg Declaration and in an invigorated research agenda which has focused attention on echocardiographic screening for RHD leading to the concept of ‘subclinical’ RHD, and on contemporary trends in management and outcome of patients with tertiary RHD from all over the continent.7–9
Burden of CHD in Africa
The birth prevalence of CHD is thought to be relatively similar the world over, with variations between regions and countries due to genetic, environmental and epigenetic differences.10 The estimate of ∼8 per 1000 live births is generally accepted as the most reliable, however a recent systematic review emphasised potential significant differences, with the lowest prevalence rate observed in Africa, particularly among lowest-income populations.11 This mainly reflects the paucity of readily available estimates and the urgent need for robust data to support burden of disease calculations in Africa. Given the reductions in under-5 years mortality (albeit less than in developed countries), and coupled with the projected increase in the proportion of African people in the world over the next decades, the number of children and adults affected with CHD in Africa may be vastly underestimated.
Several recent publications have profiled the epidemiology of CHD in children and adults in Africa, emphasising the burden of CHD among patients referred with suspected heart disease.12–14 Among children and adults with suspected heart disease the prevalence appears to be dramatically much higher according to recent data from Sudan.15 In Cameroon, 13.1% of patients with suspected cardiac pathologies, aged between 2 months and 41 years (mean age 10±9 years), during a 4-year study period, were diagnosed with CHD.16 A survey conducted in Mozambique provided an opportunity to assess the prevalence of CHD in the general population of public school children in Maputo.17 Five children (out of 2170) had CHD giving a prevalence of 2.3 in 1000 of which 80% were newly discovered.
Data from northern Nigeria reported that among 1312 patients (aged 9 days to 35 years) with abnormal echocardiograms, 122 (9.3%) had CHD.18 The predominant lesions noted were ventricular septal defect and among cyanotic lesions, tetralogy of Fallot. However critical congenital heart defects such as left-sided obstructive lesions were rare, suggesting the poor survival of affected children, and the likelihood that the data available underestimate the true prevalence of CHD.
Children with CHD in Africa have a dramatically different prognosis to those living in developed nations, in terms of morbidity and mortality.1 The impact of CHD on admissions for heart failure has been established in southwestern Uganda.19 The aetiology of heart failure in this cohort of children (n=58) was largely due to CHD (35%) compared with acquired heart diseases, establishing the importance of CHD as a cause of heart failure among children in Africa.16 ,20 A recent review of the profile of CHD in newborns in Bizerte, Tunisia, a middle-income country, revealed that medical treatment was indicated in 46.3% and surgery in 22.5% of patients with a very high case-fatality rate of 23.8% over a 9-year period.21 The limited access to surgical programmes means a long waiting list, in particular when the only access to surgery requires sending children abroad for treatment. While early postoperative mortality in children deemed fit for surgery may be as low as 4%,1 the long-term outcome of children sent abroad for surgery is associated with a high mortality rate (18.8%) in part related to the delay prior to definitive treatment.22 Yet, the majority of congenital cardiac lesions are simple and potentially correctable with suitable medical and surgical facilities. Instead, children living with these lesions in many parts of Africa will die in early teens or adulthood from the long-term effects of cyanosis, pulmonary hypertension and cardiac failure.2
Burden of RHD in Africa
RHD remains the leading cause of acquired heart disease among the young worldwide.23 The condition results from repeated acute rheumatic fever (ARF) attacks following exposure to Group A streptococci (GAS) infections. The incidence of ARF has remained particularly challenging to assess accurately and thus, no prospective population-based studies of the incidence of first attack of ARF from Africa is available to date. No reports were included in recent systematic reviews.24 ,25 Incidence may be extrapolated from the median incidence from Middle East and North Africa, estimated to approximately 13–14 cases per 100 000 and per year.24 Even without considering the existence of atypical or asymptomatic forms of GAS autoimmune reaction, these data are probably a gross underestimation of the reality in Africa.
It has been projected that more than 15 million people suffer from RHD worldwide,21 ,24 which is likely a significant underestimation according to the increasing data on subclinical RHD.26 Historically, sub-Saharan Africa has had the greatest prevalence of clinically detected RHD, ranging from less than 1 to 14 per 1000.8 ,23 ,27 ,28 It has emerged that previous studies may have markedly underestimated the prevalence of the disease, and recent data suggest that other regions may also present an even higher burden of disease.23 ,29 ,30 Since the first report of echocardiography as a potential screening tool,31 surveys were carried out in Mozambique, and subsequently in Uganda and in Senegal.8 ,27 ,32 ,33 All these studies demonstrated that echocardiography detects a significant additional number of children with clinically silent RHD, estimated to 7.5–51.6 per 1000 children (figure 1).
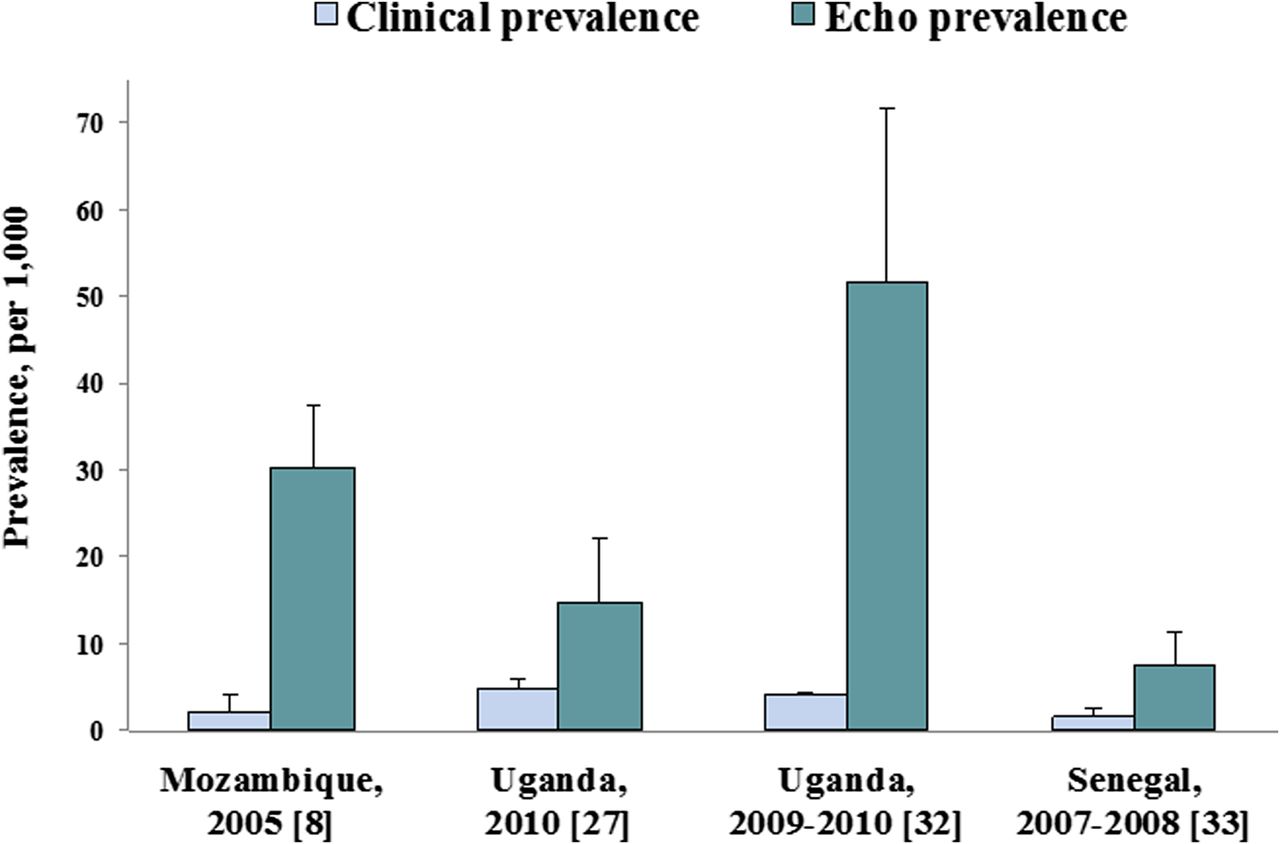
Schoolchildren echo-based screening, Africa 2000–2010. Clinical versus echocardiography (probable and definite lesions) approaches.
It has been calculated that if 1.5% of people with RHD die each year, the approximate number of deaths due to RHD would range from 233 000 to 294 000 per year worldwide.24 However, the exact mortality rate due to RHD is most probably dramatically underestimated in Africa. A large multinational African study demonstrated that RHD prevails as the most frequent cause of heart failure among children and young adults, and importantly that the 180-day mortality is as high as 17.8%.34 In rural Ethiopia annual mortality rate reaches 12.5% among patients with RHD.35 And as many as 70% of such patients die under 26 years of age.36
The recently published Global Burden of Disease Study reports that the number of years lived with disability due to RHD was estimated in 2010 at 1430 (944–2067) worldwide, a figure that represents up to a fourth of all neoplasms.37 Further data are needed to assess the social and economic impact of RHD in sub-Saharan countries. Sensibly, RHD should bear high morbidity due the scarcity of prevention programmes across most sub-Saharan countries, which may strongly impact on social, educational and economic issues. Hospital-based studies recently reported that RHD accounts for 6.6–34.0% of cardiovascular disease-related hospital admissions or echocardiographic examinations performed in institutions across Africa.16 ,38–42 RHD has been documented to be relatively frequent among pregnant women (up to 2.3%), although symptomatic forms remains more rarely encountered.43 Furthermore, recent data emphasise that pregnancy in patients with RHD remains a challenge bearing high morbidity and mortality, requiring multidisciplinary antenatal and postnatal care.44
Importance and challenges of early diagnosis
In congenital heart disease
In Africa, the vast majority of congenital cardiac lesions are not diagnosed prior to birth, due to severely limited antenatal screening for CHD. Early diagnosis of simple lesions can result in timely referral before onset of permanent sequelae yet remains hampered by limited resources. However, recent data reveal improved access to diagnostic services in several parts of Africa. Diagnostic and curative services are being offered in Kenya in the capital cities of Nairobi and Mombasa, while rural communities are being accessed using different models of outreach.45 In an integrated clinic in Kisumu, 400 km west of Nairobi, the most common diagnosis is CHD with the result that early detection and timely referral of CHD is a specific focus of outreach clinics.46 Pulse oximetry screening for critical CHD is now recommended in the USA and has been adopted in many parts of the developed world.47 While potentially exciting, it is critical that newborn screening in Africa be integrated into existing programmes to identify, manage and treat CHD, rather than creating new vertical programmes.
In rheumatic heart disease
Although echocardiography may prove a valuable tool in detecting RHD cases at an early stage, fundamental issues remain to be addressed.48–51 Echocardiographic detection of morphologically abnormal valves or significant valvular regurgitation does not guarantee later progression to advanced valvular disease, nor has the clinical effectiveness of secondary prophylaxis in this population been proven. A first step towards the assessment of subclinical RHD has been taken through the standardisation of echocardiography criteria under the auspices of the World Heart Federation.26 However, if this newly described entity is proven to impact on prognosis, easier ways of detecting the disease may be needed in the field.52 Indeed, differences in echo criteria may impact on the case detection rates, making echo-based screening particularly challenging.53 The ideal screening age is also still unclear. Recent data from Dakar emphasised that adolescents in their late teens should be considered suitable for screening in the light of the higher prevalence of the disease, and the clearer cardiac lesions.33 Currently, echo-based screening remains a research tool with several unanswered questions with experts agreeing that antibiotic prophylaxis should be initiated in cases of definite subclinical RHD.51 ,54
Primary and secondary prevention for RHD: integration into specific African programmes
Prevention for RHD includes: (1) improvement of socioeconomic conditions with better hygiene and housing (i.e. primordial prevention); (2) primary prevention through antibiotic treatment of GAS pharyngitis; and (3) secondary prevention of ARF recurrence by penicillin prophylaxis against repeated or chronic ARF attacks. To date, only South Africa has a national guideline for RHD prevention on the continent (table 1).23 ,55
Available recommendations for secondary prophylaxis for rheumatic heart disease (RHD)
Penicillin, a low-cost drug, is the cornerstone to the treatment of RHD since it prevents the advent of ARF and its recurrence. Emphasis should thus be made on the prevention of the disease through comprehensive register-based programmes in order to deliver penicillin for primary and secondary prophylaxis. Safe administration of penicillin is still an issue in many resource-deprived settings and should become a priority in primary care facilities.
To date, primary prevention alone has often been neglected as a large scale strategy in developing countries.59 A systematic review on primary prevention showed an overall benefit by preventing 1 ARF case for 53 sore throats treated,60 confirmed by the meta-analysis of Lennon et al.61 However, these results remain somewhat controversial largely due to the fact that a controlled randomised trial recently failed to demonstrate any benefit of prophylaxis in this setting.62 However, by contrast with the previous reports, this last trial refers to a strategy of active ascertainment of pharyngitis in a school system followed by treatment with oral penicillin. Two main arguments have been raised against primary prophylaxis: asymptomatic throat infection, and the possibility of other sites of pathogenic infection (such as skin).63 In the African context, there is no available evidence that would favour skin infection in the genesis of ARF. On the other hand, approximately 18% of schoolchildren are asymptomatic GAS carriers in Ethiopia and may be at risk of developing the classical pharyngitis-ARF pathway.64 Experts agree however that primary prophylaxis in developing countries should be based on primary healthcare and cannot rely on the availability of microbiological diagnosis. Clinical scores helping to predict GAS infection had failed in the past,65 ,66 and systematic treatment of sore throat without bacteriological tests have to be advocated in sub-Saharan countries. A better understanding of reasons behind the difficulty of primary prevention has been recently carried out in Tanzania, emphasising the negligence of patients and also medical staff regarding the importance of consulting and treating sore throats.67
Vaccine development is the main promise for primary prevention. Most developments have unfortunately targeted strains prevalent in other regions (North America, Europe and Australia), whereas recent African data emphasised the high diversity of GAS emm types among healthy schoolchildren in Ethiopia.68 Although research in vaccines using highly conserved antigens and 30-valent N-terminal region remains active,69–71 no vaccine is scheduled for phase 2 clinical trials in the foreseeable future. The high heritability and ongoing research on genetic susceptibility may be particularly helpful for a better understanding of the pathogenesis of ARF and may guide vaccine development.72
Duration of secondary prophylaxis depends on several factors most important of which is the presence and severity of RHD and the risk of recurrence, suggesting the need for lifelong prophylaxis in the presence of severe RHD or previous heart valve surgery beyond childhood.23 Poor compliance has been the principal issue in relatively well-funded programmes.73 Compliance with prophylactic benzathine penicillin appears even lower in the African context, being only of 37.5% after 3 months in Congo.28 This particularly low compliance has mainly been reported to be associated with the target population's mobility, understaffing and remote settings.
To the best of our knowledge, there is very scarce data on the cost-effectiveness of prevention in Africa. The principal study evaluated primary prevention—the cost per ARF episode prevented has been estimated at US$46 in South Africa.60 Secondary prophylaxis is thought to be the most cost-effective of interventions, but this has not been verified in any recent African study. Irlam et al have recently assessed the cost-effectiveness of primary prophylaxis by a single penicillin injection for pharyngitis in urban South Africa,74 and favour the use of a clinical score to guide treatment.75 However, these results may not apply to many sub-Saharan countries with markedly lower per capita Gross domestic product than South Africa.
Up to the 2000s, relatively little progress has been made towards achieving the implementation of a comprehensive programme for the secondary prevention of ARF/RHD in Africa. In 2005, African medical practitioners subscribed to the Drakensberg declaration on prevention and control of RHD in Africa.7 Known as the Awareness Surveillance Advocacy Prevention project, it calls for a comprehensive strategy based on the pillars of awareness-raising, surveillance, advocacy and prevention to be applied in all African countries. In 2012, the (hospital-based) Rheumatic Heart Disease Global Registry (REMEDY) is the first attempt at comprehensive characterisation of RHD in countries where it is most prevalent.9 The aims are to collect detailed data on clinical and echocardiographic features at presentation and follow-up and meticulously document clinical and echocardiographic progression of disease and the occurrence of disease-related adverse events during the course of the study.9
Innovations, advances and locally-appropriate management in severe CHD and RHD
Although the percutaneous approach is now the standard approach for definitive correction of defects such as patent ductus arteriosus and valvular pulmonary stenosis, the lack of cardiac catheterisation laboratories has precluded this being introduced into routine clinical practice in many African countries. A recent report from Rwanda however, demonstrated the innovative use of a monoplane conventional C-arm x-ray system and portable ultrasound machine in order to complete several diagnostic and interventional procedures, including closure of atrial septal defects, patent ductus arteriosus and ballooning of valvular pulmonary stenosis.4 This has demonstrated the possibility of performing cardiac interventions on children safely and effectively in under-resourced environments with excellent results. Programmes such as these should be strongly encouraged, and expanded to other countries to provide critical services for patients with simple congenital cardiac lesions that can be corrected at a reasonable cost.
The late presentation of CHD presents special challenges, which is unique to the developing country situation, and the need for a structured management pathway.76 ,77 It is also apparent from countries with long-established cardiac surgical programmes that increased survival in childhood will lead to an increasing number of patients with grown-up CHD.78 In the past decade, there have been major advances in highly technical and expensive catheter interventions for complex CHD such as percutaneous valve replacements, occluders, stents and balloons, and complex hybrid procedures.79 These techniques have been successfully introduced to Africa in certain tertiary and quaternary centres.80–83 However it is important to note that these interventions are restricted to complex CHD, which is the minority of lesions detected, and to specific centres in South Africa, Egypt and Sudan. These innovations however provide opportunities to develop crucial expertise and serves as an important source of centres of excellence for the whole of Africa. Contextualising interventions in terms of local needs and resources should be integral to the choice of surgery and intervention, especially in view of the vast differences in healthcare funding. Unique African challenges such as malnutrition and poor follow-up initially resulted in a preponderance of palliative procedures, however with review; the benefits of definitive repair are obvious.84
Medical and surgical care for people with severe RHD is the least cost-effective intervention and consumes the vast majority of funds available for RHD control in endemic regions.85 Sadly, RHD diagnosis in Africa is usually established at an advanced stage of the disease, when severe valve lesions become symptomatic, and significant intervention is indicated.2 However, percutaneous mitral dilatation, closed heart mitral commissurotomy and open heart surgery are limited to a few centres in Africa.
Percutaneous mitral balloon commissurotomy has replaced surgical commissurotomy over the past two decades as the treatment of choice for significant mitral stenosis and yields excellent outcomes.6 It has been recently demonstrated that clinical presentation of mitral stenosis significantly varies across the world with particularly young and severe patients in Africa.86 Recent data from Egypt also suggest that redo mitral balloon commissurotomy for mitral restenosis is feasible and safe, and achieves immediate and long-term outcome comparable with initial mitral balloon commissurotomy.87
In patients requiring heart surgery, valvuloplasty is always attempted, even at the risk of suboptimal results, owing to its advantages in avoidance of anticoagulation, and thus allowance for pregnancies. Valve replacement presents a dilemma due to the generalised lack of adequate facilities for anticoagulation. Recent experience from Senegal evaluated the mid-term outcome of mitral valve repair in children, demonstrating encouraging results, dependent on careful patient selection and evaluation of lesions.88 Findings from South Africa confirm superior long-term outcome in patients who underwent mitral valve repair while also demonstrating reasonable long-term results for mitral valve replacement in an indigent population.89
The African health workforce crisis: a major barrier to CHD and RHD management in Africa
Sub-Saharan Africa carries over 24% of the global disease burden but is home to only 3% of the global health workforce, in sharp contrast to the Americas, with only 10% of the world disease burden but 37% of the global health workforce.90 It has been said that this inequity in the global health workforce represents the greatest impediment to health in sub-Saharan Africa. Ethiopia has one of the lowest doctors to population ratio with only 1600 doctors serving a population of 83 million and like other countries in Africa, has been plagued by high attrition rates of qualified staff and significant migration of health professionals, including pharmacists, nurses and laboratory technicians, to developed nations or local private organisations.91 The response from the Ethiopian health ministry in 2008 was a commitment to increase the number of practising doctors in the country by 9000 over the following 4 years.92 Incentives have been introduced for doctors alongside a targeted programme to improve primary healthcare resulting in a vast increase in the number of primary health workers. Similar country-led and country-specific interventions that seek solutions beyond the health sector are urgently required throughout the continent. The most pressing needs and urgent research priorities for RHD and CHD are summarised in table 2.
Crucial areas of further research, clinical practice and critical issues for congenital heart disease (CHD) and rheumatic heart disease (RHD) in Africa
The need for sufficient health workers to be trained, sustained and retained in sub-Saharan African countries cannot be overemphasised.
Cardiac surgery in Africa: role of continental (North-South) as well as South-South collaborations
Efforts to overcome the multiple barriers to cardiac surgery have resulted in humanitarian projects along two patterns: (1) transfer of children to receive cardiac surgical care abroad, either pro bono or at reduced fees or (2) visiting surgical teams. Both of these models have demonstrated successes;88 however these are not tenable long-term solutions. We now see a paradigm shift in terms of cooperation to improve access to cardiac surgery for congenital and acquired lesions in Africa.
Several new paediatric cardiac centres are currently funded by non-governmental organisations but run on a permanent basis in African countries. The Salam Centre for cardiac surgery in Sudan, managed by an Italian humanitarian organisation, is the only centre in central Africa offering a free-of-charge service for comprehensive cardiac services.89 Another important collaboration is that established in Cameroon.93–96 This project has been able to demonstrate its feasibility, while stressing the importance of human resource capacity building and a robust funding mechanism to achieve longevity and long-term sustainability.94
The Walter Sisulu Paediatric Centre for Africa in South Africa provided a continental referral centre, training surgeons who would then develop programmes in their own countries.5 As a result, the Ghanian National Cardiothoracic Centre (established in 1989), has been accredited by the West African College of Surgeons as a centre of excellence for the training of cardiothoracic surgeons, providing a much needed resource for West Africa, one of the poorest regions in the world.97 The Pan African Society of Cardiology is a platform which allows for development of these critical partnerships to serve all the children of Africa: thus far it has helped to establish links between African universities and institutions impacting on training, teaching and outreach.3
The final model is that of systematic programme development in order to build a long-term successful programme. Here the focus is on developing and strengthening local teams and the creation of pathways to sustainability. A commitment from all involved parties, including government is paramount. New cardiac programmes such as those established in Mozambique, Namibia and Uganda have adopted the approach of inclusivity and a carefully staged cardiac programme to ensure long-term success.1 Figure 2 depicts countries with established cardiac programmes performing at least 100 cases per year, providing training and in some cases, certification for cardiologists or cardiac surgeons. These numbers include surgery for congenital and acquired cardiac lesions in public and private units.

{kind=link}
{kind=link}
Countries with established cardiac surgery programmes.
Conclusions
Africa continues to carry the heavy burden of RHD in children and young adults while access to appropriate management of CHD, including simple defects, remains to be addressed. New data confirms a high prevalence of subclinical RHD in studies from Uganda, Senegal and Mozambique. The application of standardised criteria in follow-up reviews of children with subclinical RHD will be crucial in establishing the role of early echo-based detection of RHD. Primary prophylaxis of ARF may be a cost-effective prevention strategy in middle-income African countries. Although comprehensive prevention programmes (focused on early detection and treatment of RHD and CHD) are still lacking in most African countries, several critical partnerships have been established in the recent decade to facilitate improved management of those with congenital and acquired heart disease. Most importantly multisectoral and multidisciplinary platforms have given rise to new cardiac centres acting as continental centres of excellence, comprehensive integrated service frameworks and landmark research focusing on the African context.
References
Footnotes
Bongani Mayosi is the Guest Editor of this Cardiology in Africa review series.
-
Contributors LZ and EM prepared the first draft and edited all subsequent drafts. MM provided critical review of the first draft and then edited all subsequent drafts. EM prepared figure 1 and table 1 and LZ table 2 and figure 2. All authors contributed to the final submission and approved the final version.
-
Funding LZ is funded by the Thrasher Foundation, Clinical Infectious Diseases Research Initiative, University of Cape Town Medical Research Council of South Africa and the Hamilton Naki Clinical Scholarship Programme funded by Netcare Limited.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.